
Abstract
Background
Hip fracture is a common reason for elderly admission to hospital and majority of patients will require a hip fixation surgery. Pain originating from a hip fracture is usually severe and the need to improve comfort is paramount, especially before the hip fixation surgery because severe pain results in unnecessary stress response such as catecholamines release, tachycardia and hypertension. This worsens outcomes, increases risk of complications such as myocardial ischaemia, strokes, pulmonary embolus or deep vein thrombosis. Multimodal systemic analgesia has been shown to be effective in reducing pain in hip fractures but the associated side effects and contraindications have accelerated the adoption of nerve blocks in the peri-operative management of hip fracture patients. 1 As a result, this has been increasingly recognised as a important component of the hip fracture pathway (as part of a multimodal approach for analgesia) and many hospitals have protocols to perform various interventional therapies (various nerve blocks) for newly admitted patients with hip fracture to alleviate pain immediately and potentially provide intra and post-operative analgesia.
Objective
The aim of this review is to elucidate the various interventional therapies currently available (including pericapsular nerve group (PENG) block which was first described in 2018), their evidence and the pros and cons.
Methods
We reviewed the latest evidence for femoral nerve block (FNB), 3-in-1 block, lumbar plexus block (LPB), fascia iliaca block (FIB), erector spinae plane block (ESPB) and pericapsular nerve group (PENG) block.
Results and conclusion
Each block has its pros and cons, as discussed in this review article. The procedurist should deliberate these considerations before deciding which block is most appropriate.
Clinical impact
What is New ◦ Pericapsular nerve group (PENG) block is a novel technique (first described in 2018) to block nerve supplying the hip joint to reduce pain associated with hip fractures ◦ We review the current literature on PENG block against all other available interventional therapies for hip fracture pain reduction
Clinical implications
◦ Many hospitals have hip fractures protocols which incorporate blocks to reduce pain associated with hip fractures to reduce pain and improve outcome ◦ Our review article summarises all available interventional technique to date, discuss their pros and con and make recommendations for factors to consider when deciding which blocks to perform.
Highlight: We review all available and most updated techniques for interventional therapies for management of hip fracture pain.
Context
Hip fracture is a common reason for elderly admission to hospital and majority of patients will require a hip fixation surgery. Pain originating from a hip fracture is usually severe and the need to improve comfort is paramount, especially before the hip fixation surgery because severe pain results in unnecessary stress response such as catecholamines release, tachycardia and hypertension. This worsens outcomes, increases risk of complications such as myocardial ischaemia, strokes, pulmonary embolus or deep vein thrombosis. In addition, good pain relief also aids the operative team (Surgeons, Anaesthetists and Nurses) in transfer of the patient from the ward to operating theatre and positioning of patient for performance of spinal anaesthesia. Multimodal systemic analgesia has been shown to be effective in reducing pain in hip fractures but the associated side effects (such as opioid induced drowsiness) and contraindications (NSAID not being suitable for the elderly and renal impaired patients) have accelerated the adoption of nerve blocks in the peri-operative management of hip fracture patients, in conjunction with other modalities of multimodal analgesia.1,2 As a result, this has been increasingly recognised as an important component of the hip fracture pathway and many hospitals have protocols to perform various interventional therapies (various nerve blocks) for newly admitted patients with hip fracture to alleviate pain immediately and potentially provide intra and post-operative analgesia. The aim of this review is to elucidate the various interventional therapies currently available, their evidence and the pros and cons.
