
Abstract
Introduction
Since the introduction of the pericapsular nerve group (PENG) block technique by Giron in 2018, 1 several case reports have been published demonstrating its analgesic use in hip surgeries. 2 However, the PENG block alone does not cover the skin incision site and the nerve branches innervating the posterior aspect of the hip joint. Hence, the addition of a caudal epidural and lateral femoral cutaneous nerve (LFCN) block provides a more comprehensive block to ensure near-complete sensory coverage of the surgical site. In this case report, we used a combination of caudal epidural, PENG and LFCN blocks as an adjunct to opioid-sparing anesthesia for hip fracture surgery in a high-risk geriatric patient with severe aortic stenosis. This manuscript adheres to the CARE guidelines for case reports, and the patient has given written consent to publish this case report.
Case description
Our patient was an 87-year-old, 55 kg Chinese female who suffered a left intertrochanteric fracture after a fall that was precipitated by giddiness. She was planned for a surgical fixation of the left hip. During the preoperative assessment, a history of recent decreased effort tolerance was elicited and an incidental finding of an ejection systolic murmur was discovered. Transthoracic echocardiography revealed severe degenerative aortic stenosis with an aortic valve area of 0.98 cm2.
In view of her severe aortic stenosis and advanced age, our technique of choice was an opioid-sparing general anesthetic combined with three nerve blocks – Caudal epidural, PENG and LFCN blocks.
The patient was sedated with IV Fentanyl 25 mcg. Caudal epidural catheter insertion was performed with the patient in a right lateral position under ultrasound guidance. 3 cm of epidural catheter was left in space and a test dose of 2 mL of 1% Lignocaine was given to exclude an inadvertent intrathecal spread. After observing hemodynamic stability over 10 min, another 4 mL of 0.5% Bupivacaine was given as a slow bolus.
