
Abstract
Background and objectives
Vaginal digital examination and transvaginal ultrasound are routinely for clinical assessment. Many women find these procedures uncomfortable, embarrassing, and stressful. Negative experiences increase anxiety and discomfort experienced during subsequent examinations. Emotional distress and fear of pain result in women avoiding gynaecological screening and follow-up. This study uses qualitative methods to evaluate the experience of patients who have undergone both vaginal digital and transvaginal ultrasound examinations, collectively called pelvic examinations (PE) in the outpatient setting of a tertiary hospital in Singapore.
Methods
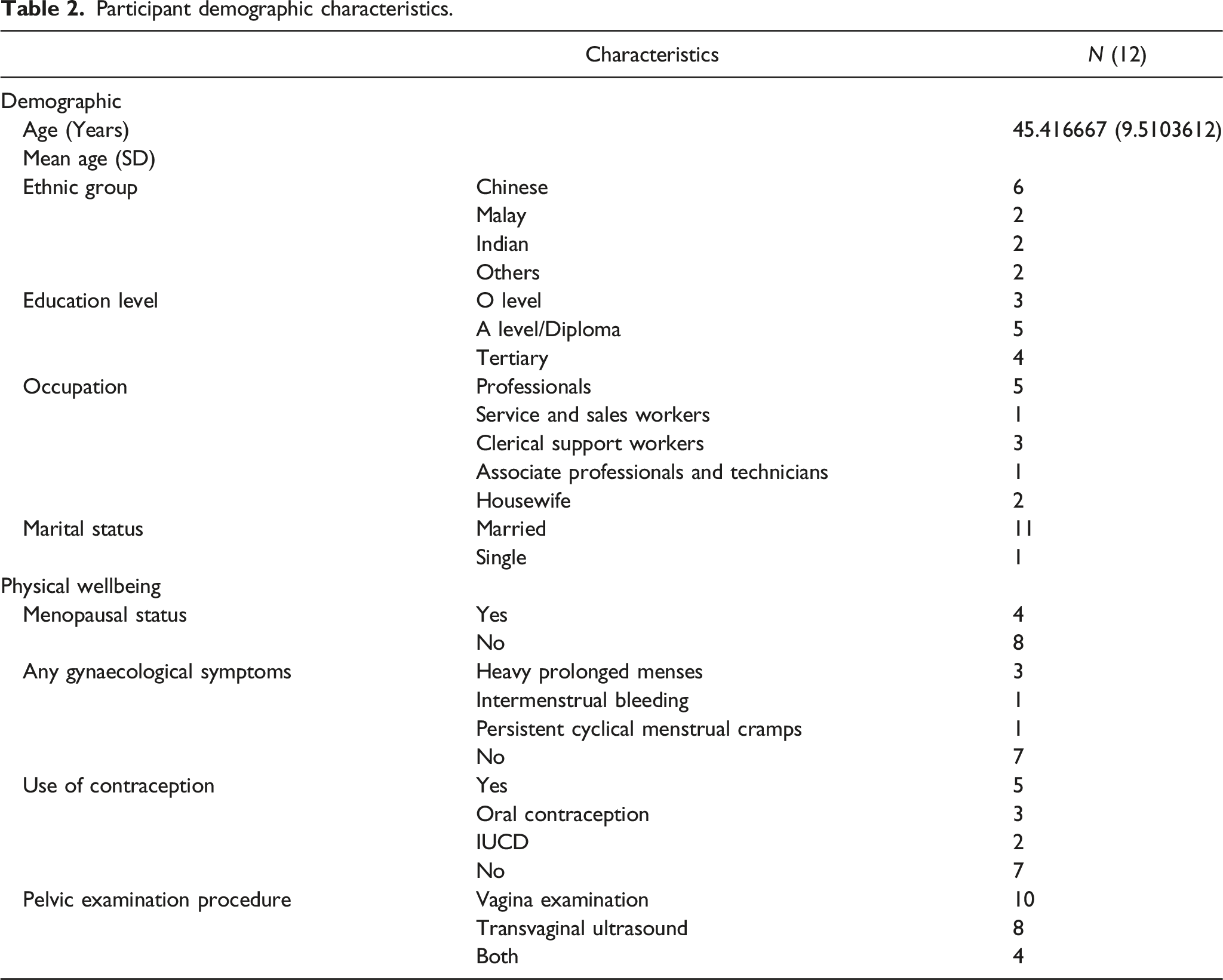
Qualitative semi-structured interviews were conducted on 12 participants aged 30-57 years. Interviews were audio-recorded, transcribed, audited, and analysed iteratively based on grounded theory. Emergent themes were first externally validated and finalized after rounds of deliberations amongst the investigators. This included descriptions and concepts reflecting the most important matters experienced by participants.