Relevant anatomy
Hip joint
The hip joint consists of a ball (femoral head) and socket (acetabulum) with the femoral head, neck, and greater and lesser trochanters comprising the proximal end of the femur. The psoas major muscle originates from the vertebral bodies of T12–L4 and costal processes of the L1–L5 vertebrae and merges with the iliacus muscle (which originates from the inner surface of the iliac bone) before inserting into the lesser trochanter. The greater trochanter provides the insertion for gluteus medius and gluteus minimus muscles. 3
Innervation of the hip joint
The sensory nerve supply to the hip joint includes the femoral nerve (FN), obturator nerve (ON), articular branches of the sciatic nerve, nerves supplying quadriceps muscles, and superior gluteal nerve. Sensory innervation of the skin on the lateral thigh is supplied by the lateral cutaneous nerve of thigh (LCNT) and by the lateral cutaneous branch of the subcostal nerve. Sensation to the upper anterior portion of the thigh is supplied by the ilioinguinal and genitofemoral nerves. The FN, ON, and LCNT arise from the lumbar plexus, whereas the sciatic nerve, nerve supplying quadriceps muscles, and superior gluteal nerve arise from the sacral plexus. 3
Aetiology of hip fracture pain
Broken hips are painful for a variety of reasons. The nerve endings that surround periosteum contain pain fibres and these fibres may become irritated when the bone is broken or bruised. Also, muscles that surround the injured area may go into spasm when they try to hold the broken bone fragments in place, and these spasms may cause further pain. Lastly, broken bones bleed, and the blood and associated swelling (oedema) cause pain.
Therefore, in addition to blocking the nerve endings of the hip, certain interventional therapies may further reduce pain by partially blocking motor function of the hip joint, reducing unnecessary movement which worsens pain by causing spasms and potentially exacerbate the fracture.
Interventional therapies (from oldest to latest)
Femoral nerve block (FNB)
Background
First Described in 1952, FNB is the oldest technique described here. 4 The femoral nerve is among the largest branches of the lumbar plexus and it arises from the ventral rami of the L2, L3, and L4 spinal nerves. It is relatively easy to perform and the FN at inguinal ligament can be clearly visualised using ultrasound. Unfortunately, as the FNB only blocks the FN and no other nerves (such as ON or LCNT), studies have shown FNB to be the least efficacious amongst the techniques described here. 5
Technique
Landmark and Nerve-Stimulation approach