The patient was then turned supine and an ultrasound-guided PENG block was performed over the left hip. As the patient’s habitus was slight, a linear ultrasound probe (6-13 MHz) provided adequate visualization of the femoral vessels and nerve, iliopsoas muscle, ilium, and iliopubic eminence. (Figure 1) A 100 mm 21G Stimuplex needle was inserted in an in-plane approach from lateral to medial, and 18 mL of 0.5% Bupivacaine was deposited between the iliopsoas muscle and iliopubic eminence. Ultrasound Image of PENG Block. FV: Femoral vein; FA: Femoral artery; FN: Femoral nerve; IP: Iliopsoas muscle; IPE: Iliopubic eminence; AIIS: Anterior inferior iliac spine; Area highlighted in yellow: Area of deposition of local anesthetic; White arrow denotes the needle position. PENG: Pericapsular nerve group; LFCN: Lateral femoral cutaneous nerve; MAC: Minimum alveolar concentration; NRS: Numerical rating scale.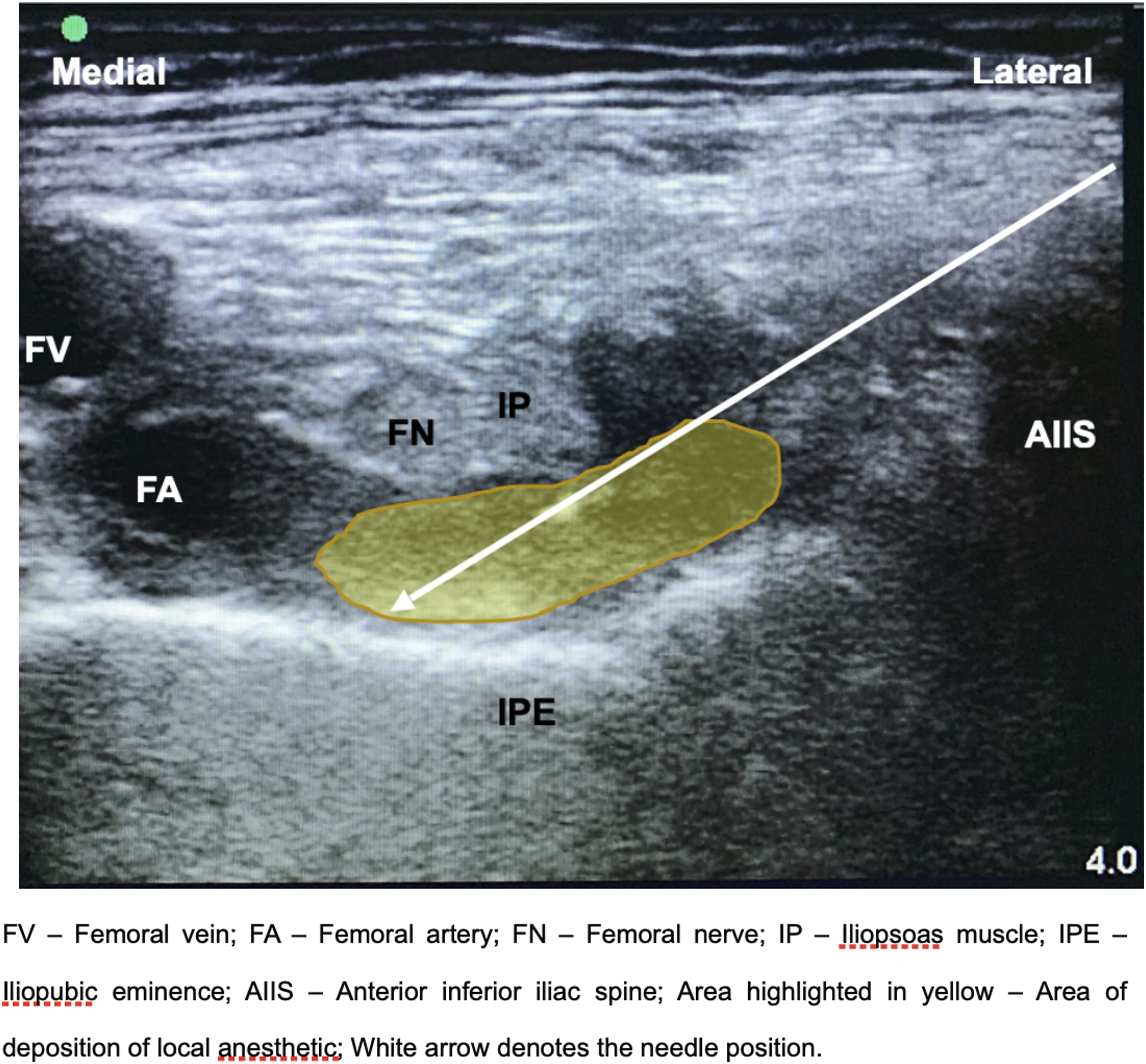
The LFCN block was then performed while in supine position using the linear ultrasound probe. The LFCN was identified with the sartorius muscle medially, tensor fascia lata muscle laterally and the fascia lata superficially (Figure 2). 2 mL of 0.5% Bupivacaine was deposited around the nerve. Upon completion of the blocks, the patient reported no further hip pain. Ultrasound Image of the Lateral Femoral Cutaneous Nerve. Sa: Sartorius muscle; TFL: Tensor fasciae latae muscle; White arrow denotes the lateral femoral cutaneous nerve; Yellow arrow denotes the fascia lata.
In view of possible prolonged surgery, we opted for a co-induction of general anesthesia with inhalational sevoflurane and IV Propofol 30 mg. A laryngeal mask airway was inserted and anesthesia was maintained with nitrous oxide 60% and sevoflurane titrated to a MAC of 0.8. IV Parecoxib 40 mg was given as part of multimodal analgesia. No vasopressors were required throughout the surgery and no additional opioids were needed for the entire 90 min of the surgery.
The patient was monitored in the post-anesthesia care unit for 1 hour. She was comfortable and did not require any analgesics. Prior to discharge, 6 mL of 0.5% Bupivacaine was administered through the caudal epidural catheter before it was removed. On the first post-operative day, she was able to ambulate with assistance. Reported pain scores were 0 at rest and 2 on ambulation using the 11-point Numerical Rating Scale (NRS). She was given simple analgesics such as oral Paracetamol for postoperative analgesia. No adverse effects from the regional blocks were observed.
