
Abstract
Presacral myelolipomas are rare, benign, asymptomatic tumors composed of mature adipose tissue and hematopoietic elements. Presacral myelolipomas can occur in patients with a medical history of malignancy, steroid use, and/or endocrine disorders including diabetes mellitus. A 65-year-old man with no specific medical history experienced temporal abdominal pain without bowel symptoms that lasted a few hours. By the time he visited a hospital, the pain had diminished. Computed tomography failed to detect any abnormality in the abdominal or pelvic organs that would have caused the abdominal pain but revealed a lesion 4 cm in diameter in the frontal sacrum. Magnetic resonance imaging showed that the lesion contained fat elements with a high signal intensity on T1- and T2-weighted images, which was decreased on fat-suppression T2-weighted images. Computed tomography–guided biopsy and imaging allowed a diagnosis of presacral myelolipoma. After 3 months, hematochezia was observed, and follow-up examination revealed rectal carcinoma with multiple lung metastases. He died due to spread of the cancer despite chemotherapy, 6 months after the cancer was found. Considering the possible association between presacral myelolipoma and cancer, presacral myelolipoma might be a cancer parasymptom. Checking for possible malignancy may therefore be warranted in patients with presacral myelolipoma, especially in those without diabetes mellitus.
Introduction
Myelolipomas are benign tumors composed of fat tissue with extramedullary hematopoietic elements that most commonly occur in the adrenal glands. 1 Myelolipomas may rarely occur in extra-adrenal locations; over half of these cases are located in the presacral region and are thus called presacral myelolipoma.2–4 In a review of extra-adrenal myelolipomas, a medical history of diabetes mellitus, cancer, and steroid use was observed in 22%, 19%, and 16% of patients, respectively. 4 In the present case, presacral myelolipoma was found incidentally, and rectal carcinoma was discovered 3 months later due to hematochezia. Considering its possible association with cancer, myelolipoma might be a cancer parasymptom.
Case report
A 65-year-old man who did not have a history of cancer or endocrine disorders, including diabetes mellitus, experienced acute-onset abdominal pain without a trigger, such as eating or drinking. The pain was mild, and it was not accompanied by bowel symptoms. The pain had diminished by the time he visited a hospital. Ultimately, the pain had lasted a few hours. On physical examination, his abdomen was soft without tenderness. There was no palpable mass. No edema was observed in the lower extremities. Fever was not present. Laboratory data revealed no anemia, mineral imbalance, inflammation, or diabetes mellitus; values with institutional normal limits in parentheses were: hemoglobin, 14.8 (13.5–17.5) g/dL; sodium, 145 (138–146) mEq/L; potassium, 3.9 (3.6–4.9) mEq/L; calcium, 9.3 (8.7–10.3) mEq/L; phosphate, 3.7 (2.5–4.7) mEq/L; C-reactive protein, 0.46 (0–0.3) mg/dL; and HbA1c, 5.0% (4.6–6.2%).
Previously, screening computed tomography (CT) of the abdomen and pelvis had not yielded specific findings, and no disease was suggested on physical examination. CT images identified a 4 × 4 × 3 cm mass in front of the third to fifth sacral (S3-S5) vertebrae. The CT value of the lesion indicated heterogeneity. The average CT value was −1.08 HU (Hounsfield Units); the low CT value area ranged from −20 to −40 HU, consisting of the fat component, while the other rather high values ranged from 0 to 10 HU. No destruction of the adjacent sacral vertebra was seen (Figure 1(a)). No other apparent abnormalities in abdominal and pelvic organs were observed.

Presacral myelolipoma: (a) CT images show a presacral mass at S3-S5—top and middle, soft-tissue windows (width = 250, center = 30); bottom, bone windows (width = 2000, center = 400). The tumor has lobulated contours and a heterogeneous appearance, containing low CT values (−20 to −40 HU) suggesting fat tissue. MRI shows a lobulated lesion with heterogeneous low to high signal intensity on T1-weighted (top) and T2-weighted (middle) images. The degree of suppression on T2-weighted fat-suppression images is low but visible (bottom) ((b) sagittal, (c) axial).
On magnetic resonance imaging (MRI), the lesion appeared to be heterogeneous with intermediate to high signal intensity on T1- and T2-weighted images and was lobulated by septae with low signal intensity on T1-weighted images (Figure 1(b) and (c)). A low degree of suppression at high signal intensity on T2-weighted fat-suppression images was observed (Figure 1(b) and (c)). CT-guided biopsy was performed, in which the biopsy needle reached the lesion through the paraspinal muscle, thereby not involving the vertebral body. Histologic analysis showed predominant mature adipose tissue intermixed with extramedullary hematopoietic components. The diagnosis was extra-adrenal myelolipoma, or presacral myelolipoma, because there was no chance of bone marrow tissue contamination in the specimen (Figure 2).
