
Abstract
Choroidal metastatic tumours from gastric cancer (GC) are rare compared with breast and lung cancer. Here, we report a patient with GC who presented to our ophthalmology clinic with a one-week history of left eye visual disorder and pain. Fundoscopic and B-scan examinations suggested a choroidal metastatic tumour. Computed tomography (CT) and magnetic resonance imaging (MRI) scans confirmed our initial diagnosis. Histopathology and immunohistochemical findings showed the tumour most likely originated from the gastrointestinal tract. Although the patient was well after eye removal, he died two months after surgery. Metastasis of GC should be a consideration when a patient with a history of GC presents with eye pain, decreased vision, and/or high intraocular pressure.
Background
Metastatic tumours are the most common type of intraocular malignancy. 1 The primary cancers that most commonly lead to choroidal metastases are breast and lung.2,3 However, choroidal metastases arising from gastric cancer (GC) are rare.4–8 In a survey of 520 patients with GC, choroidal metastasis was found in only 4% patients. 4 Choroidal metastases tend to occur late in the course of cancer, and are associated with a poor prognosis.9,10 Therefore, it is critically important to identify ocular metastases early since primary treatment can significantly affect patients’ survival. We report here, a patient with GC who presented with a visual disorder, eye pain, and ocular hypertension in his left eye and we also briefly summarize and discuss related case studies.
Case report
A man in his late 50s presented to our hospital with a one-week history of pain in his left eye with accompanying visual disorder. Twelve months previously, in another hospital, the patient had undergone 18F-fluorodeoxyglucose-positron emission tomography/computed tomography (18F-FDG-PET/CT) and gastric biopsy via esophagogastroduodenoscopy. His scans had shown multiple bone metastases, irregular thickening of the gastric wall in the corner area, and an abnormal increase of FDG metabolism (Figure 1a). The esophagogastroduodenoscopy showed new organisms with irregular ulceration in the middle and anterior wall of gastric antrum (Figure 1b). The posterior wall of the anterior region of the pylorus showed a small polypoid eminence with smooth surface. A moderately differentiated tubular adenocarcinoma was diagnosed by gastric biopsy specimen via esophagogastroduodenoscopy (Figure 1c). The patient had been diagnosed as having stage IV GC with multiple metastases. Instead of surgery, the patient had undergone systemic chemotherapy with oxaliplatin (85 mg/m2, once a day, for 21 days) and cetuximab (250 mg/m2 every three weeks).

(a) A 18F-fluorodeoxyglucose-positron emission tomography/computed tomography (18F-FDG-PET/CT) scan showed irregular thickening of gastric wall in the corner area and an abnormal increase in FDG metabolism. The red arrows indicate two lymph nodes in the lesser curvature of the stomach. (b) Esophagogastroduodenoscopy showed new organisms with irregular ulceration in the middle and anterior wall of gastric antrum and (c) Results of a biopsy showed a moderately differentiated tubular adenocarcinoma (haematoxylin and eosin staining; magnification ×100).
To identify the cause of the patient’s recent visual disorder and pain, we performed fundoscopic examinations and ophthalmologic examinations in the ophthalmology department at our hospital. A fundoscopic examination of his left eye showed retinal detachment, conjunctival oedema and hyperaemia, combined with subretinal haemorrhage; these signs suggested a choroidal metastatic tumour (Figure 2a). Ophthalmological examination of the same eye showed an intraocular pressure of 14 mmHg oculus dextrus and 50 mmHg oculus sinister. His right eye was unremarkable. B-scan ultrasonography showed a mass in the ball of the left eye, vitreous haemorrhage, and exudative retinal detachment (Figure 2b).

(a) Fundoscopic examination of the left eye showed retinal detachment, conjunctival edema and hyperaemia, combined with subretinal haemorrhage, which suggested a choroidal metastatic tumour. (b) B-scan ultrasonography showed a mass in the ball of the left eye, vitreous haemorrhage, and exudative retinal detachment. (c) Computed tomography (CT) scan showed an enhanced mass at the nasal and posterior sides of the left eye (white arrow). (d) T1-weighted image showed iso-intensity with enhancement (white arrow) and (e) T2-weighted image showed hypointensity (white arrow).
The results of laboratory tests showed that several tumour markers were elevated these included: alpha-fetoprotein (AFP), 692 µg/l (normal range, 0–20 µg/l); carcinoembryonic antigen (CEA), 162 µg/l (normal range, 0–5 µg/l); CA-125, 103 kU/l (normal range, 0–35 kU/l); CA153, 101 kU/l (normal range, 0–45 kU/l); CK19, 169 µg/l (normal range, 0–3.3 µg/l).
