
Abstract
A 70-year-old female suffered from gross hematuria and bladder tamponade. She had a solitary non-papillary tumor at the dome of the urinary bladder, underwent transurethral resection of the bladder tumor, and was diagnosed with an inflammatory myofibroblastic tumor positive for anaplastic lymphoma kinase proteins in immunohistochemistry. Subsequently, she underwent laparoscopic partial cystectomy using the Signia Stapling System due to the low-grade malignancy of the tumor. The patient has been under outpatient observation with no recurrence for 12 months post-surgery.
Keywords
Introduction
Inflammatory myofibroblastic tumor (IMT) is a rare tumor characterized by the growth of spindle-shaped cells and infiltration by inflammatory cells such as lymphocytes, plasma cells, and eosinophils. It commonly affects the lungs, gastrointestinal tract, liver, and bladder, and is slightly more frequent in females. IMTs are associated with a low risk of metastasis, and favorable outcomes can be achieved with treatments such as transurethral resection of bladder tumor (TURBT) or partial cystectomy, rather than radical cystectomy.1,2 They are often misdiagnosed as other malignant spindle cell tumors, leading to overtreatment. Diagnosis is supported by anaplastic lymphoma kinase (ALK) positivity in immunohistochemistry. 3 In this report, we present a case in which the diagnosis of IMT was confirmed by ALK positivity in a TURBT specimen, leading to the selection of partial over radical cystectomy.
Case presentation
The patient had a history of an overactive bladder and was taking vibegron for it. A 70-year-old female presented to another hospital with gross hematuria. The patient underwent a cystoscopy at the hospital. Cystoscopy revealed a solitary non-papillary tumor at the dome of the urinary bladder. Contrast computed tomography (CT) of the abdomen and pelvis revealed a 30-mm enhancing mass at the dome of the urinary bladder (Figure 1(a)). There were no findings suggestive of lymph node enlargement or multiple organ metastases. On the next day, the patient experienced worsening gross hematuria, suggesting the possibility of bladder tamponade. Consequently, she was transferred to our hospital and admitted to our department. She underwent TURBT and transurethral electrocoagulation (TUC) 3 days later. The tumor was located at the dome of the bladder, highly vascular, and macroscopically muscle-invasive. The tumor was partially resected by TURBT, and complete resection was not feasible. The rapid pathological diagnosis of TURBT showed tumor cells containing sarcoma components; however, this did not facilitate a definitive diagnosis. The patient’s hematuria improved, and she was discharged five days after surgery. Regarding permanent pathology, histopathological examination revealed a spindle cell tumor with nodular to radiating proliferation accompanied by inflammatory cell infiltration. The spindle cell tumor exhibited lymphocyte infiltration with mild cellular atypia and few mitotic figures. Immunohistochemical staining results indicated that the tumor cells were negative for Desmin and Myogenin, which are muscle markers, ruling out sarcoma. The tumor cells were also negative for the urothelial markers GATA3 and p40/p63, ruling out urothelial carcinoma. Positivity for ALK and Vimentin led to a diagnosis of IMT. The pathological specimens obtained by TURBT did not contain any muscle fibers. After a discussion with the pathology department, it was decided that total cystectomy was unnecessary due to the low-grade malignancy of the tumor, and so partial cystectomy was planned. Six weeks after discharge, contrast CT revealed that the tumor had increased in size from 30 to 60 mm. (Figure 1(b)) The tumor had pulled the bladder wall, including the muscle layer, toward the lumen, and the increased density of the surrounding adipose tissue suggested extravesical invasion. There were no findings suggestive of lymph node enlargement or organ metastasis. The patient underwent laparoscopic partial cystectomy using the Signia Stapling System (Medtronic plc., Minneapolis, MN, USA) eleven weeks after TURBT and TUC (Figure 2). According to the pathological diagnosis, the tumor exhibited vascular invasion and slight infiltration into subserosal tissue, but the resection margins were negative (Figure 3). The postoperative course has been uneventful, and the patient is being monitored as an outpatient, undergoing cystoscopy every 3 months (Figure 4) and CT scans every 6 months. No recurrence or metastasis has been observed even 12 months after the surgery.
