
Abstract
Curative surgery for a localized tumour at the early and pre-symptomatic stage is the main aim of lung nodule assessment. As part of the process, pre-operative tissue diagnosis is a key step in making appropriate clinical decisions and avoiding unnecessary invasive surgical intervention which is associated with high morbidity. In this case report, we describe a patient who had a curative lobectomy for a growing nodule without a preoperative tissue diagnosis although the initial discussion deemed it mandatory, and we dissected the arguments supporting it in the setting of a tuberculosis endemic country.
Keywords
Highlights
• This case report highlighted a patient with a suspicious lung nodule in a tuberculosis endemic country • A preoperative tissue diagnosis is the usual course of action to minimize the operative risk and avoid unnecessary surgery; however, in our case, there were two external factors that pushed us away from this practice • The technically challenging location of the tumour and hence, the unacceptable ensuing delay to arrange a tissue diagnosis and a growing nodule with time • We discussed this conundrum and highlighted the dilemma that many will face in our part of the world in managing pulmonary nodules.
Introduction
Curative surgery for a localized tumour at the early and pre-symptomatic stage is the main aim of lung nodule assessment. As part of the process, pre-operative tissue diagnosis is a key step in making appropriate clinical decisions and avoiding unnecessary invasive surgical intervention which is associated with high morbidity. This is also an important step in the assessment of a nodule in a tuberculosis endemic region such as Malaysia where tuberculosis is a differential diagnosis of any lung nodule. In practice, however, this priority may change. In certain circumstances, despite the obvious clinical necessity, the nodule location may render it technically non-accessible for pre-operative tissue diagnosis despite the availability of multi-modality approaches. If preoperative diagnosis is a must, this will cause unwanted delay in the management especially in early-stage tumour, whereby timely curative surgery is the most critical intervention. In this case report, we describe a patient who had a curative lobectomy for a growing nodule without a preoperative tissue diagnosis although the initial discussion deemed it mandatory, and we dissected the arguments supporting it in the setting of a tuberculosis endemic country. The nodule turned out to be a localized atypical carcinoid tumour. This conundrum could well apply to other chest centres in this part of the world.
Case study