Results
Majority of participants found PE unpleasant and uncomfortable especially when providers were perceived to have poor communication and examination skills. Factors that improve their experience include a conducive environment that is, privacy, dim lights, and warm lubricant. Having adequate information before and during the procedure was important especially for first time.
Conclusion
Patient-centred care ensures a positive experience in relation to the themes found in this study. Gaps in HCP training on communication and procedure skills should be addressed. Efforts should be made improve the clinic environment and provide adequate information to patients.
Introduction
Pelvic examinations (PE) in the form of vaginal examination and transvaginal ultrasounds are routine evaluations in a women’s health assessment. They are important in the detection of cancer of the reproductive organs, infectious diseases and other benign conditions and should be performed only after a proper explanation and obtaining patient consent.
Conventionally the vaginal examination includes external visual inspection followed by a speculum examination to assess the internal genitalia. At this point, opportunistic cervical cancer screening may be performed using a cytology brush. Subsequently a bimanual examination is performed to evaluate the pelvic organs. Occasionally, a rectovaginal examination may be done if deemed necessary. If warranted, a trans-vaginal ultrasound involves inserting a transducer (probe) into the vagina for ultrasonic evaluation of structural abnormalities. More detailed images are seen during this method compared to the trans abdominal ultrasound.1,2 For the purposes of this study, PE includes both the vaginal examination and the transvaginal ultrasound.
Most studies on patient experiences of PE have been via quantitative methods using patient surveys. In addition to physical discomfort, studies show that PE may also have an emotional and psychological effect. Physical experiences described range from discomfort to pain. 2 Women feel vulnerable throughout the process due to exposure of intimate parts of the body. Patients describe a loss of control and embarrassment, worries about their own cleanliness and vaginal odour during the procedure. Some are fearful of discovery of a pathological condition, and many fear pain.3–5
Globally, studies have shown that patients do not understand the purpose of PE and cervical cancer screening. 6 A systematic review in Southeast Asia (SEA) uncovered the top three barriers to PE-embarrassment, time constraints and not understanding the importance of cervical cancer screening. 7 This suggests that patient education-based interventions will be useful to address these barriers. From a physicians’ perspective, the most common reasons that PE is difficult is perceived to be from a previous negative experience and patient anxiety or fear regarding the exam. 8
We know that a negative first experience of a PE will influence future experiences and present barriers to wanting or receiving subsequent exams. 9 However, there is little qualitative research done to illuminate the patients’ experience of PE.
The aim of this study was to investigate women’s experiences during outpatient PE and identify potential areas to focus on when teaching PE to minimize patient discomfort and embarrassment.
Methods
Study design and participants
This qualitative study was conducted in the largest women’s and children’s hospital in Singapore from June 2020 till July 2021. Inclusion criteria were English speaking women aged 22 years to 80 years who have undergone a vaginal examination or transvaginal ultrasound within the past year. Patients who had similar procedures done due to pregnancy were excluded. Those with other procedures done like Hystero-Salpingo-Foam sonography (HyFoSy), IUCD insertion, colposcopy or have gynaecological cancer or surgery performed as well as those with sexual issues were also excluded. Purposive sampling was deployed to capture viewpoints from different demographic profiles.
Focus group discussions (FGDs), in-depth interviews (IDIs) and data collection
Participants who satisfied the criteria were provided with a participant information sheet detailing the study. The study’s Principal investigator went through the sheet with each participant face-to-face and obtained written informed consent before a scheduled interview. Participants were anonymized to ensure data confidentiality.
Questions used to guide IDI and FGD.

Analysis
Investigators analysed the data independently to identify emergent themes using the Grounded Theory. The investigators read the transcripts after the first two interviews and developed an initial coding framework manually. The codes were modified or expanded after each interview as the study progressed. No new code was identified after the eleventh IDI, implying idea saturation. This was confirmed by the last IDI. The coded data were grouped and organized in themes iteratively with reference to the hypothesis and the study’s objectives. Analysis software was not used.