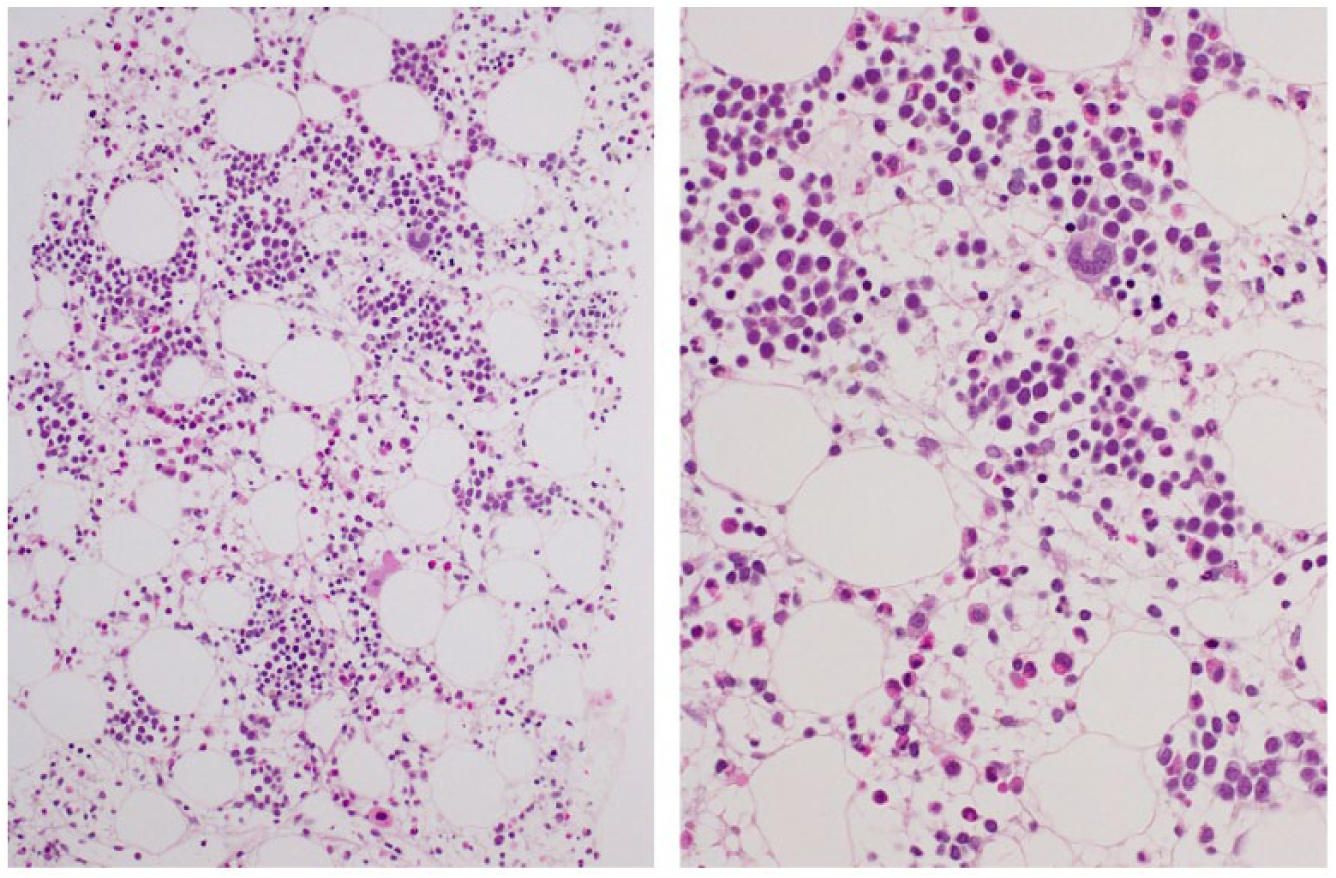
Presacral myelolipoma. Histopathologic analysis shows predominantly mature adipose tissue intermixed with extramedullary hematopoietic components (H & E staining; original magnification; left ×20, right ×40). There is no intra-tumoral hemorrhage.
The abdominal pain disappeared without treatment, and the association between the abdominal pain and presacral myelolipoma was inconclusive. The presacral myelolipoma was assumed to be asymptomatic due to its small size. Considering its benign nature, a treatment strategy of observation, not resection, was chosen. CT follow-up imaging was planned to check for possible enlargement every 6 months. Three months after the initial assessment, the patient noticed hematochezia. Digital rectal examination and other assessments identified a well-differentiated rectal adenocarcinoma, with multiple lung metastases (T3A, N0, M1b; stage IVB). Because resection of the cancer was not expected to improve the prognosis, chemotherapy consisting of bevacizumab plus mFOLFOX3 (oxaliplatin, leucovorin, and 5-fluorouracil) was administered. Despite chemotherapy, the patient died due to the spread of the cancer 6 months after hematochezia was first noticed.
Ethical approval was not sought for this study because the study is a retrospective case report, showing medical information of patient with specific disease. This study was completed in accordance with the Helsinki Declaration as revised in 2013.
