
Abstract
Schwannoma, also known as neurilemmoma, is a benign neoplasm of Schwann cells of the cranial or peripheral nerve sheath. Scalp involvement has been reported in 25% of patients with extracranial head and neck schwannomas, which can be misdiagnosed clinically as epidermal cyst or lipoma. In this article, we report a 32-year-old male presenting with a slow-growing painful subcutaneous mass on the left occipital scalps without any neurological symptoms. Pathological findings confirmed the diagnosis of schwannoma, and surgical removal resulted in the resolution of pain and lack of recurrence.
Introduction
Schwannoma, also known as neurilemmoma, is a benign neoplasm of Schwann cells of the cranial or peripheral nerve sheath. Extracranial head and neck schwannomas are uncommon tumors, and it is commonly misdiagnosed as epidermal cyst, vascular malformation, or lipoma by clinicians due to their nonspecific clinical appearance.1,2 It frequently manifests as an asymptomatic or symptomatic solitary pink nodule, and the scalp involvement has been reported in 25% of patients with extracranial head and neck schwannomas. 1
Case report
A 32-year-old male presented with a slow-growing mass on the scalp. The lesion was present for 5 years and became painful during times of stress. He denied any past medical history and family history of similar lesions. Physical examination revealed a mobile subcutaneous mass of 4.1 cm × 3.5 cm size on the left occipital scalp. Initial differential diagnosis included lipoma and epidermal cyst. Patient opted for elective elliptical surgical excision due to the growth and pain symptoms (Figure 1). Excision of the overlying dermis, epidermis, and adipose tissue revealed a 2.5 × 2.5 × 1.5 cm firm neoplasm, which was carefully extracted from the galeal plane (Figure 2). Linear closure utilizing subcutaneous and epidermal sutures was used to decrease the dead space due to exposure of the galeal plane. Histologic examinations revealed an encapsulated, well-circumscribed mass with a proliferation of spindle-shaped cells with delicate, elongated, cytoplasmic processes, and alternating hypercellular (Antoni A) and hypocellular (Antoni B) regions (Figure 3).

Physical examination revealing 4.1 cm × 3.5 cm freely mobile subcutaneous mass on left occipital scalp.

Excision of the overlying dermis, epidermis, and adipose tissue revealed a 2.5 × 2.5 × 1.5 cm firm neoplasm.
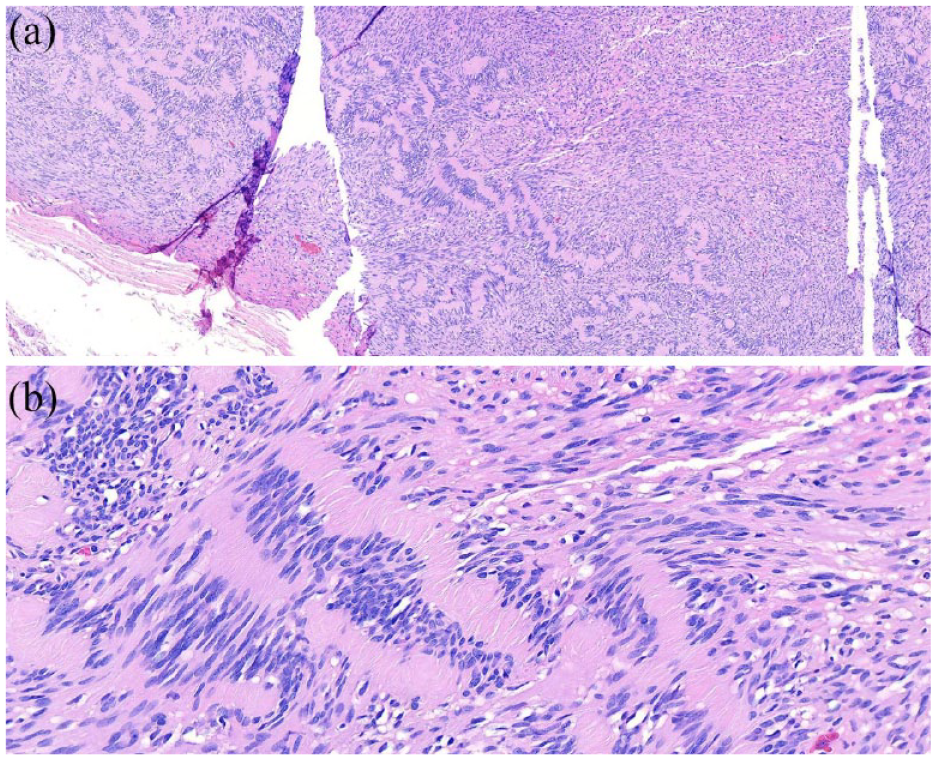
Histologic examinations revealing an encapsulated, well-circumscribed mass with a proliferation of spindle-shaped cells having delicate, elongate, and cytoplasmic processes with alternation of hypercellular (Antoni A) and hypocellular (Antoni B) areas with 10× magnification (a) and 40× magnification (b) in hematoxylin and eosin stain.