The themes were summarized and presented to a focus group of staff, who were not part of the research team but involved in patient care. A few of the participants were also invited for their feedback and agreement. Majority of the staff and participants concurred with the key themes. The demographic data collection forms, audio recordings, transcripts, coding framework and codes were maintained in secure archives to establish a clear audit trail.
The study was approved by the Singapore Health Services Centralised Institutional Review Board (CIRB 2020-2327).
Results
Participant demographic characteristics.
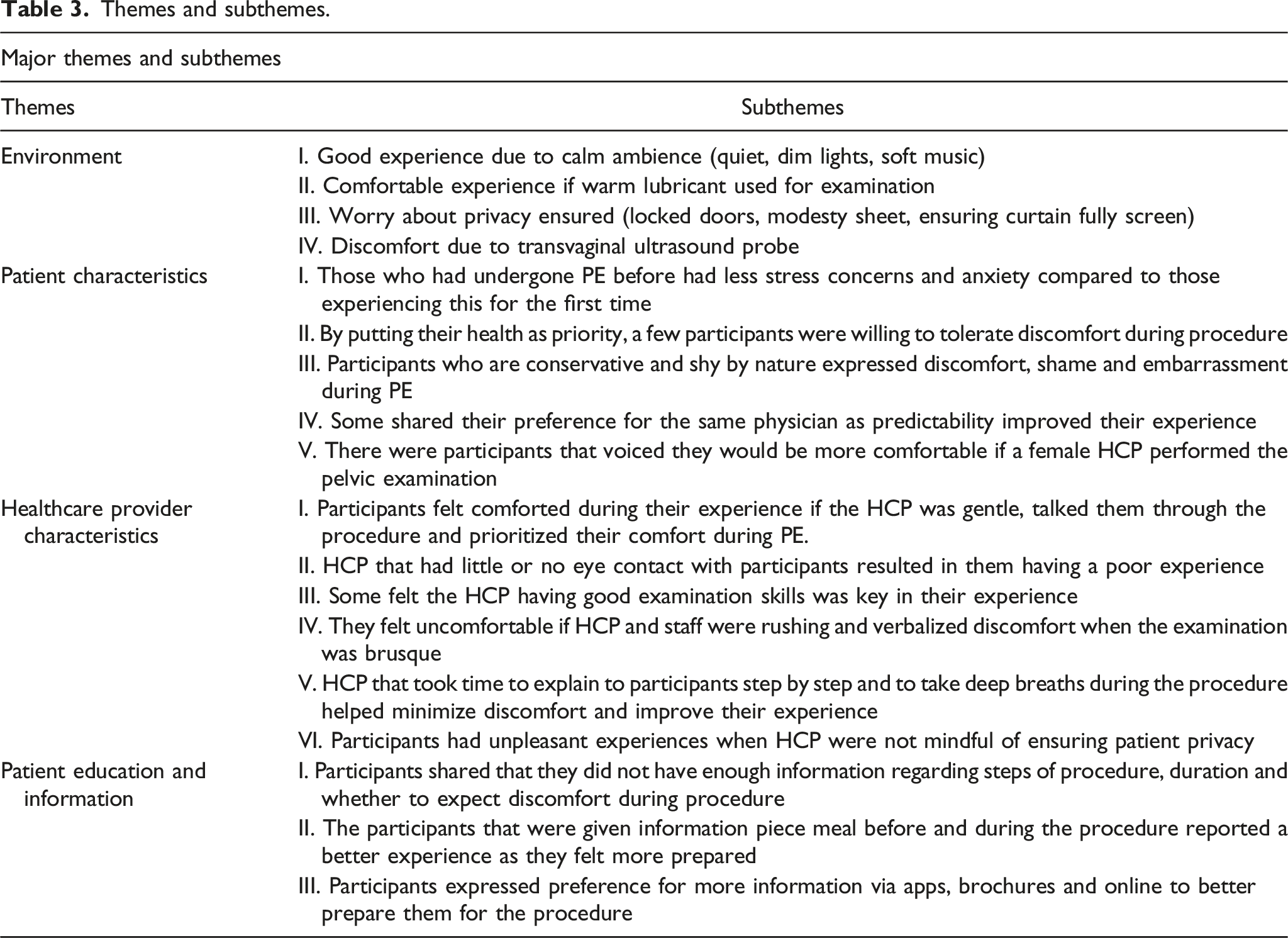
Themes and subthemes.