Verbal informed consent was obtained from the patient before the study. Written informed consent was not obtained, but the patient was informed that the data from the case would be de-identified and used in a journal publication along with a written statement confirming that consent to use their data was provided by them verbally.
Discussion
Myelolipomas are characterized by fat and myeloid components. 1 Extra-adrenal myelolipoma is a tumor of the adrenal gland. A review of extra-adrenal myelolipomas revealed that they are most commonly found in the presacral region, followed by the retroperitoneal, thoracic, and pelvic regions. 4 Presacral myelolipomas are generally diagnosed in elderly patients, usually between the fifth and seventh decades of life, with a female predominance.2–4 Symptoms are directly related to tumor dimensions. 5 Small lesions are usually asymptomatic, although patients may complain of urinary retention, constipation, or lower extremity radiculopathy.3,4,6 In this case, the association between the temporal abdominal pain and the presacral myelolipoma was not conclusive because the lesion was small.
Presacral myelolipomas appear as generally well-circumscribed, heterogeneous, predominantly fat-containing masses. 7 Variable amounts of fat tissue accompanied by hematopoietic soft-tissue elements reflect the images. Myelolipoma appearance on CT also depends on the composition of the lesion.8,9 The attenuation value of fat in myelolipomas has been reported to be lower than 20 HU, but it is usually higher than that of retroperitoneal fat because of the admixture with hematopoietic tissue.10,11 In the diagnosis of myelolipoma, MRI is able to depict the presence of the fat component with high signal intensity on T1-weighted and T2-weighted images and is suppressed on fat-suppressed T1-weighted images.5,12 In addition, hematopoietic elements usually exhibit low signal intensity on T1-weighted sequences and intermediate signal intensity on T2-weighted sequences.5,10 In our case, the degree of fat suppression was low. But the degree of the fat suppression would be affected by intra-tumoral hemorrhage, 12 though the small sample from the current CT-guided biopsy failed to provide evidence of intra-tumoral hemorrhage. The differential diagnosis of fat-containing neoplasms in the presacral region includes liposarcoma, teratoma, extramedullary hematopoiesis, and neurogenic tumor. 9
For precise diagnosis of presacral myelolipoma, biopsy is necessary. However, the location of these lesions makes biopsy relatively difficult. 7 Diagnostic procedures, such as CT-guided percutaneous fine-needle aspiration biopsy or frozen sectioning, have been reported be useful in diagnosis. 8 In the present case, CT-guided needle biopsy was successfully performed, allowing a diagnosis of presacral myelolipoma. The biopsy needle reached the lesion via the paraspinal muscle. In cases of malignancy, the lesion at the distal sacrum would be resected by a posterior approach. Therefore, though there is a risk of seeding of neoplastic cells along the biopsy needle tract, the contaminated biopsy tract could be resected as well. In particular, in the diagnosis of myelolipoma, the paraspinal approach was able to exclude contamination of bone marrow tissue, because the vertebral body was not involved. Surgery remains the treatment of choice for symptomatic presacral myelolipomas. 9 In a previous report, presacral myelolipoma was subjected to surgical resection to rule out malignancy. 7 However, considering the benign nature of presacral myelolipoma, non-surgical observation is supported for asymptomatic lesions.
The etiology of both adrenal and extra-adrenal myelolipomas remains unknown. 8 Cytogenetic abnormalities reported for adrenal myelolipomas have included t(3;21)(q25; P11) 13 and X-chromosome inactivation, 14 suggesting a neoplastic nature of the lesion. However, no cytogenetic abnormalities have been reported in extra-adrenal myelolipomas. Non-neoplastic adrenal and extra-adrenal myelolipomas have been proposed to arise from reactivation of peritoneal connective tissue hematopoiesis or embolization of bone marrow tissue.9,12 Endocrine dysfunction could also be a cause of adrenal and extra-adrenal myelolipomas, as associations with diabetes, Cushing syndrome, Addison disease, adrenal hyperplasia, and chronic steroid intake have been reported.4,5,7,9 As noted earlier, extra-adrenal myelolipomas have been reported to be accompanied by diabetes mellitus, cancer, and steroid use in 21.6%, 18.9%, and 16.2% of patients, respectively. 4 Extra-adrenal myelolipoma has been reported to be associated with breast cancer8 and bladder cancer5, as well as with colon cancer, 15 as in our case.
Conclusion
The current patient had a rare case of presacral myelolipoma. After the myelolipoma finding, rectal cancer was identified. Considering the presence of cancer in this patient, myelolipoma might be a parasymptom of cancer. Cancer screening may therefore be warranted in patients with myelolipoma, especially for those without endocrine disorders such as diabetes mellitus.
Footnotes
Acknowledgements
A.S. drafted the manuscript. A.S. and I.N. were in charge of the treatment. E.S. and M.H. are pathologists and were in charge of the pathological diagnosis. T.O. and S.M. participated in its design and coordination, and helped to draft the manuscript. All authors read and approved the final manuscript.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.