In supine position, the inguinal ligament is identified between the anterior superior iliac spine and pubic tubercle. 6 The femoral artery can be palpated just below the femoral crease. The needle is inserted approximately 1 cm lateral to the femoral artery pulse in a cephalad direction. The expected depth of the femoral nerve is 2–4 cm (though may be variable depending on body habitus), and can be combined with a nerve-stimulation technique for a more precise location. Approximately 10–20 mL of local anaesthetic (LA) injected is sufficient to achieve an adequate block.
Ultrasound-guided technique
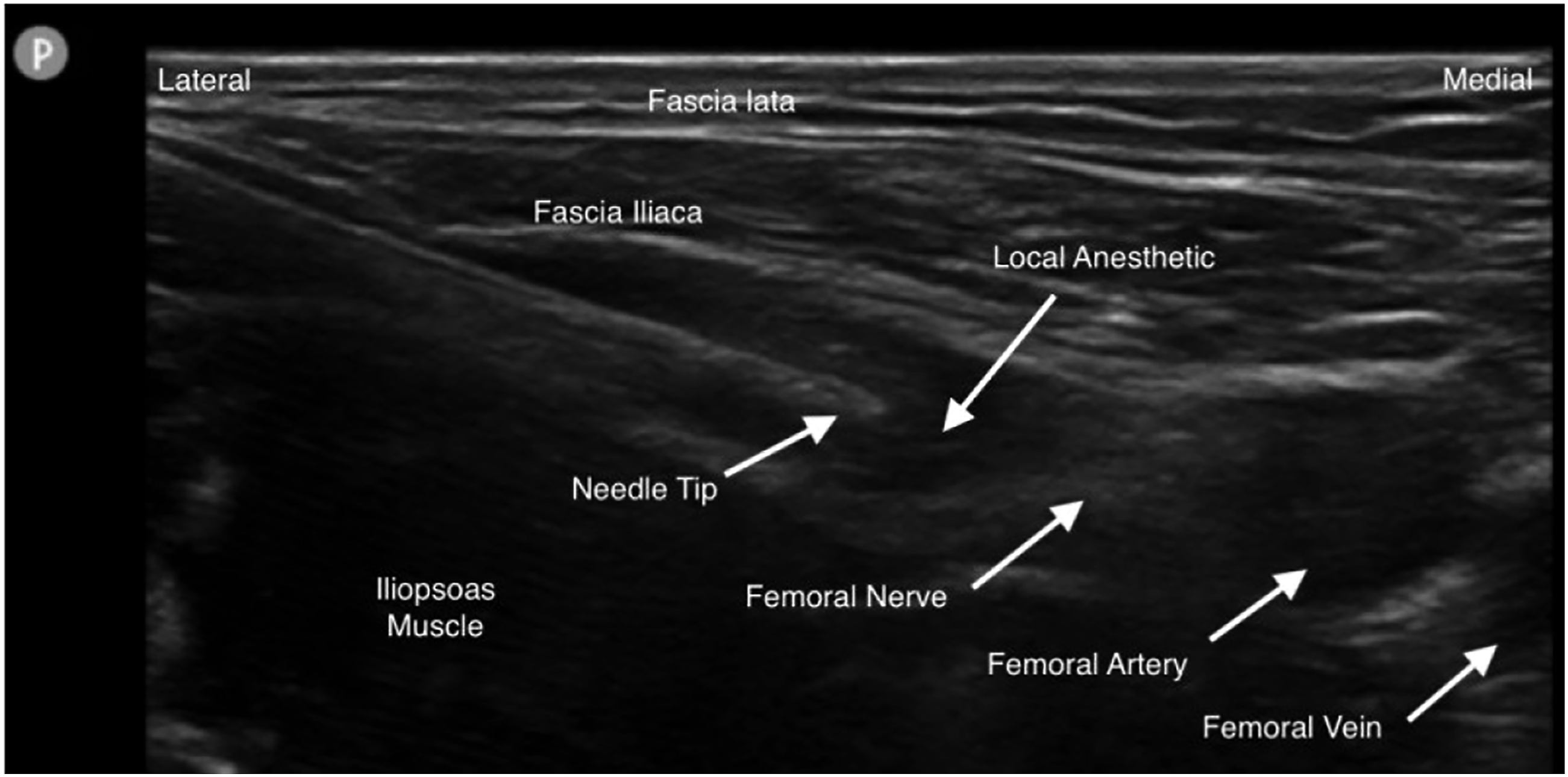
In supine position, the transducer is placed transversely at the inguinal crease, and the femoral vessels are located. Immediately lateral to the femoral vessels, the femoral nerve classically appears as a hyperechoic wedge or ovoid structure. The femoral nerve is superficial to the iliopsoas muscle group and it is deep to the fascia lata and fascia iliaca, respectively.
The needle tip is advanced below the fascia iliaca towards the femoral nerve. Either an in-plane or out-of-plane approach may be used, depending on the procedurist’s preference. The ultrasound monitor will show the spreading of LA injection around the femoral nerve (Figure 1). Approximately 10–20 mL of local anaesthetic (LA) injected is sufficient to achieve an adequate block. In-plane Femoral Nerve block image under ultrasound.
6
Evidence
The quantity of evidence supporting pre-operative single-shot FNB for hip fractures is very low, and the certainty of evidence supporting pre-operative single-shot FNB for hip fractures is low. 5 5 randomised controlled trials (RCT) studying use of non-ultrasound guided FNB for hip fracture pain control were identified and the average pain score reduction was 2.13 (statistically significant). 5 No studies using ultrasound guided technique were identified. One study demonstrated that nerve-stimulator versus ultrasound guided FNB have equal success rates though the ultrasound guided technique had a shorter procedural time and hence lower need for rescue dose of morphine. 7
3-in-1 block
Background
Described by Winnie in 1973, this technique is similar to FNB except that a larger volume of LA is used and manual pressure is applied distal to the site of injection in order to encourage the LA to spread proximally in the fascial plane between the iliacus muscle and fascia iliaca. 8 In essence, it was thought that this technique may result in the blockade of the FN, ON and LCNT as these nerves were thought to reside in the same fascial plane.