Clinics’ environment and physical set up
Participants identified that the environment of the hospital, namely the physical set up and equipment, at outpatient clinics had an impact on their experience. Soft lighting and ensuring the room was warm increased their comfort. A few participants felt vulnerable and exposed during PE and assurance of patient privacy was important to them. The transvaginal probe was mentioned often as a cause of discomfort, and some felt more comfortable if warmed lubricant was applied to the transvaginal ultrasound probe compared to if lubricant was not warmed up. The use of ambient music and aromatherapy were mentioned as suggestions to improve their experience. “And also ensure that the door is closed or whatever. Then, then dim down the light, you know especially when you lie down this, this ceiling light is right on, on to your eyes that will really make you very uncomfortable” “The first time when I had it, I was really a little bit shy and a bit embarrassed because I felt like you know, umm the curtain was I felt like it wasn’t fully closed even though there the door was locked…”
Patient’s individuality and characteristics
Disparities in patients’ experience may be related to the differing individual characteristics of patients such as demographic differences, sociocultural make up, personalities and prior experience. Participants who had undergone PE before and knew what to expect viewed their most recent experience as less stressful. Participants undergoing PE for the very first time, expressed concerns and challenges faced during their experience. Some were willing to tolerate a certain amount of discomfort during PE due to perceived benefits of this procedure and self-responsibility over one’s health. Participants stated they preferred a female HCP to perform PE as this would make them more comfortable. Some participants expressed preference for continuity of care with same physician for their routine PE. “The previous year, I had this PAP smear done and the doctor was very rough so after that I think I didn’t go for the check-up for years.” “Because I’ve been through it before, so the anxiety level wasn’t really there”
“I think it’s because it’s very new…it’s like the first time ever, maybe some kind of explanation would have helped”
“If it’s a gynae that I have visited more than twice then I will know this person’s style. But if it is a different gynae or a covering gynae then, you wouldn’t know how it will be like until it happens. So, the discomfort is the pain, it’s the err… how they asked you to position your leg, how much more to stretch…”
“So, I think in my position, I would say that “yes” to have a female gynae will feel more secure, feel safer, feel more comfortable to speak with. Maybe because I feel that she probably can feel what I am trying to say because she is also a female.”
Participants were aware that their requests to be examined by female HCP would not always be feasible. So, they suggested that male HCP take these extra measures improve their comfort level during PE.
These include: 1. Pre-empting the patient of the steps required during PE with instructions before and during examination. 2. Having a female assistant present during PE who could explain the steps to the patient during the examination. 3. Receiving reassurance from male HCP that he will be gentle, and patient’s modesty will be protected. 4. Allowing a female friend or family member present in the clinic room during the PE. 5. Providing a step-by-step explanation throughout the examination.
Healthcare provider characteristics and attitude
Participants discussed the relational aspects of care that affected their experience, such as, HCPs attitude and ability to provide emotional support, demonstrate empathy and communicate well. They shared examples of healthcare staff alleviating anxiety and distress with sensitivity and professionalism and ensuring that the patient’s dignity was protected. Participants wanted their providers to demonstrate genuine interest in their wellbeing and communicate with them throughout the procedure. They expressed their preference for providers to be well versed and polished in their examination skills. Some shared their bad experiences when HCPs rushed patients through the PE. Participants had better experience when assistants prioritised the patient’s comfort over assisting the physician. Discomfort occurred when providers did not respect patient’s privacy before the procedure.
“The doctor was very gentle, and the explanation was very clear. So, I don’t feel so nervous and during the procedure she keep asking me to, because I was having a lot of bleeding. So, she keeps asking me to relax take a deep breath. So, the assistant also holds my hand the other side because the bleeding was a lot. So, I, I feel so much better.”
“For me, I really expect a healthcare professional to look at me…First! Talk to me like you see my face and all that. I expect that, even if it’s a doctor doing the procedure without looking at my face, I will still be a bit taken aback.”