Orbital computed tomography (CT) (Figure 2c) and magnetic resonance imaging (MRI) showed an enhanced mass on the nasal and posterior side of the choroid in the left eyeball. The lesion presented as hypointense and isointense areas on T1- and T2-weighted images, respectively (Figure 2d–2e). The patient’s right eye was unremarkable. These diagnostic results suggested that the tumour was a metastatic lesion rather than a melanoma.
Surgery was performed to remove the patient’s left eyeball. A nasal-posterior solid neoplasm was found in the dissected eyeball with a massive haematocele (Figure 3a). Pathology results showed a metastatic and moderately differentiated (papillary) adenocarcinoma with extensive necrosis (Figure 3b). Periodic acid-Schiff staining showed a positive mucinous secretory material within gland-like structures (Figure 3c).
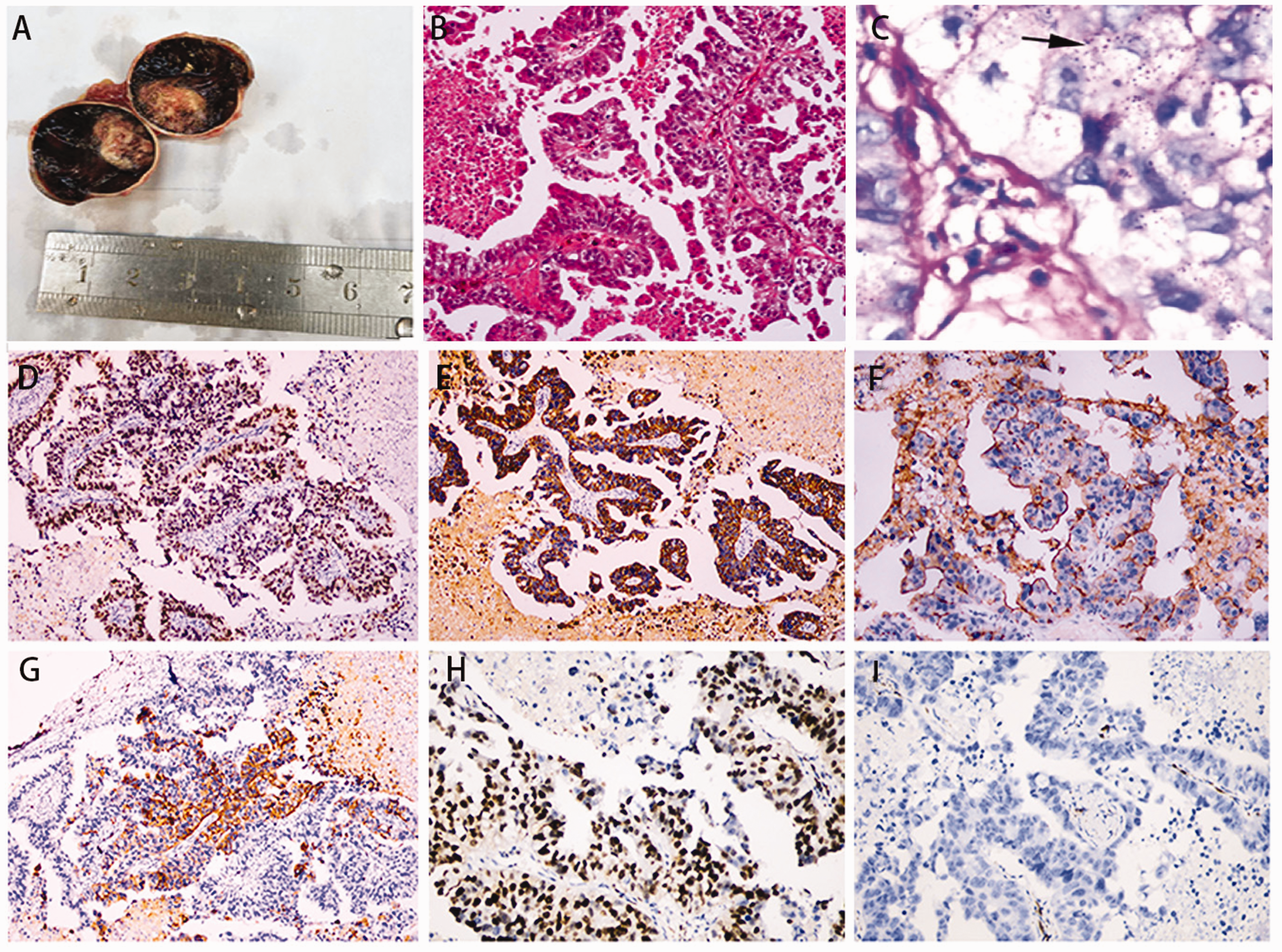
(a) The dissected eyeball, along with a massive haematocele. (b) The removed eyeball showing a poorly differentiated tubular adenocarcinoma (haematoxylin and eosin staining; magnification × 100). (c) Periodic acid-Schiff (PAS) staining showed tumour cells containing a large amount of mucin. The black arrow shows a positive mucinous secretory material within gland-like structures (magnification ×4 00). (d) Using immunohistochemistry antibody expression of CDX2 was positive (magnification × 100). (e) Using immunohistochemistry antibody expression of CK19 was positive (magnification×100). (f) Using immunohistochemistry antibody expression of Muc-1 was positive (magnification × 200). (g) Using immunohistochemistry CK20 stain showed weak positivity in <20% of cells (magnification × 100). (h) Using immunohistochemistry antibody expression of Ki67 was positive (magnification ×200). and (i) Using immunohistochemistry antibody expression of CK7 was negative (magnification ×200).
