
Abstract
Background
Synovial osteochondromatosis is a rare, benign condition characterized by the formation of cartilaginous nodules within the synovium. It commonly occurs in the anterior compartment of the knee joint and predominantly in middle-aged men. It is relatively unusual in females, and at this remarkable age, there is a greater probability of missed diagnosis.
Research Design
This case report describes a 63-year-old female with classical synovial osteochondromatosis complicated by a clinically suspected septic arthritis of the right knee. Underlying comorbidities, including hypertension, diabetes mellitus, and hyperlipidemia further complicate patient management.
Conclusions
We have detailed anesthetic and clinical management strategies to stabilize the patient preoperatively and ensure successful surgical outcomes.
Introduction
Synovial osteochondromatosis (SO) is an unusual proliferative and metaplastic disorder that often presents with chronic joint pain and dysfunction owing to the presence of multiple intra-articular cartilaginous nodules in the synovial membrane of the joint, tendon sheath, and bursa, 1 which can cause mechanical symptoms and lead to degenerative joint changes over time. The prevalence of SO is not well documented due to its rarity, but men are reported to be affected with SO up to four times more commonly than women. 2 Although SO can develop in any joint where the synovium exists, it is most prevalent in the knee, followed by the hip joint,2,3 which typically affects diarthrodial, weight-bearing joints of individuals 30-60. Within the knee, the disease predominantly occurs in the anterior compartment, such as the suprapatellar pouch, medial or lateral gutter, and infrapatellar fat pad. 4
SO can mimic septic arthritis (SA), which can cause joint pain, swelling, redness, and warmth. 5 However, this condition becomes particularly challenging when accompanied by SA, necessitating urgent surgical intervention. SA is an orthopedic emergency that can lead to rapid joint destruction and systemic sepsis if not treated promptly. The coexistence of SO and SA is rare, but significantly complicates the clinical picture. This case report highlights the complexities involved in perioperative care of these patients and provides insights into effective management strategies. Here, we discuss anesthetic considerations, surgical approaches, and postoperative care, emphasizing the importance of a multidisciplinary approach in managing patients with multiple comorbidities.
Case report
A 63-year-old woman presented to the emergency department on June 6, 2024, following a near-syncope episode secondary to hypoglycemia with a random plasma glucose level of 3.0 mmol/L. She reported worsening right knee pain over the previous week, of which sought outpatient medications from a general practitioner (GP), compounded by a year-long history of right knee pain that rendered her wheelchair bound without any specific injury. Additional symptoms include loss of appetite, poor oral intake, lethargy, intermittent fever, and constipation. Her medical history included hypertension, diabetes mellitus, and hyperlipidemia.
Upon presentation, the patient’s vital signs were as follows: blood pressure, 114/59 mmHg; heart rate, 112 beats/min; respiratory rate, 20 breaths/min; temperature, 39.1°C; and SpO2, 97% on room air. She was septic-looking and distressed, without obvious signs of dehydration. Physical examination revealed moderate tenderness over the medial and lateral joint lines ( pain score of 9/10), visible knee effusion, reddish discoloration of the knee joint, and palpable mass across the joint line. Gait assessment could not be performed because of worsening right knee pain.
Initial laboratory investigations revealed hyponatremia with a sodium level of 131 mmol/L, acute kidney injury (AKI) evidenced by a urea level of 38.2 mmol/L, and creatinine level of 368 µmol/L resulting estimated glomerular filtration rate (eGFR) 11 mL/min/1.73 m2. Septic workup revealed evidence of infection with leukocytosis with a white blood cell count of 18.3 × 109/L, predominant neutrophils (76%), and C-reactive protein (CRP) level of 257.9 mg/L. Her arterial blood gases (ABG) showed type 1 respiratory failure. The other laboratory results were within normal limits.
Right knee anteroposterior and lateral radiographs (Figure 1) revealed numerous calcified loose bodies within the joint space, indicative of SO. Other intra-articular structures, including the cartilage, meniscus, and ligaments, could not be visualized owing to X-ray limitations. Right knee MRI was not ordered because of urgent assessment of a clinically suspected right knee SA. Given the above presentations, the patient was referred for right knee arthrotomy washout for SA under spinal anesthesia to resolve the symptoms and make a definite diagnosis of SO complicated by SA. Preoperative X-ray of the right knee, displaying lateral and anteroposterior views with numerous calcified loose bodies within the joint space, indicative of synovial osteochondromatosis (SO).