“I could overcome it because she did teach me how to do breathing in and out when the instrument is going in and all. But other than that, she didn’t speak to me and she like didn’t go through with me what’s happening next and what err to anticipate next…so that physical part and discomfort I felt …I wasn’t assured what’s going to happen next”
“The experience I would say, the person who is doing us must give us a very clear explanation, when they are doing it. Especially the transvaginal…sometimes they really poke very far in. So, the explanation is very important. So, some, they, they really can’t see. They just keep pushing”
“Okay, I think this, this doctor has so many cases, so, so she never prepared me, she just asked me to lie down,” Okay you lie down faster, expose yourself, I need to rush. I need to do a delivery”. So, she really rushes, that’s what she did. So, the experience was very bad, and she was very rough”
“I guess if they are there to provide…, emotional support or comfort to the patient but…, but if in the end they are also to attend to the Doctor’s request or whatever that is required from the procedure right, then, then the emotional support will actually be missed out.”
Patient information or education
Most participants described being left in the dark regarding the proceedings, duration, and possibility of discomfort during the procedure. Some commented that there wasn’t enough information about the ultrasound transvaginal probe used during the procedure. Most felt they would have been better prepared if they had received information about PE online, via apps or QR code or in a pamphlet form. They would have had a better experience if they could obtain information while waiting to see physician or sonographer in the clinic. The timing of when patients received information was an important consideration. Participants described preferring to receive information in a stepwise manner before and during the procedure.
“At the beginning I wasn’t expecting it to be quite as long as it took. So, it would have helped if the person the staff carrying out the procedure could have actually informed me about the duration…in my mind I was thinking when this is going to end.”
“I think it is very important that they explain what’s the next step, what to look out for, so, so that I am prepared… In this case, the nurse, and the doctor both are very clear in explaining what the next step is, so that there is nothing surprise to me”
“But I think if the medical team, or the sonographer team or what do you call that, give me a leaflet or a maybe brochure before the procedure starts and then I can just read through I can just see what I can expect and I can just read through what is it for, what are they looking for exactly…”
“An app, you know like through our phone, like an app, like a quick one, just like when you register with the scanner. Maybe even the app, you know there be like what to expect some like infographics would be awesome.”
Discussion
Results generated from the interviews in this study provide insights into patient expectations during a PE. Most participants had discomfort during PE. Themes and subthemes generated from our study concur with recommendations from other studies.
A calm clinic environment with warm lubricant during PE improved their experience. Patient discomfort can be minimized by utilizing the correct speculum size, adequate lubrication, proper positioning, providing privacy for undressing and draping the thighs. 10 Our study also showed that complementary techniques such as lavender aromatherapy and music therapy could also be considered. Special attention to the clinic environment such as warm lighting and ensuring privacy will make the patient more comfortable.
Interviews also uncovered those participants that prioritised HCP demeanour, communication, and examination skills during their experience. Participants in this study highlighted the importance of HCP taking their time and ensuring patient comfort during PE. We recommend that prior to the procedure or PE, HCPs should enquire if it is patient’s first time, inform the patient on the steps of the procedure and address any questions they might have. This is in keeping with previous studies where effective communication and shared, informed decision making is crucial for this sensitive procedure. 6 Our study shows that HCP should be sensitive to individual characteristics e.g., the first timers, those who have a prior bad experience or felt uncomfortable with male providers. Participants also felt more comfortable if female HCP were performing the PE. They shared important perspectives how male HCP could take steps to allay patient anxiety and improve comfort during a PE.
More information regarding PE before and during the procedure via online resources and pamphlets will help improve their experience.
Practical implications for medical education
This study has identified key issues faced by patients and the gaps and barriers in their care during PE to lead improvement in the delivery of care in this area and facilitate women’s positive experiences.
In Singapore there are no recommendations or guidelines available to raise the awareness of practitioners about the importance and the ways of making the PE more comfortable. This is particularly so for any patient’s first experience with PE. We hope that the findings of this study will be used in teaching programs and skills training for medical and allied health practitioners at all levels. HCP require adequate training in skills to help meet patients’ needs and foster a positive experience to encourage regular PE. Our study also highlights the importance of HCP education on improving procedure skills and communication skills in explaining the procedure, obtaining consent from patient, for which gaps in current training regimes should be addressed.