To distinguish between primary and metastatic tumours, immunohistochemistry was performed and results showed that the tumour cells were positive for the following tumour markers: CDX2; CK19; Muc-1; CK20 (weak); Ki67. However, immunostaining for CK7 was negative (Figures 3d–3i). These findings together with patient’ previous medical history suggested that the tumour cells had most likely arisen from the gastrointestinal tract. A diagnosis of choroidal metastasis originating from GC was made. Following his surgery, the patient recovered well and was relieved of his eye pain. Unfortunately, he died two months after surgery.
The reporting of this study conforms to CARE guidelines. 11 Written informed consent to publish the patient’s anonymised data was obtained from his family. The study was approved by our Hospital Ethics Committee.
Discussion
Due to its abundant vascular supply, the choroid is the most common ocular site of metastasis. 2 With cancer rates rising and diagnostic methods and treatments improving, reports of metastatic choroidal tumours are increasing. 2 At initial diagnosis, choroidal metastases need to be differentiated from choroidal melanoma, haemangioma, granuloma, osteoma, and sclerochoroidal calcification. 12 Moreover, since choroidal metastases tend to become apparent late in the course of the malignancy, they are associated with poor prognosis.9,10,12 Typical symptoms of metastases of the choroid are blurred vision (70–81%), pain (5–14%) and flashes and floaters (5–12%). 12 However, up to 20% of patients are non-symptomatic and metastases are discovered on routine examination or during a systemic evaluation of a generalized cancer. 2
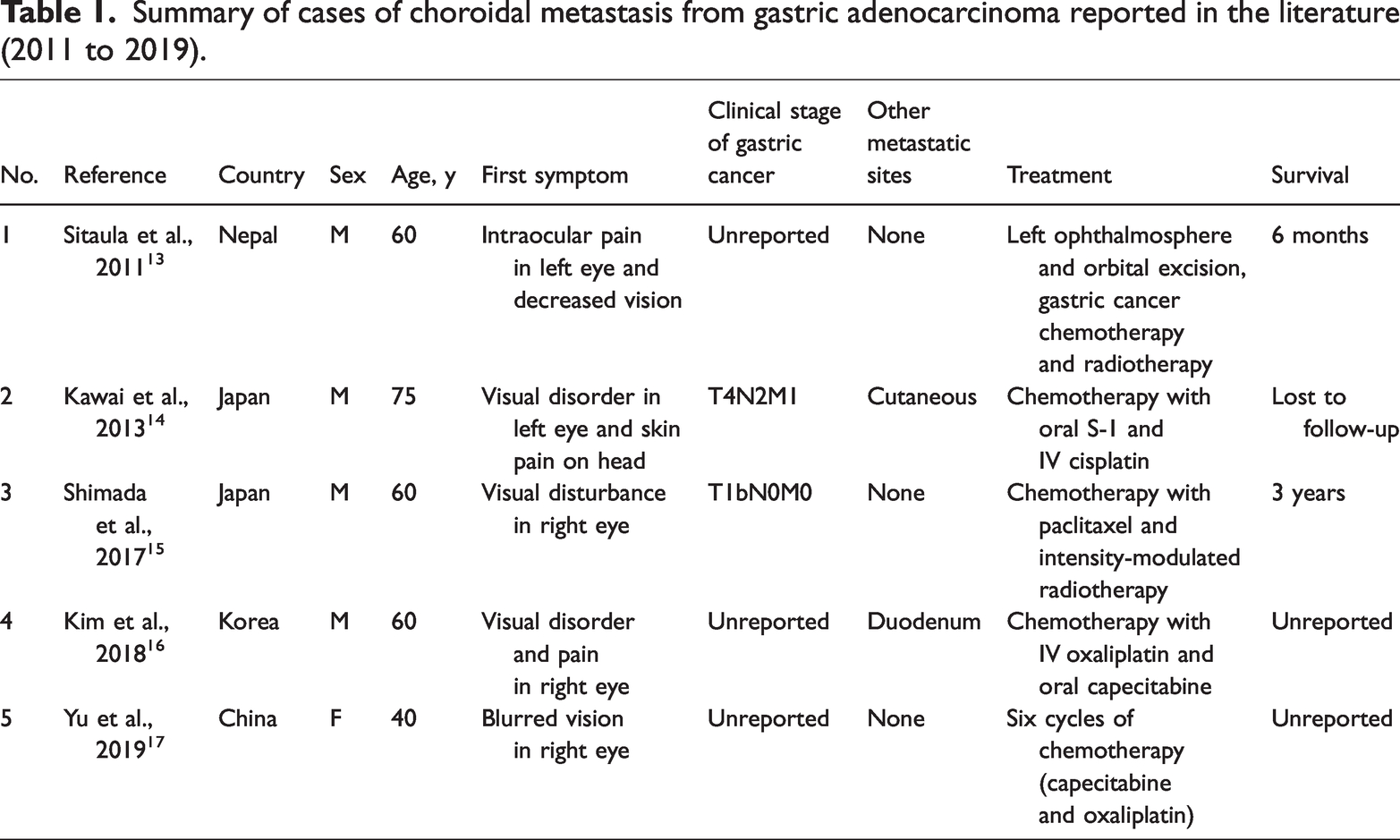
The most common primary tumours in patients with choroidal metastases are breast cancer (40–53%) and lung cancer (20–29%). 12 Metastatic ocular tumours that originate from the gastrointestinal tract are rare.4–8 In our current report we describe the diagnosis of choroidal metastasis originating from GC. Following eye removal surgery, the patient was relieved of pain and recovered well. However, he died two months later which was probably related to his metastatic GC. From a review of published studies between 2011 and 2019, we identified only five other case reports of choroidal metastases from