
Abstract
Introduction
Postnatal depression (PND) has been estimated to affect between 10 and 25% of women worldwide. 1 PND is a major public health problem which has been associated with maternal and familial distress, 1 suicide risk, as well as impaired child development and behavioural outcomes. 2
To facilitate early detection and treatment of PND, a programme for postnatal emotional health screening was introduced at a large public maternity hospital in 2008. Under this programme, women are prospectively recruited up to 6 months post-natally and are screened for PND using the Edinburgh Postnatal Depression Scale (EPDS). High-scorers (EPDS scores ≥13) are offered psychiatric review and intervention, while those with borderline scores (EPDS scores 10-12) are offered counselling and phone follow-up by clinical counsellors.
Although PND is highly treatable, many women with the condition are unable or unwilling to seek professional help.3,4 Studies have shown that at most, 50% of women who are distressed post-natally seek treatment.5–8
There is a need to understand the reasons behind women’s unwillingness to seek professional help for PND, so as to improve maternal, familial and child outcomes. While other studies have explored help-seeking behaviours in women with PND, to our knowledge, this is the first Singaporean study to examine this issue.
Methods
From April 2008 to January 2010, 214 women who returned to a public maternity hospital for their postnatal obstetric check-ups were screened to be at risk of postnatal depression, with scores of 13 and above on the Edinburgh Postnatal Depression Scale (EPDS). They were contacted by the study team for recruitment into this study via phone contact. Women were eligible for this study if they were 21 years of age or older, up to 6 months postpartum, had an EPDS score of 13 and above, and were English-speaking. Ethics approval was obtained from the Singapore Health Services Institutional Review Board, which approved the waiver of written informed consent. Verbal informed consent was obtained from all participants.
Of the 214 women who screened positive, 68 women could not be contacted, 71 women declined to participate in the study and 27 non-English-speaking women were excluded. 48 women were recruited and participated in the phone interview, which was conducted by a study team member (JW) between December 2009 and April 2010. During the interview, the participants were first asked to complete a socio-demographic questionnaire. They were then asked two open-ended questions: “In your experience, after you were informed of the possibility that you might have post-natal depression, what were some of the factors that might have stopped you from accepting a referral to see a psychiatrist” and “What were the factors that might have helped you to accept a referral to see a psychiatrist?” The interviews were audio-recorded, transcribed and imported into NVivo8 for analysis by JW and ES. Thematic analysis was used to identify themes. Two researchers (JW and ES) coded the data independently and discrepencies were discussed until a consensus was reached. No further participants were recruited after the 48th interview as data saturation had been reached; no new codes, themes or data were identified during analysis of the final interview.
Results
Demographic and clinical data of the participants a (n = 48).

aData are presented as number (percentage) of subjects unless otherwise stated.
Themes and subthemes.
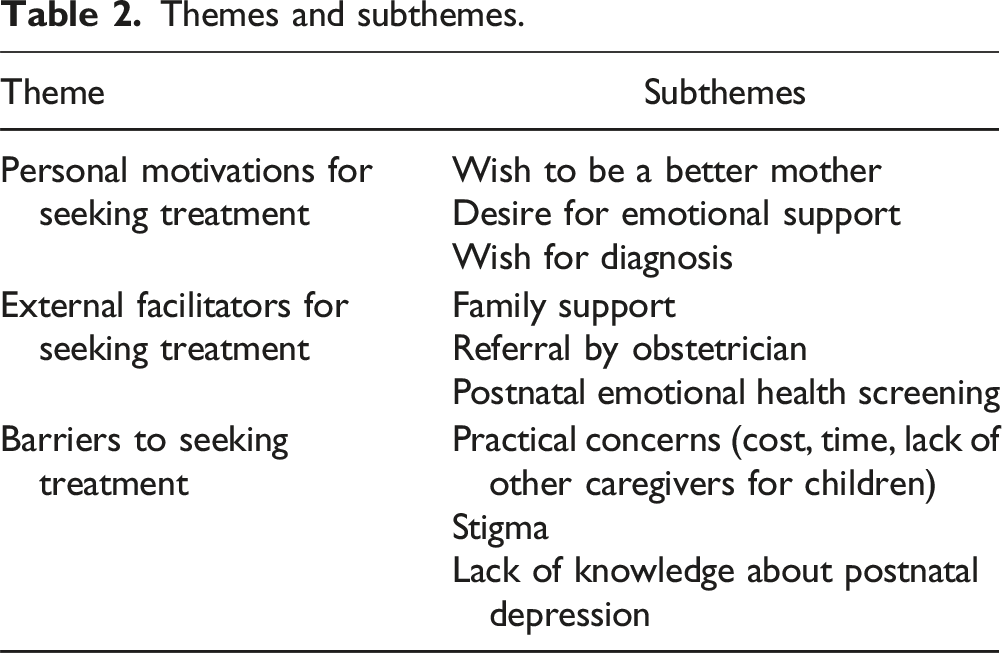
Theme 1: Personal motivations for seeking treatment
Several participants felt that their depressive symptoms affected their ability to care for their children, and wanted to recover for the sake of their children. For example, one participant shared, “I knew that I was having problems controlling my emotions and I could feel that I was affected by everything. I need to get well. I have four children and I need to be there for them. I have to keep my emotions healthy, to take care of my children. At the end of the day, this is to protect the family. I don’t want to take it out on the kids.” (P4)
Participants also expressed a wish to seek mental health treatment so that they would have a source of emotional support, which they felt was otherwise lacking in their lives. As one patient reported, “I had many family problems after giving birth…I was very down, not happy at all. I believe that if I go and see the doctor, I can speak about what is in my heart. I need someone to advise me, someone who can listen to me.” (P26)
In addition, participants spoke about seeking a mental health assessment as they suspected that they might be suffering from postnatal depression, and wished for confirmation by a mental health professional. One patient said, “Actually I already suspected that I had depression. I would lose my temper with my son and I was behaving unreasonably. I just want to confirm what’s the problem and learn how to overcome it.” (P14)