In the emergency department, the patient was initially managed with nebulization of salbutamol to relieve her bronchospasm. An intravenous (IV) dextrose D50% 50cc stat, IV pantoprazole 40 mg, IV maxolon 10 mg, IV hydrocortisone 200 mg, and IV augmentin 1.2 g were administered as well. In the ward, she received IV Unasyn 3 g OD, IV pantoprazole 40 mg OD, oral vitamin C 1 g OD, oral ultracet, and continuous IV dextrose (D5%) infusion. Blood tests for serial CRP levels, full blood count, renal function tests, and other relevant profiles were performed to monitor the patient’s condition.
The patient was then resuscitated with intravenous normal saline for 2 days to address acute kidney injury (AKI), improve renal function, and stabilize her overall condition before surgery. Once stabilized, the patient underwent right knee arthrotomy and washout under spinal anesthesia. Intraoperatively, multiple crystallized cartilaginous nodules (Figure 2) were removed from the right knee joint during arthrotomy for SA, consistent with SO, along with synovial pus, further confirming the clinical diagnosis of SA. The operation lasted for approximately 1 hour, with minimal blood loss. The patient was intraoperatively hemodynamically stable. Her sugar levels normalized both intraoperatively and postoperatively. Intraoperative image showing multiple cartilaginous nodules removed from the right knee joint during arthrotomy for septic arthritis (SA), consistent with synovial osteochondromatosis (SO).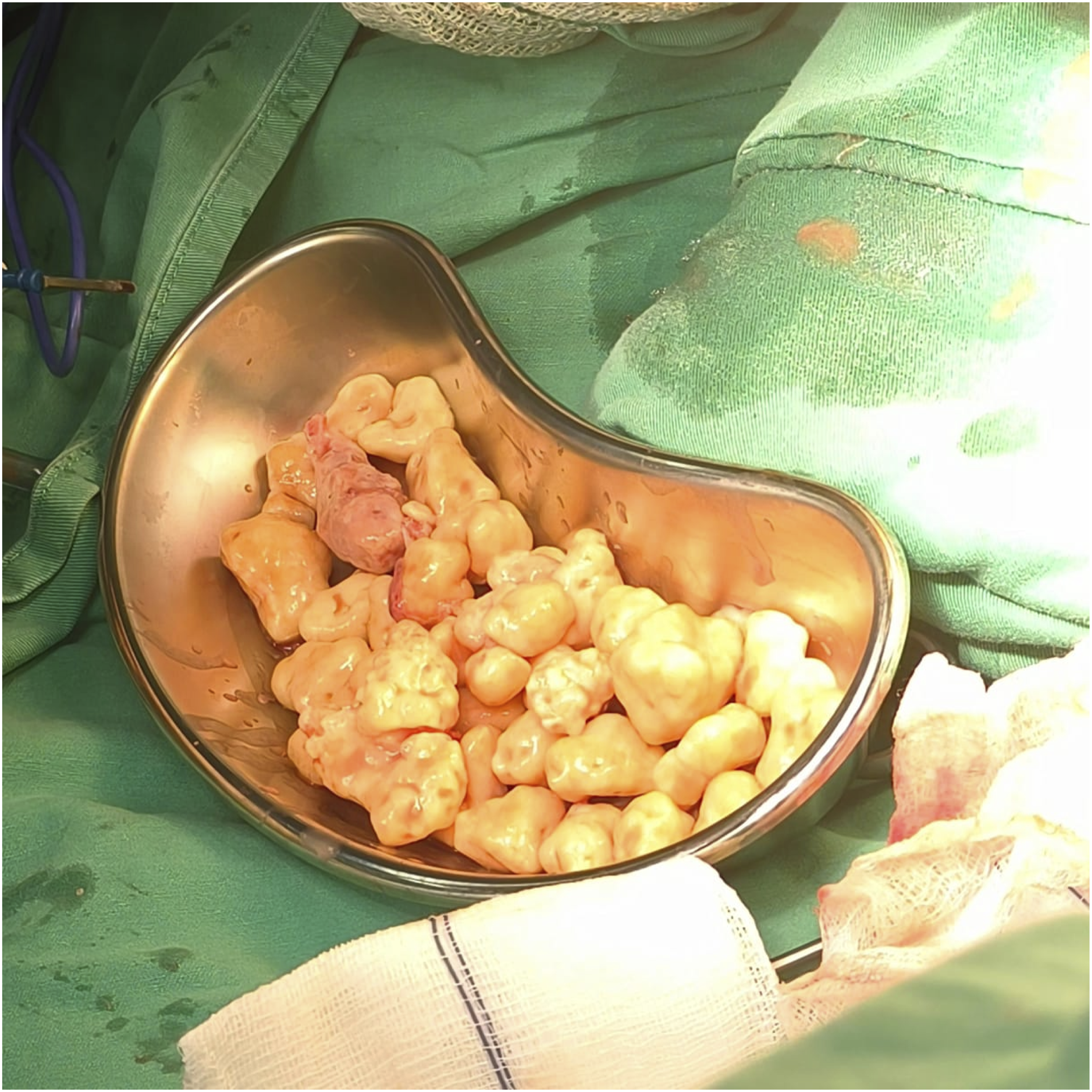
Postoperatively, the patient’s symptoms improved dramatically. However, negative culture and sensitivity for synovial fluids, pus, and crystals ruled out the definitive diagnosis of SA. The patient was subsequently hospitalized to complete the course of the antibiotic therapy. Serial MRI follow-up was recommended to detect recurrence since the lesions were not detected preoperatively using detailed radiographs. However, in our case, the patient’s family refused it because of the economic burden. Nevertheless, the patient showed no recurrent disease 2 months after surgery.