Madam S, a 72-year-old Malay lady, non-smoker with past medical history of hypertension and a single cardiac stent had cardiac computed tomography (CT) as part of her chest pain assessment. She denied any specific respiratory symptoms or constitutional symptoms. There was no family history of malignancy, and she denied any occupational exposure to chemical fumes or radiation. Physical examinations were unremarkable.
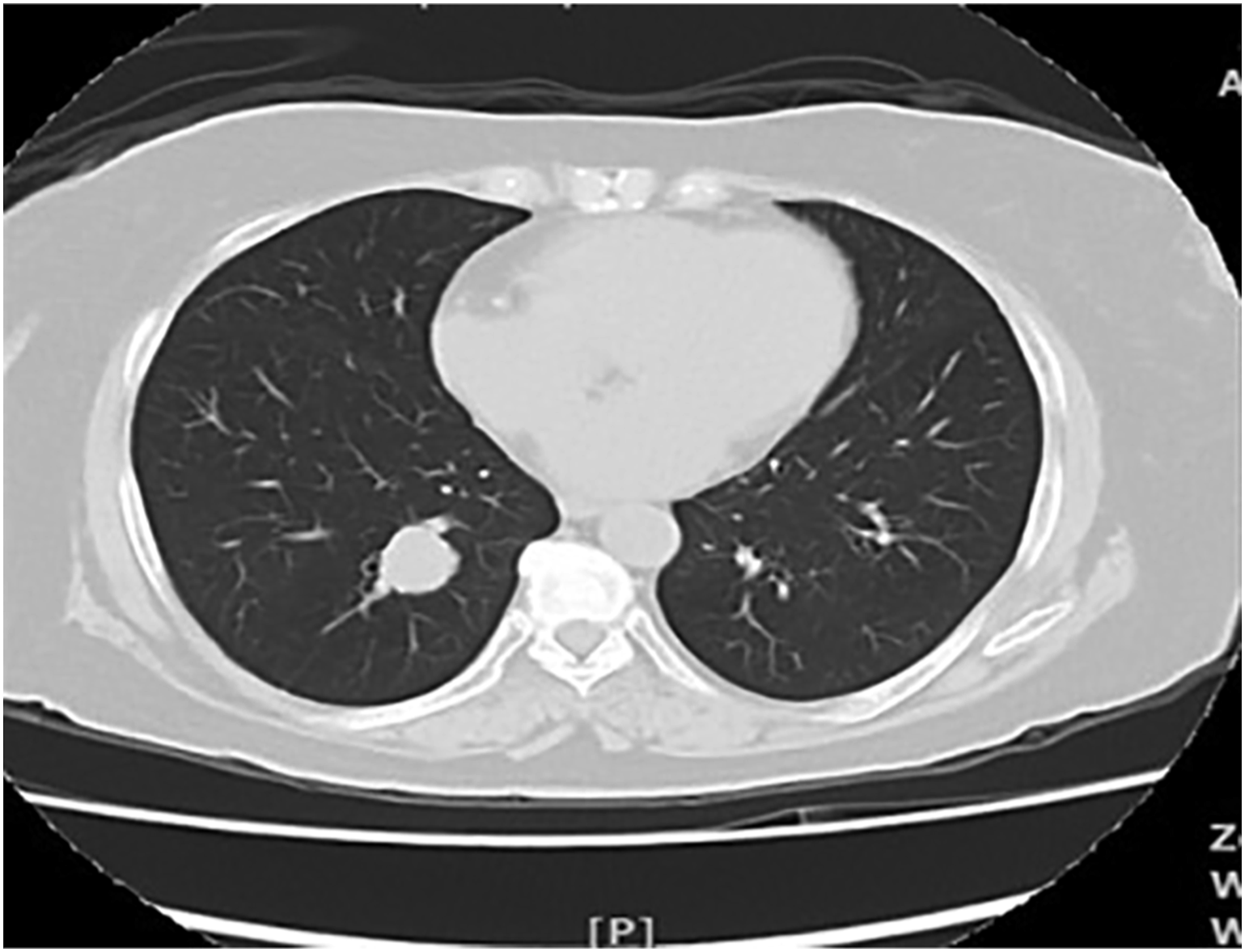
The cardiac CT noted an incidental finding of a solitary lung nodule in the right lower lobe measuring 17 mm × 17 mm which later confirmed in CT thorax (Figure 1). Brock’s score for the solitary lung nodule calculated a 28% risk of malignancy; hence, her case was discussed in a multi-disciplinary team discussion. A consensus was reached that a tissue diagnosis would be insightful with malignancy and pulmonary tuberculosis are likely possibilities, but its location precluded an approach via a bronchoscopy or a CT-guided biopsy. There were no connecting airways to the nodule and its location was central and adjacent to blood vessels. The next best option was a serial three-monthly CT monitoring which showed an enlarging lung mass, to 20 m × 18 mm × 20 mm in 9 months’ time (Figure 2). Positron emission tomography (PET) scan showed an increased fluorodeoxyglucose (FDG)-avid uptake in the solitary right lung nodule which was suspected of malignancy and tuberculosis with no other distant uptake (Figure 3). The latter is less likely. CT thorax in axial view lung window showed a solitary lung nodule in the right lower lobe measuring 17 mm × 17 mm. CT thorax in axial view lung window during follow-up at 9 months showed an enlarging lung nodule to 20 mm × 18 mm × 20 mm. . PET scan showed an increased FDG-avid uptake in the solitary right lung nodule with no other distant uptake in axial (left) and coronal view (right). PET: positron emission tomography; FDG: fluorodeoxyglucose.

Pre-operative cardiac and respiratory assessments showed good functional reserve and low risk for surgery. Echocardiogram showed left ventricular ejection fraction was 66% and no regional wall abnormality. Pre-operative FEV1 and diffusing capacity lungs for carbon monoxide were both > 80% predicted. The patient then proceeded to have Right VATS lower lobe lobectomy and lymph node sampling. Macroscopically, a well-circumscribed tumour measuring 22 mm × 20 mm × 13 mm was resected and clear margins were achieved. Histology of the tumour showed atypical carcinoid tumour with positive immunohistochemistry for synaptophysin, chromogranin A and CD56. The Ki-67 proliferation index was low (5%). All 10/10 lymph node samples were negative. Her pathological staging was pT1cN0 based on the 2010 American joint committee on cancer TNM classification of malignant tumours Staging of NETs of the Lung. Post-operatively, she has no complication and discharged after day 5 of surgery.