Theme 2: External facilitators for seeking treatment
Participants who were keen to seek treatment were encouraged by their family members, particularly by their husbands, to seek help. Some had family members who offered help with child-minding, which allowed them to have the time to see a psychiatrist. “My husband is supportive and encouraged me to seek help before the problem got worse. He said that if there’s something wrong with me, I should see a doctor to get it cured. If my husband had not taken leave and accompanied me, I would not have gone for the appointment. He brought the kids together with me to the clinic.” (P18)
Participants also shared that their obstetricians/gynaecologists played an important role in encouraging them to seek mental health treatment and facilitating referrals to a psychiatrist. As patients had an established relationship with their obstetricians/gynaecologists, they felt comfortable disclosing their emotional difficulties to them. Participants also thought that their obstetricians would be familiar with postnatal depression and would refer them to a psychiatrist if needed. As one participant shared, “I spoke to my obstetrician and told her about my situation, because I feel that I can talk to her. I’m sure that coming from O&G, she should be aware of postnatal depression. If not for her referral, I wouldn’t know what to do or whom to call.” (P48)
Participants found routine postnatal emotional health screening helpful. They appreciated that the counsellor encouraged them to seek help, and provided support in the form of follow-up phone calls after the screening. “A month after I delivered my baby, I got an appointment to see the gynaecologist. But before that, the hospital arranged for me to see the counsellor. The counsellor knew that I might have postnatal depression and she arranged for me to see the psychiatrist. The counsellor also called me and asked me how I was doing. I felt good after talking to her… I appreciate that someone is doing this kind of communication.” (P4)
Theme 3: Barriers to seeking treatment
Many participants were hesitant to seek treatment due to practical concerns, such as lack of time, lack of alternative caregiving arrangements for their children, as well as concerns about the cost of psychiatric treatment. One patient shared, “I really just couldn’t find the time to leave the house. I was breastfeeding my baby and my husband is not confident enough to be left alone with the baby. I didn’t want to bring my baby along as he was born premature and I didn’t want to expose him to the outdoors” (P16)
Another patient reported, “I was worried about finances because I am a housewife and I depend on my husband financially. What happens if I see a psychiatrist? Medical charges are not cheap, especially for specialists. And after every birth there’s usually a lot of bills, a lot of financial issues.” (P27)
Participants were often concerned about the stigma associated with seeking psychiatric treatment. “Being Asian, we are not that open to this. People think that seeing a psychiatrist is taboo. When you see a psychiatrist people will think that you are mad.” (P28)
A participant shared her fears that she would be judged for being unable to cope, if people learnt that she had sought psychiatric treatment. “To see a doctor for depression is like saying that I have problems, I can’t manage. It becomes like a weakness. People would doubt my capability to handle the newborn.” (P36)
Several participants did not think that they needed to seek treatment as their understanding of postnatal depression was limited; they tended to view their depressive symptoms as a normal, transient period of adjustment to motherhood which was caused by lack of rest and hormonal changes. As a result, they often preferred to wait for their symptoms to improve instead of seeking treatment early. “I heard from everybody that it is normal to get postnatal depression and that after 2 or 3 months, it will be ok. I find that it’s just a phase and I just need to get over it. Maybe I don’t have enough sleep or rest, maybe it’s a hormonal thing. I just have to get used to it.” (P38)
Discussion
The barriers to seeking treatment cited by study participants were consistent with barriers described in existing literature. Practical concerns such as ‘childcare issues’ and ‘lack of time’ have commonly been cited as reasons for not accessing treatment. 9 In the Singaporean context, the common traditional practice of ‘confinement’ (staying home for postnatal recuperation for 30 to 40 days), may make it especially difficult for postnatal women to seek psychiatric treatment in the first postnatal month.