Discussion
Synovial osteochondromatosis (SO) is a rare benign condition characterized by the formation of multiple cartilaginous nodules within the synovium, often leading to chronic joint pain and dysfunction. 1 The etiology of SO remains unclear, but it is thought to arise from the metaplasia of synovial cells into cartilage-forming cells. 2 This condition commonly affects the knee joint, consistent with the current case.
Primary or idiopathic SO involves normal joints unrelated to trauma, infection, synovial irritation, or genetics. 6 It presents at an earlier age, 30–40 years, and is relatively rare.1,2 This is compared to secondary SO, where there is an underlying joint pathology resulting in synovitis and articular destruction, such as trauma (single traumatic event or repetitive microtrauma), osteochondritis dissecans, advanced osteonecrosis, or Charcot neuropathic joint. 6 Patients with secondary SO were relatively older, in their 50s and 60s. 6 SO can be classified into three stages: initial active intrasynovial disease without loose bodies, transitional lesions with active intrasynovial proliferation and loose bodies; and multiple loose bodies with subsiding synovitis. 7
Septic arthritis (SA) complicates SO management, necessitating urgent surgical intervention to prevent joint destruction and systemic sepsis. 5 The presence of comorbid conditions such as diabetes mellitus and hypertension increases the risk of infection and complicates perioperative management. In particular, diabetes mellitus is associated with impaired immune response and poor wound healing, which can exacerbate the severity of infections.
SO is a self-limiting condition.6,7 Therefore, conservative management may be effective for some patients. Non-steroidal anti-inflammatory drugs (NSAIDs), modification of their activities, and cryotherapy should be considered.1,6 However, the reduced range of motion and mechanical symptoms of locking and catching from loose bodies can have deleterious consequences for joint destruction. Hence, the definitive management of SO is the surgical removal of loose bodies with or without synovectomy.3,8 Synovectomy for synovium-based pathology sounds is the primary indication for management. 8 However, there is no strong evidence in favor of this option, along with the surgical removal of loose bodies. In the past, multiple studies have supported the option of performing isolated removal of loose bodies without additional synovectomy, as there is no superiority for such an addition.3,8 In other studies, synovectomy has been supported to prevent recurrence.3,4,8
Additionally, whether to perform synovectomy arthroscopically or through an open approach is controversial. 9 Open synovectomy offers better visualization of joint surfaces. 8 Arthroscopic management is associated with lower morbidity, quicker return to function, shorter hospital stay, reduced postoperative pain, and faster rehabilitation.3,9 In this case, the patient presented with both SO and clinically suspected SA, making management exceptionally challenging. The choice of spinal anesthesia is crucial to avoid potential complications associated with general anesthesia such as hemodynamic instability and airway management issues. Although studies have shown that arthroscopic exploration and removal of loose bodies combined with partial synovectomy is an effective treatment for SO, in this case, the patient was managed with arthrotomy and washout under spinal anesthesia because of clinically suspected worsening right-knee SA. Although intraoperative findings of multiple crystallized structures and pus were suggested, with negative culture and sensitivity for synovial fluids, pus, and crystals, the diagnosis of SA was excluded.
Continuous hemodynamic monitoring and collaboration among surgical, anesthetic, and medical teams are pivotal for successful outcomes. The patient’s comorbid conditions, including diabetes and hypertension, necessitated meticulous preoperative optimization and intraoperative management.
Conclusions
This case highlights the importance of comprehensive perioperative care in patients with complex medical histories undergoing emergency orthopedic surgery. Prompt recognition and treatment of septic arthritis in the context of synovial osteochondromatosis are vital to prevent severe complications. Multidisciplinary collaboration and tailored anesthetic strategies are essential for ensuring optimal patient outcomes.
Footnotes
Author contributions
All authors managed the patient, and prepared the manuscript, edited, and approved the final draft.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institute does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient for her anonymised information to be published in this article.
Data Availability Statement
Data sharing is not applicable to this article as no datasets were generated or analysed during the current study.