Discussion
Lung nodules are the commonest extra-cardiac finding in cardiac CT studies, 1 as the case in our patient. The differential diagnosis of lung nodules encompass both benign and malignant causes, which can be stratified using lung nodule risk calculators utilizing clinical and radiological characteristics. This will expedite the diagnosis and treatment of patients with malignant nodules and to minimize testing in patients with benign nodules. The Brock model was validated for both the lung cancer screening programme 2 and individuals with incidental nodules. 3 Our patient’s risk was high based on Brock’s Model which warranted further intervention with tissue sampling. 4 In addition, the endemicity of TB in our part of the world mandates pulmonary tuberculosis to remain a possibility in the assessment of pulmonary nodules and a preoperative diagnosis would avoid a risky surgical intervention.5,6 Unfortunately, its location precluded the attempt at diagnosis by either a bronchoscopy or via a CT-guided approach.
A short-term interval imaging by a serial three-monthly CT scanning, which we took instead, was a reasonable alternative follow-up as recommended by the Fleischner Society Guidelines. 7 We also believe that any new typical radiological changes of tuberculosis with time will help us consider the diagnosis of pulmonary tuberculosis. The volume-doubling time of the lung nodule in the subsequent CT scans strengthened our initial suspicion of malignancy with a PET F-FDG scan showing a localized tumour without distant metastasis; tuberculosis was becoming less likely. Pursuing a pre-operative tissue diagnosis at this point at our institution would likely lead to a longer wait for the definitive treatment which could offer a curative intention and worse delay if it had required multiple biopsy attempts. These supported the arguments for the urgent need of surgical resection without pre-operative tissue diagnosis.
Surgical resection without pre-operative tissue diagnosis is safe especially in good functional status and low surgical risk patients. In a study of 443 patients operated on without a perioperative diagnosis, there was no mortality or major complications, and the perioperative minor morbidity rate was about 9.7%. 8 Furthermore, post-operation benign disease was only found in about 7.8% patients without preoperative diagnosis. A significantly lower proportion of patients without perioperative diagnosis waited a shorter interval for surgery and there were more likely stage I disease. These are beneficial when the chance of disease detection at an early stage should theoretically increase, leading to a greater chance of surgical cure and better survival.
Post-operatively, histology studies showed the tumour was early-stage neuroendocrine with good nodal clearance. It isworth noting that pre-operative PET scan for this patient utilized F-FDG as a tracer that maybe less sensitive compared to the Ga-DOTATATE tracer in detecting low-grade neuroendocrine tumour and Ki-67 proliferation index. 9 This highlights the disadvantage of pre-operative PET scan staging without tissue diagnosis. Pathological staging post-operative re-assured the tumour was at early stage. Other histological features include low-grade and Ki-67 proliferation index also indicated less aggressiveness of the present tumour. 10
Surgical resection is the treatment of choice and the only curative option for localized atypical carcinoid tumour with the aim to remove the tumour and preserve as much normal lung tissue. 11 Localized disease should be managed with curative intent. In addition, systematic nodal dissection should be carried out to designate R0 resections during the curative surgery. 12 Post-operatively, general follow-up recommendations include a reassessment once between 3 and 6 months after complete curative resection and then every 6–12 months for at least 7 years thereafter. 13 This is in view of risk of late relapse (up to 19% of relapses were 7 years from resection in some series) reported in the literature.14–16 The follow-up assessments should include serial serum chromogranin A.
Conclusion
Even in a tuberculosis endemic area, curative surgery for a localized lung nodule without a preoperative tissue diagnosis is safe and should be the option in difficult-to-biopsy lesions with high suspicion of malignancy when a proper assessment and investigation have been conducted. This avoids the unnecessary delay in the diagnosis in many busy chest centres and allows an early definitive treatment.
Footnotes
Acknowledgements
Not required.
Authors’ contributions
All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Availability of data and materials
Not required.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
(include full name of committee approving the research and if available mention reference number of that approval): AIMIE R. M AMIN IBRAHIM, M FAUZI RANI, A AZAM MOHAMMAD RAZI.
Informed Consent
Informed Consent was taken from the patient for the publication of case report.
Trial Registration
Not applicable.