It is also known that stigma is one of top barriers to help-seeking amongst postnatal women. 9 Women who are concerned about stigma associated with psychiatric treatment have reported fears of being ‘labelled mentally ill’, 10 being judged as a ‘bad mother’, 11 or being alienated. 12 There might also be stigma attached to antidepressant treatment. 13 Stigmatization of mental illness continues to be prevalent in the Singaporean context. 14
Lack of knowledge about postnatal depression is also a well-known barrier to help-seeking.15,16 Participants of this study often normalised their depressive symptoms and opted to wait for their symptoms to improve spontaneously. Postnatal women with depressive symptoms find it difficult to distinguish between normal levels of distress from distress that warrants professional help. 17 PND symptoms are often perceived to be related to adjustments to mothering and women who perceive PND symptoms to be short-lasting tend to under-utilize treatment. 18
Known facilitators of help-seeking behaviour in postnatal women include social facilitators such as support from family or healthcare providers, instrumental facilitators such as support with childcare and transportation, and structural facilitators such as provider responsiveness and community-based support.15,19,20 Our study participants agreed that social facilitators were key; support from their families, obstetricians and the clinical counsellors that they met through postnatal emotional health screening encouraged them to seek psychiatric support. Family support took the form of encouragement to seek help, as well as practical support such as accompanying the women for consultations or offering help with child-minding. It is known that families who normalize women’s depressive symptoms hinder help-seeking, 15 whilst families who are encouraging and express concern encourage help-seeking. 21 With regard to support from healthcare providers, it is known that care providers who encourage disclosure of symptoms and acknowledged women’s depression in turn encourage help-seeking. 21 Several study participants reported that they accepted their obstetricians’ advice to seek psychiatric treatment due to the established relationship they shared with their obstetricians. Participants also valued the screening and professional advice offered during postnatal emotional health screening, and engaged in psychiatric treatment with the encouragement of the clinical counsellors who conducted the screening.
Participants’ reported personal motivations for seeking treatment provided an interesting perspective that has not been commonly reported in existing literature. Many participants sought help as they feared that their depressive symptoms, left untreated, would affect their ability to care for their children. Others hoped that mental health professionals would offer emotional support; it has been found that women’s dissatisfaction with the deficient family and spousal support might prompt them to tap onto external support from professionals. 22
One limitation of the study is that of recall bias, given that some participants were interviewed more than a year postpartum. The study team member who interviewed the participants (JW) was also part of the care team for some of the participants and this could also have introduced researcher bias and participant bias. To mitigate this, participants were reassured that their responses would not affect their clinical care. Lastly, the study results are not generalizable to the general postnatal population, or to women diagnosed with postnatal depression, as we studied a sample of women screened with the EPDS. Future studies can consider investigating the help-seeking behaviours of depressed women at several time points, both prior to and after treatment, so that we may be able to better understand facilitators or barriers related to service provision. It may also be helpful for future studies to explore if there may be differences in help-seeking behaviour amongst women of different ethnicities in Singapore.
Interventions to encourage help-seeking in women with symptoms of postnatal depression should address both barriers and facilitators of help-seeking. In addition, women’s personal motivations for seeking treatment should be explored in greater detail when healthcare providers attempt to engage them in psychiatric treatment. Postnatal emotional health screening is key; the American College of Obstetricians and Gynecologists recommends that all patients are screened at least once for depression and anxiety during the perinatal period, 23 while the Singapore Perinatal Mental Health Guidelines on Depression and Anxiety similarly recommends that patients are screened for antenatal and postnatal depression and anxiety. 24 The practical barriers cited by many postnatal women may be addressed by modalities of care provision which increase access to care, such as community-based support 25 or telehealth. 26 There is a need for increased education about PND to increase awareness of the condition amongst postnatal women, their families and healthcare providers, and to reduce stigma associated with psychiatric treatment of the condition. Healthcare providers may also consider employing motivational interviewing (MI) to strengthen patients’ personal motivations to seek treatment, by exploring patient’s motivations for change; MI has been shown in a pilot study to encourage help-seeking in mothers with depression, 27 and has shown promising results for improving treatment adherence among women with postnatal depression. 28
Footnotes
Acknowledgments
The authors would like to thank all the participants for their support and contributions towards the study.
Author contributions
JW conceived the study, recruited study participants and interviewed them. JS and ES conducted a literature survey and carried out data analysis. All authors reviewed and edited the manuscript, and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Data availability statement
The datasets generated and analysed during the study are available from the corresponding author.