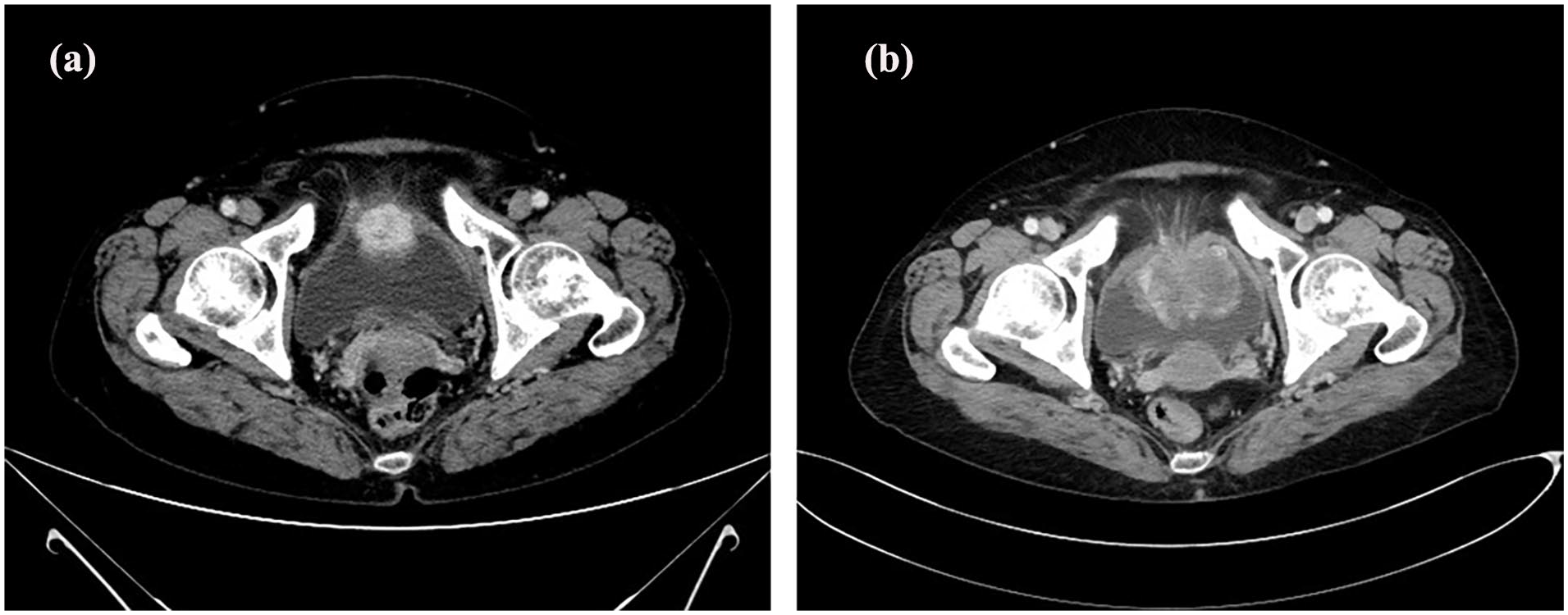
CT findings. (a) CT revealed a 30-mm enhancing mass at the dome of the urinary bladder. (b) Six weeks after diagnosis, CT revealed that the tumor had increased in size from 30 to 60 mm.

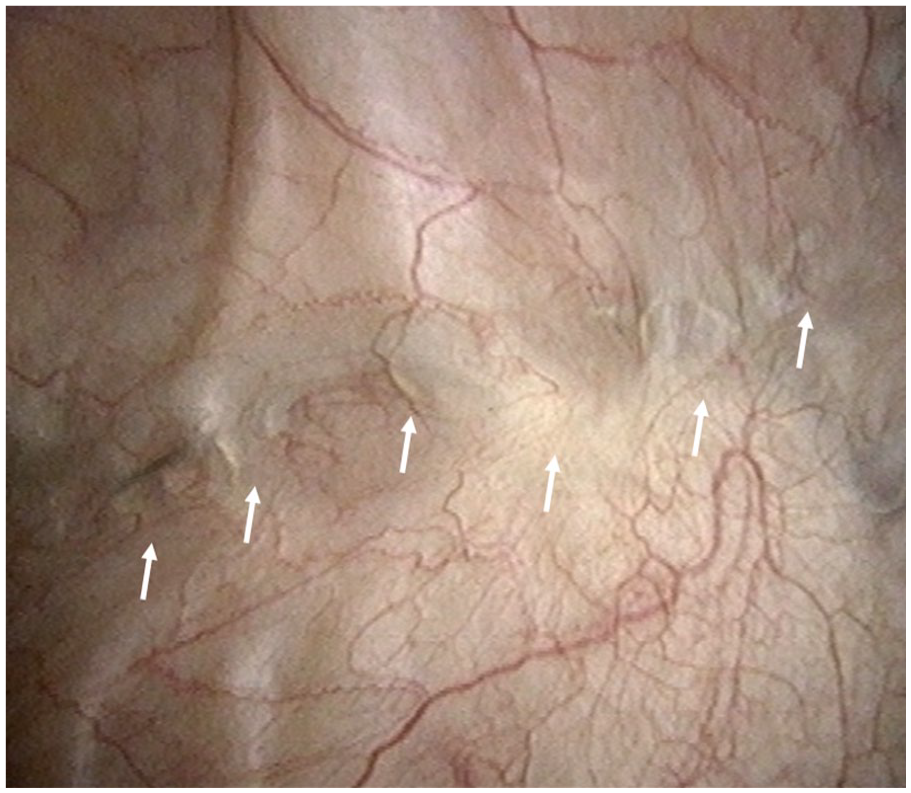
The view of laparoscopic partial cystectomy. By utilizing Signia Stapling System during partial cystectomy, surgery could be conducted without exposing tumor tissue to the surgical field. (a) tumor lesion of the bladder. (b) Normal bladder region.

