
Abstract
Villous adenoma is a rare pathology seen in the urinary tract; it is mostly found in the large bowel. When encountered in the urinary tract, it mainly originates from intestinal segments of urinary reconstruction. Villous adenoma is commonly seen in patients more than 50 years and has a male predominance. In the urinary tract, it has been reported in the urachus, bladder dome and trigone. A few cases of villous adenoma have been described in the literature. We report a case of primary villous adenoma in the remnant of the urachus and discuss the pathophysiology, investigation and management.
Case report
A 58-year-old female presented with one episode of painless visible haematuria and debris in her urine. She had no significant past urological or medical history and no history of urinary tract infections. Clinical examination was unremarkable. Urine microscopy showed microscopic haematuria, no evidence of urinary tract infection and negative cytology. Ultrasound of the urinary tract was unremarkable. Contrast-enhanced computed tomogram (CT) of the urinary tract showed a filling defect in the anterior wall of the bladder with normal upper urinary tracts and kidneys (Figure 1). Subsequent magnetic resonance imaging (MRI) confirmed the presence of a predominantly hyperintense, on the T2 imaging, and hypointense, on T1 imaging, extrinsic bladder abnormality with an intermediate to low signal irregular margin (Figure 2). Flexible cystoscopy showed a cystic lesion at the bladder dome with mucus discharging from a tiny round opening on the surface of this lesion (Figure 3).

Coronal view contrast-enhanced computed tomography (CT) of the pelvis demonstrating a heterogeneous cystic lesion involving the right anterolateral bladder wall. There is no associated lymphadenopathy or evidence of metastatic disease.

Axial view magnetic resonance imaging (MRI) T2 sequence showing an irregular cystic lesion, with a possible soft tissue component, at the right bladder dome measuring 4 ×2.5 × 2 cm with irregular mucosa and a small tract between the lesion and the bladder.

