
Abstract
Introduction
Schwannomas (Neurilemmoma) are benign nerve sheath tumors composed of Schwann cells. These can occur on the surface of any peripheral nerves and account for approximately 5% of all benign soft tissue tumors.1,2 The presentation of these tumors in the foot is rare, with most cases reporting their occurrence on the plantar aspect of the foot. 3 Dorsal involvement is rare and can present significant diagnostic challenges due to overlapping features with other soft- tissue masses, such as neurofibromas, pilomatrixomas, and even malignant tumors. 4
These lesions are typically encapsulated and slow-growing, which may have been presented for at least one to 2 years. Most lesions are asymptomatic, and if they become symptomatic, their clinical presentation depends on the size, location, and proximity of the tumor to adjacent structures.1,5 In the foot, where space is limited and functional demands are high, small lesions may cause discomfort or impair ambulation. Imaging studies, including ultrasound (US) and Magnetic Resonance Imaging (MRI), are often employed to evaluate these masses, but the findings are not always pathognomonic. Schwannomas may share imaging features with pilomatrixomas, neurofibromas, and other benign or malignant lesions, leading to diagnostic uncertainty. 6 As this case highlights, definitive diagnosis often requires histopathological confirmation following surgical excision.
This report describes a rare case of a schwannoma on the dorsum of the foot that had been present for 50 years before the patient sought medical attention. It discusses in detail the clinical presentation, imaging findings, histopathological features, and diagnostic and therapeutic challenges associated with this atypical presentation.
Case presentation
A 69-year-old male with a past medical history of well-controlled diabetes mellitus (DM) and hypertension (HTN), No family history of neurofibromatosis or congenital conditions diseases, presented to our clinic with a chief complaint of a gradually enlarging soft tissue mass on the dorsum of his right foot over the past 50 years. He denied any history of recent foot trauma. The lesion is associated with pain and affects his ambulation. He denied any history of numbness or electric sensation. Clinical examination revealed a mobile lesion over the dorsum of the right foot at the second web space. The mass was non-tender and not adherent to the underlying tissue. There was bluish discoloration with varicose veins on the overlying skin, with intact distal neurovascular examination of the foot (Figure 1). Clinical photograph of the right foot showing the presence of a soft tissue lesion on the dorsum of the 2nd web space.
Ultrasound examination of the mass demonstrated a lesion measuring approximately 40 x 14 mm within the subcutaneous tissue on the dorsum of the 2nd web space, with tiny calcifications. Doppler imaging showed increased vascularity in the peripheral region (Figure 2). Further evaluation of the mass with MRI showed a well-defined, oval-shaped, lobulated mass demonstrating marginally low signal intensity, measuring approximately 29 x 13.4 x 42.5 mm in its transverse, anteroposterior, and craniocaudal dimensions, respectively, at the dorsal aspect of the second and third metatarsal heads, extending to the skin surface and in contact with the second extensor tendon. On T1-weighted images, the mass exhibits intermediate signal intensity with small regions of fat signal at both the periphery and central region, while showing heterogeneous signal characteristics on Short Tau Inversion Recovery (STIR) and T2-weighted sequences. Post-contrast imaging revealed heterogeneous enhancement and peripheral diffusion restriction, suggestive of a schwannoma of the peripheral nerve (Figure 3). (a) US of the right foot demonstrating a soft tissue mass in the subcutaneous tissue in the dorsal aspect, measuring 40x14 mm; (b) Doppler shows increased vascularity more in the peripheral area with tiny calcification seen within the mass. Sagittal MRI of the lesion in the foot. (a) T1-weighted fat-suppressed image with contrast; (b) T2-weighted image.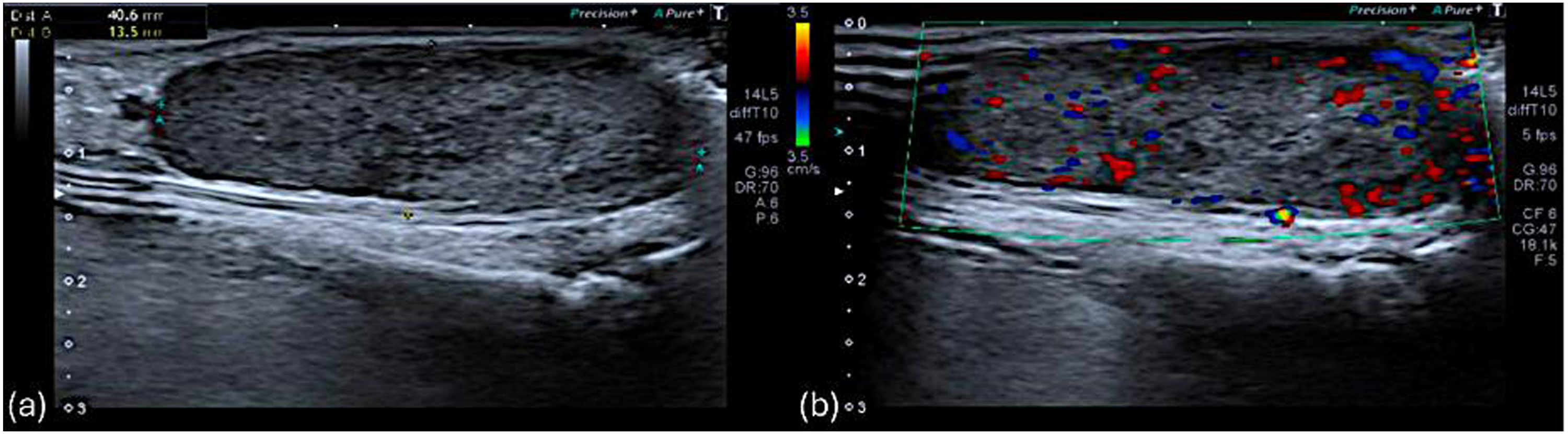

Following a multidisciplinary team (MDT) meeting, the decision was to proceed with excision of the mass for histopathological evaluation. The patient was admitted to the hospital electively and then underwent surgical excision of the lesion. No intraoperative or immediate postoperative complications occurred. Histopathological examination revealed features consistent with a schwannoma.