There are practical implications for medical education on patient centred improvements when training HCP involved in Women’s Health. Simple practices to improve the patient experience in other studies include using a disposable wrapped skirt as opposed to a drape, allowing for chaperones during the exam (particularly when the provider is male) and having the clinician ask for permission for each step of the exam. Other suggestions include forgoing the use of footrests, warming the speculum in advance, offering self-insertion of the speculum, and offering a mirror so the patient can see the exam. 11
Participants in this study preferred female HCP to perform this intimate examination and shared suggestions on how male physicians can make their experience a more positive one which should be incorporated during medical training. Studies have highlighted barriers and difficulties male medical students face when learning PE in clinical settings. An increased likelihood of patient refusal and ‘gate-keeping’ make their exposure limited and training challenging. 12
Some studies have found that medical students fear of hurting the patient, being judged inept by senior doctors, and missing clinical signs during PE. 13 However, later studies have shown that negative thoughts and fears dissipate in students as they get used to performing PE. 14 Graduate teaching assistant programs alongside mannequin simulations have been known to decrease fear and anxieties in medical students. 15 There is additionally a role in the use of innovation to teach HCP PE skills and communication via augmented and mixed reality.
Strengths and limitations
To our knowledge, this is the first qualitative study, exploring the experience of patients undergoing PE in Singapore. We attempted to decrease recall bias by recruiting participants that had underwent PE within the past one year. Patients who had antenatal scanning and vaginal examination during labour or underwent procedures such as HyFoSy or colposcopy or PE during emergencies were excluded from our study as these settings are considered more stressful due to urgency of the medical issues. Patients who had undergone cancer treatments and/or pelvic surgery and patients with existing sexual dysfunction were also excluded from this study.
Limitations of this study exists. Although participants were interviewed about their experience of the PE within a year after their visit to the clinic, ideally it would be best to collect feedback may be immediately after using services. Participants may find it difficult to remember the details unless discomfort was experienced during PE. Although data saturation was taken into consideration, the use of convenience sampling and having a small sample size with patients attending the same outpatient clinic, may have an impact on the generalisability of the results.
Suggestions for future research
The cultural factors that may shape a patient’s experience during PE that should be explored given the diversity of multi-ethnic Singapore. Patients who have experienced pain and discomfort during PE may benefit from Trauma-informed care (TIC). TIC has been used as a model of care for patients who have experienced physical, sexual, or emotional violence. Studies have identified TIC as a particularly important model of care during the PE, as the exam itself can mimic dynamics of abuse or violence. Further research would be useful to determine if this method is suitable for our patients locally and whether it minimises discomfort associated with PE. If so this model of care can be incorporated into syllabi. 16
Perspectives of HCP should be analysed to determine their concerns and barriers when performing PE on patients especially male students and doctors, who are less likely to get opportunities for PE. 17
A further multicentre study using mixed method approach of qualitative and quantitative methodology can give us a better understanding in both depth and breadth of how to improve patient’s experience of PE and transvaginal ultrasound. This will help in resource allocation and future studies can be implemented to track changes over time, as in the case of monitoring the outcomes of improvement initiatives.
There is also a necessity to explore experiences of subgroups of patients such as those with bodies or abilities that fall outside the medical definitions of ‘normal’ or ‘standard’ during PE. 18 PE is particularly important for women with high BMI as they have higher rates of cervical cancer and lower screening rates. 19 Studies examining PE experiences of patients with special needs is necessary. More research is also needed to understand the experience of patients’ who are part of the sexual and gender minority individuals to improve the access to comprehensive care.
Conclusions
This study has provided much needed data on the factors that contribute to a positive or challenging patient experience during PE in the outpatient clinics. Patient-centred care to ensure a positive experience includes the hospital environment, good communication of not just healthcare professionals but also the clinic staff. More work needs to be done to train clinic staff and HCP on improving communication and procedure skills. We also need to have systems in place to ensure patients receive information at every juncture for the procedure, feel more in control during PE and ensure greater patient involvement in decision-making. The patient perspective obtained from this study helped us understand patient expectations to make necessary changes to thereby improve compliance to these procedures.
Footnotes
Acknowledgments
The authors thank the patients for their invaluable contributions to this study.
Author contributions
JJMLL, RG, TTY, CC contributed to the study conception and design. JJMLL, CXY conducted the interviews. JJML, CXY, RG completed the initial data analysis. JJMLL and ASB wrote the first draft of the manuscript. CC and ZYT contributed to the data analysis and writing of this manuscript. JJMLL, ASB, TTY, CXY read and approved the final version.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Data availability statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.