Cystoscopic examination demonstrating a cystic lesion in the bladder dome with normal overlying urothelium and a foramen discharging mucus.
She underwent partial cystectomy with good surgical margin for suspicious urachal tumour. An indwelling Foley’s urethral catheter was inserted post operatively for 2 weeks and was removed following a normal cystogram.
The specimen removed was a sac measuring 5 × 2.4 × 2.3 cm with a circular piece of bladder 18 mm in diameter at one end. A probe could be passed through this area into a cavity 32 mm long, the lumen containing mucoid material. Microscopic examination revealed a cavity lined with dysplastic columnar epithelium forming numerous villi (Figure 4). The features were those of a villous adenoma with low-grade dysplasia arising in urachal remnant, and dysplastic epithelium was apposed to muscularis propria but no invasion was noted. There was no evidence of malignancy; the margin of resection was free from dysplasia, the transitional epithelium showing no significant abnormality.
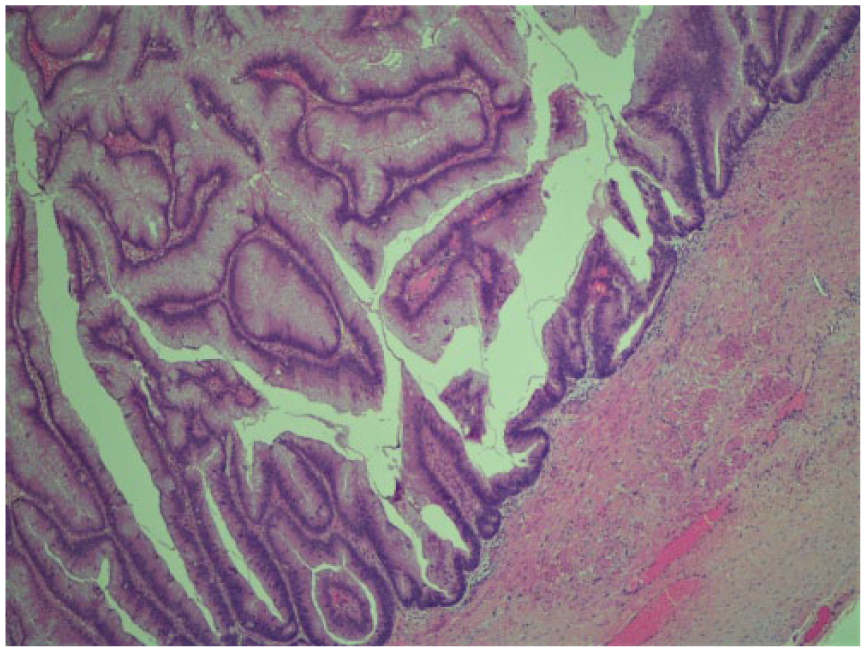
Histological examination. The sections show a cavity lined by dysplastic columnar epithelium forming numerous villi. The features are those of a villous adenoma with low-grade dysplasia. Dysplastic epithelium is apposed to muscularis propria but invasion is not identified. The margin of resection is free from dysplasia, the transitional epithelium showing no significant abnormality.
The case was discussed in our local multi-disciplinary team meeting, and as there was no associated adenocarcinoma, the patient was discharged without follow-up.
Discussion
Urachal villous adenoma of the bladder is rare and not commonly reported in the literature. Villous adenoma is mainly a disease associated with elderly male patients and the mean age of occurrence is the fifth decade.1,2
The urachus is a fibrous vestigial remnant of the allantois. It arises from the superior urogenital sinus; in the foetus, it connects the dome of the bladder and the allantois. 3 The pathogenesis of villous adenoma in the urinary bladder is speculative. The histopathology is similar to villous adenoma arising in the gastrointestinal tract. 1 Two theories have been proposed, and the first school of thought is of the opinion that villous adenoma may arise from proliferation into glandular neoplasm of the embryologic cloacal rest in the urinary bladder. An alternative theory suggests that villous adenoma is the product of a chronic irritation metaplasia–dysplasia–carcinoma sequence. 2
Villous adenoma of the urinary tract can be found arising from the kidney, ureter, bladder, or prostatic urethra. However, most of these arise from the intestinal segments of urinary reconstruction, including an Indiana pouch continent diversion, augmentation ileocystoplasty, cecocystoplasty and ureterocecal anastomosis. 4 When seen in the urinary bladder, villous adenoma has a predilection for the urachus, bladder dome and trigone. 5 Villous adenoma may be found in isolation or in association with adenocarcinoma in one-third to two-third of patients. 5
The clinical features of urachal villous adenoma are nonspecific and include haematuria, mucosuria, passage of debris in urine and storage lower urinary tract symptoms. Findings on cystoscopy and ultrasound scan are nonspecific. The findings on CT scan and MRI are also nonspecific and often are suggestive of malignancy. The diagnosis of bladder villus adenoma is usually on histological examination after surgery. 5
Management of urachal villous adenoma is partial cystectomy which could be done by open or laparoscopic surgery unlike the radical approach for invasive bladder masses. 5 A recent case report on robotic approach to resection of bladder villous adenoma has highlighted the advantages offered by this minimally invasive approach that is equally effective at achieving negative margins. 5
Although there is no consensus on follow-up for patients with villous adenoma of the bladder, with complete surgical excision with clear margins, villous adenoma has a good prognosis. There is no evidence in the English literature to suggest progression of disease to carcinoma. 5 The prognosis is poor if associated with adenocarcinoma as there have been a few cases reported in the literature where distant metastases have occurred years after primary surgery. 5
Conclusion
Villous adenoma is a rare tumour in the urinary tract with nonspecific clinical and radiological features. Diagnosis is mainly histological; therefore, a high index of suspicion is required. It is known to coexist with adenocarcinoma of the bladder in some cases; therefore, surgical excision with wide margins is recommended.
Footnotes
Acknowledgements
The authors would like to acknowledge Mr Hadi Salahia for his contribution for helping with the illustrations
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Ethical approval was not relevant or applicable to this case report. Written patient informed consent has been obtained.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.