Pathological findings. (a) Pathological examination with hematoxylin-eosin staining revealed spindle cell tumors growing in a nodular and radial pattern, accompanied by infiltration of inflammatory cells like lymphocytes. (arrow: vascular invasion). (b) A spindle cell tumor was observed, showing mild cellular atypia accompanied by lymphocytic infiltration and almost no mitotic figures. (c) Immunohistochemical staining results revealed that the tumor cells were ALK-positive, exhibiting a granular cytoplasmic pattern consistent with the CLCT-ALK fusion gene. (d) Tumor cells proliferating destructively in the bladder wall muscle layer were Desmin-negative.
Cystoscopic findings 3 months post-surgery.
Discussion
IMT is characterized by the proliferation of spindle-shaped cells, primarily fibroblasts and myofibroblasts, accompanied by the infiltration of inflammatory cells such as lymphocytes, plasma cells, and eosinophils. IMT is a tumor with a low frequency of metastasis and is predominantly found in the lungs, gastrointestinal tract, liver, and bladder. Epidemiological studies have shown that IMT slightly more frequently affects females.1,2 The incidence of IMT of the urinary bladder is currently unknown; however, Hage et al. reported 75 cases, with the average patient age being 36 years. 3 Differentiating IMT from malignant tumors, such as sarcomas, is critical for accurate diagnosis and appropriate treatment. IMT is associated with a low risk of metastasis. Given this characteristic, bladder-preserving treatments such as TURBT and partial cystectomy are reported to be the most common management strategies, rather than radical cystectomy. 2 Immunohistochemistry plays a significant role in diagnosing IMT, particularly with the expression of ALK being a helpful marker. According to a survey conducted by Hage et al., 68% of the 75 IMT cases tested positive for ALK. 3 The histological features of IMTs, which include predominant spindle cell proliferation, a pronounced chronic inflammatory component, low mitotic activity, and a lack of tumor necrosis, can assist in excluding other differential diagnoses. It is crucial to distinguish bladder IMTs from leiomyosarcoma and sarcomatoid carcinoma. Leiomyosarcoma and sarcomatoid carcinoma are ALK-negative, while the diagnosis of ALK-positive IMT is relatively straightforward and often results in bladder-preserving surgery. However, differentiating ALK-negative IMT cases from leiomyosarcoma and sarcomatoid carcinoma can be challenging. In our case, the inflammatory findings in the transurethral resection specimen were relatively mild. If the ALK proteins had not tested positive, it would have been challenging to pathologically diagnose this case as IMT based solely on the transurethral resection specimen prior to radical surgery. However, the presence of ALK positivity in immunohistochemistry confirmed the diagnosis of IMT, allowing for partial rather than radical cystectomy in this case. Therefore, it can be extremely challenging to distinguish ALK-negative bladder IMT cases from leiomyosarcoma or sarcomatoid carcinoma using tissue obtained through TURBT. As a result, radical cystectomy may be required. Due to the limited number of reported cases, it is challenging to determine the degree of biological malignancy between ALK-negative and ALK-positive cases.
In this case, imaging evaluations indicated invasion beyond the bladder wall, making it impossible to achieve a curative outcome with TURBT. In addition, because the pathology of IMT indicates that the risk of distant metastasis is extremely low, partial cystectomy was selected as a bladder-preserving surgical option. Furthermore, due to concerns regarding the potential for local recurrence resulting from tumor exposure in the surgical field during the IMT procedure, we performed a partial cystectomy utilizing a stapling system to prevent tumor exposure during the surgery. In this case, the use of the stapling system during partial cystectomy allowed the surgery to be conducted without exposing tumor tissue to the surgical field. However, concerns regarding potential complications, such as stone formation, arise when the non-absorbable metal components of the stapler used in the system become exposed within the bladder. Nevertheless, follow-up observations confirmed that the stapler remained unexposed inside the bladder and was instead covered by the mucosa (Figure 4). In this case, a partial cystectomy was successfully performed because the tumor was solitary and located at the dome of the bladder. However, the procedure may become challenging depending on the tumor’s location or the presence of multiple tumors.
It is important to note that ALK-negative IMT cases have also been reported, suggesting heterogeneity within the disease. 2 Treatment outcomes for IMT have shown variability, with some reports indicating tumor reduction or complete remission achieved through the use of corticosteroids and nonsteroidal anti-inflammatory drugs.4,5 IMT encompasses a range of disease presentations, and there is a possibility that this tumor group may be further subdivided in the future as our understanding of its pathogenesis and clinical behavior advances.
Conclusion
We presented a case with a diagnosis of IMT confirmed based on ALK positivity, leading to partial cystectomy using the Signia Stapling System due to the low-grade malignancy of the tumor. IMT encompasses a wide range of diseases, and it is likely that this group of tumors will be further subdivided in the future as our understanding of the pathogenesis and clinical behavior progresses.
Footnotes
Acknowledgements
This research project received no specific grant from funding agencies in the public or commercial sectors.
Author contributions
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient for the publication of this case report and accompanying images.