The histopathological findings led to the diagnosis of schwannoma. Following the procedure, the patient was pain-free with no recurrence in the 2 week and 8 week follow-up visits. Patient was advised to perform genetic testing in case of future similar lesions.
Discussion
A schwannoma is a benign slow-growing tumor of the nerve sheath consisting of Schwann cells. Classically, they present as a 0.5–3 cm diameter solitary, well-encapsulated skin-colored to pink nodule along the nervous system. 3 Family history and demographic of patients can lead to hereditary schwannoma diagnosis since patients under the age of 25 have been reported to have mutations in predisposition genes such as NF2, LZTR1, and SMARCB1. 4 Extracranial head and neck schwannomas are uncommon, and they are commonly asymptomatic; however, the mass effect can lead to symptoms such as discomfort, nerve palsy, and obstruction depending on the location of the lesion.1,2,5 A study conducted by Kang et al. 6 found unilateral neck masses as the most common location in 76% of 22 cases of extracranial nonvestibular head and neck schwannoma. Preoperative studies including fine-needle aspiration cytology (FNAC), computed tomography (CT), or magnetic resonance imaging (MRI) can be considered for diagnosis and evaluation of the mass. It has been reported that FNAC has 71.4% sensitivity for diagnosis of schwannoma for histopathological analysis. 1
Accurate diagnosis of extracranial head and neck schwannoma is recommended prior to the operation to avoid detrimental consequences including nerve palsy. 5 The gold standard diagnosis for schwannoma is based on pathological findings.3,7 The histological findings of encapsulated well-circumscribed lesions reveal overgrowth of Schwann cells with common alternation of axons-free areas of hypercellularity containing Verocay bodies and hypocellular areas, Antoni A and Antoni B respectively.3,7 Further immunohistochemical examination of positive Schwann cells via S100, the positive perineurial capsule via epithelial membrane antigen, and lack of axons presence via neurofilaments confirm the diagnosis of schwannoma.3,8
The management and treatment of this benign neoplasm depend on the severity of the symptoms. The surgical removal of schwannoma is the common standard of care; however, postoperative neurological deficit can present depending on the location of the tumor. 5 As a consequence of the uncommon location of schwannoma on the scalp in our case, the complete excisional surgical removal of the tumor resulted in symptomatic resolution and lack of recurrence.
Conclusion
Clinician needs to consider extracranial head and neck schwannoma as a differential diagnosis for the slow-growing mass of the scalp. Genetic testing should be considered for young patients. Preoperative imaging and testing, including FNAC, CT, or MRI, should be considered for the management of patients with schwannoma. Histopathological studies confirm the diagnosis of schwannoma, and the surgical excision leads to the resolution of symptoms and recurrence.
Footnotes
Acknowledgements
There is no acknowledgment for this article.
Author contributions
All authors had active roles in the preparation of original manuscript and the treatment of patient.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.