After the surgical excision, the patient was discharged home the following day and given a routine follow-up appointment in the orthopedic tumor clinic. Two weeks following the procedure, the patient was seen in the clinic for wound inspection. The wound was healed completely, with no signs of infection. Unfortunately, the patient was complaining of numbness at the surgical site. However, the power in the foot and toes was normal. The patient did not have any problems with gait. He was followed up for 2 months after the procedure and had no new complaints, so he was discharged from the clinic.
Discussion
Schwannomas are benign encapsulated tumors arising eccentrically from peripheral nerves, sparing the nerve axons. These foot lesions are rare and tend to involve large peripheral nerves.7,8 While schwannomas are rare in the foot, the plantar location of these tumors is more common than the dorsal.9,10 Pain is reported in approximately half of schwannoma cases and is typically due to either compression of adjacent tissues or irritation of the originating nerve. 3 Despite the lesion’s proximity to the extensor tendon, the absence of Tinel’s sign or paraesthesia in this patient further highlights the variable clinical presentations of schwannomas.
Preoperative radiological evaluation is critical but sometimes insufficient for a definitive diagnosis. US examination of schwannomas typically shows a round, hypoechoic, homogenous mass with clear margins, which is non-specific. 11 However, MRI is considered the gold standard for evaluating soft-tissue tumors; it provides more detailed information about the lesion’s characteristics. 12 Schwannomas are generally encapsulated, lobulated masses with heterogeneous signal intensities and peripheral enhancement on post-contrast imaging. 13 The findings in this case were consistent with the typical imaging features of the lesion on MRI, including iso-to-hyperintense (compared to muscle) on T1-weighted images, hyperintense on fluid-sensitive sequences, and often diffusely enhancing on contrast-enhanced images. 14
Differential diagnosis includes pilomatrixomas, which are derived from hair follicle matrix cells. These benign adnexal tumors commonly occur in the head and neck region. Still, they can also present in unusual locations such as the foot. 15 Neurofibromas, another differential diagnosis, are benign nerve sheath tumors but differ from schwannomas in their diffuse growth pattern and lack of a true capsule. They are more commonly associated with neurofibromatosis type 1 (NF1) and are less likely to displace nerves eccentrically. 16 These features make neurofibromatosis less likely to be the diagnosis in our case. This case illustrates the diagnostic difficulty posed by overlapping imaging findings. Although the calcifications and vascularity in the US initially suggested pilomatrixoma, MRI and histopathological examination were essential to confirm the diagnosis of schwannoma.
The definitive treatment for schwannomas is observation; however, when the patient is symptomatic, complete surgical excision of the tumor can be performed, with care taken to preserve adjacent neural and soft-tissue structures. 17 In this case, the lesion was successfully excised, and the patient had an uneventful postoperative course apart from localized numbness. Postoperative sensory deficits are a common complication of schwannoma excision due to the inevitable manipulation of the originating nerve. 18 However, motor function and ambulation were preserved in our patient.
Conclusion
Dorsal foot schwannomas are rare. Although imaging studies are important for evaluating soft-tissue masses, histopathological examination remains essential for definitive diagnosis. Though rare in the foot, schwannomas should be considered as a differential diagnosis of long-standing, painful soft-tissue masses. Complete surgical excision is curative in most cases, with favorable functional outcomes. This case further emphasizes the importance of combining clinical, radiological, and histopathological data for accurate diagnosis and optimal patient management.
Footnotes
Ethical considerations
The study adhered to the Declaration of Helsinki and was approved by the local Institutional Review Board (IRB)—approval ID MRC-04-25-637.
Consent to participate
Written informed consent was obtained from the patients for their anonymized information to be published in this article. A copy of the written consent is available for review by the editor of this journal upon request.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing is not applicable to this article as no datasets were generated or analysed during the current study.