GC (Table 1).13–17 Two reports were from Japan, and one each from China, Korea and Nepal. Four patients were male and one female and ages ranged from 40 to 75 years. Symptoms were consistent with previous findings (i.e., pain, visual disorder and blurred vision). Treatments included eye removal and/or chemotherapy/radiotherapy for GC. Only two studies reported on outcomes (one six months, the other three years). Our survey of published literature over a 10-year period emphasises the rarity of this condition.
Summary of cases of choroidal metastasis from gastric adenocarcinoma reported in the literature (2011 to 2019).
For patients with suspected metastatic tumours, CT and MRI scans have a major role in the diagnosis and evaluation of local invasion and distant metastasis. Orbital MRI is useful for the differential diagnosis of choroidal masses. 18 Metastatic tumours are characterized by subretinal masses with a clear boundary, and present as an isointense signal on T1-weighted image and as a hypointense signal on the T2-weighted image. 12 In the case presented here, we made a preliminary diagnosis based on the patient’s medical history, results of CT and MRI scans of the patient’s orbits, and histopathological findings. We confirmed our diagnosis with immunohistochemical findings. Biopsy specimens were positive for tumour markers, CK19, CDX2 and Muc-1, which suggested the tumour cells had originated from the digestive tract.
In summary, although uncommon, choroidal metastatic tumours can arise from gastric adenocarcinoma. Therefore, a complete ocular examination should be performed if patients with a history of GC present with visual symptoms, since choroidal metastases from the primary site should be a consideration.
Footnotes
Acknowledgements
We wish to thank Qiu-Shi Li for images of the fundoscopic and B-scan examinations.
Declaration of conflicting interests
The authors declare that there are no conflicts of interest.
Funding
This study was supported by the Zhejiang Province Science and Technology Planning Project for Medicine and Healthcare (no.2023KY971).