Discussion
The hip fracture patient population consists predominantly of elderly patients, many of whom have multiple comorbidities. Uncontrolled pain in the geriatric patient is associated with increased stress response, sleep disturbance, cognitive impairment and functional decline.3,4 However, due to the physiological and pharmacokinetic changes related to aging, systemic opioids carry an increased risk of adverse events, 3 and are associated with cognitive decline and delirium. 5
Central neuraxial techniques, such as spinal or epidural anesthesia, are commonly used in hip fracture surgeries to avoid the need for opioids, but this technique is often avoided in patients with severe aortic stenosis due to the risk of significant hypotension from a reduction in systemic vascular resistance. Peripheral regional anesthesia for hip fracture patients has been shown to effectively reduce pain scores and opioid consumption. 6
Various regional block techniques have been used to target the nerves supplying the hip joint. As the sensory innervation of the hip is complex, blockade of multiple nerves may be required to adequately control intraoperative and postoperative pain. Innervation of the anterior capsule of the hip joint involves the sensory articular branches of the femoral nerve, articular branches of the obturator nerve and the accessory obturator nerve, while the posterior capsule is innervated by the articular branches of the sciatic nerve.7,8 Hence, effective sensory blockade of the hip joint should include the femoral nerve, obturator nerve and sciatic nerve.
The PENG block is a relatively new regional anesthesia technique that covers the pericapsular articular nerves of the anterior aspect of the hip capsule. 9 In a case series by Acharya, 2 the use of PENG blocks enabled hip fracture patients to sit upright for a subarachnoid block with reduced discomfort. As the PENG block can be performed in the supine position, it improves patient comfort during positioning for surgery. The LFCN block was performed to provide sensory coverage of the skin incision site over the hip. This can be performed easily in the same setting, as the site of injection is near that of the PENG block and does not require a change in the patient’s position. A low-dose (6 mL) caudal epidural was added to cover the origin of the sciatic nerve from L4 and below. Using a combination of all three blocks, the sensory innervation of both the hip joint and surgical incision site are completely covered, removing the need for systemic opioids. There are no cases reported in the literature of this combination of regional blocks in hip surgery.
The goals of anesthesia in aortic stenosis include maintenance of preload, afterload, myocardial contractility and avoidance of tachycardia. With the combination of the three regional blocks, the near-complete sensory blockade of the surgical site prevented the pain-induced tachycardia that can be detrimental to those with severe aortic stenosis. By reducing the sensory response to surgical stimulus, lower doses of volatile anesthetics were also required for the maintenance of general anesthesia. This minimized the dose-dependent depressant effects of anesthetic drugs on myocardial contractility. 10 As the volume and dose of local anesthetic given through the caudal was small, a significant drop in systemic vascular resistance from sympatholysis is unlikely.
The regional block combination allowed our patient to ambulate on postoperative day 1 with minimal discomfort. This is of great benefit for our patient as early weight-bearing after surgery for hip fractures has been associated with improved recovery outcomes and lower mortality risks. 11
The main limitation of our technique is the need for three regional blocks, which subjects the patient to more invasive procedures and hence, a higher risk of complications. The use of caudal epidural for perioperative analgesia in adults has also declined over the years and is a technique that the newer generation of anesthesiologists has become less familiar with. An alternative to our low-dose caudal epidural is the parasacral sciatic nerve block. However, the large volume of local anesthetic required limits its use when applied in combination with other regional blocks, as the risk of local anesthetic toxicity is increased.
In this climate of enhanced post-surgical recovery, regional anesthesia is part of a multi-dimensional approach to improve recovery through optimization of pain control, permitting early ambulation and avoiding the adverse effects of opioids. This case report demonstrates a safe technique of complete sensory coverage for hip fracture surgery in a high cardiac risk patient using a combination of three regional blocks – low-dose caudal epidural, PENG and LFCN blocks.
Footnotes
Author contributions
Elizabeth SJ TAN.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Data Availability Statement
Availability of data, Availability of data: Data sharing is not applicable to this article as no datasets were generated or analysed during the current study.