Technique
Same as FNB but a larger volume of LA is deposited, approximately 20–40 mL of LA. 9
Evidence
A prospective observational study has shown that 3-in-1 block inconsistently blocks the ON (4% chance of blocking the ON). 10 One RCT showed significant reduction in patients’ morphine requirement but this study included patients with distal femur fracture. 11 Also, a pilot study conducted in 2015 did not show 3-in-1 block to be more effective than IV morphine in reducing pain score as a primary outcome. 12
Lumbar plexus block (LPB) also known as Psoas compartment block (PCB)
Background
Chayen et al. developed this approach in 1976 to deposit LA at the lumbar plexus based on the fact that most of the branches of the lumbar plexus and some of the sacral plexus supplying the thigh are found close to each other in the region of the fourth lumbar vertebra in what they described as the “psoas compartment”. 13 Hence, the aim of LPB is the deposition of LA to result in a spread of the injectate within the body of the psoas muscle around the lumbar branches (L2–L4), with cephalad spread to the lumbar nerve roots.
Technique
Landmark technique
The site of needle insertion is determined as follows. A line is drawn connecting the iliac crests (intercristal line). 14 The spinal processes (SPs) are marked and posterior superior iliac spine (PSIS) is identified. A line through the PSIS is drawn parallel to the line joining the SPs. The site of needle insertion is at the junction of the lateral third and medial two thirds of a line between the SPs and the PSIS and 1 cm cephalad to the intercristal line (L4). The needle is inserted perpendicular to all planes. A 100 mm stimulating needle is inserted connected to a nerve stimulator with a starting output of 1.5 mA and 2 Hz. The needle is advanced until quadriceps muscles twitches are elicited or bony contact (presumed to be transverse process of L4) is made. If bone is encountered, the needle is withdrawn and directed caudad under the transverse process and advanced no further than 15–20 mm, until twitches of the quadriceps muscles are elicited with currents between 0.3 and 0.5 mA. After negative aspiration, approximately 20 mL of LA is injected incrementally over 3–5 min with regular aspiration for blood or cerebrospinal fluid (CSF).
Ultrasound guided technique
Many techniques available in both sagittal and transverse plane. The “Shamrock method” will be described here. 15
A transverse scan is performed at the flank and immediately above the iliac crest, with the patient in the lateral position and with the side to be blocked uppermost. Once the sonographic pattern of the “shamrock” is obtained at the level of the L4 transverse process, the ultrasound transducer is tilted slightly caudally until the acoustic shadow of the transverse process is no longer visualised.
This view represents the transverse view of the anatomy relevant for LPB through the L4–5 intertransverse space (Figure 2).
16
A line is then drawn on the patient’s back extending from the center of the medial end of the transducer to the midline (back). A nerve block needle is inserted 4 cm from the midline along this line and gradually advanced anteriorly under real-time ultrasound guidance (in-plane needle insertion) until the needle tip is close to the L3 nerve root. Nerve stimulation should be used in conjunction with ultrasound to confirm correct needle placement, after which approximately 20 mL of LA is injected slowly while visualising the perineural spread of the drug in the posterior aspect of the psoas muscle. Transverse sonogram of the lumbar paravertebral region during the Shamrock method.
16

Evidence
LPB has been shown to be as effective as epidural block for analgesia after total hip arthroplasty, but with less nausea, urinary retention, motor block, and orthostatic hypotension. 17 Also, Amiri et al. successfully provided surgical anaesthesia for hip surgeries with LPB in conjunction with a light sedation and outcomes were favourable in patients’ satisfaction, haemodynamic stability with no complication. 18 However, Auroy et al. found higher incidence of severe complication (i.e. intravascular injection or bilateral anaesthesia such as epidural or intrathecal) compared with femoral nerve block. 19
Fascia iliaca compartment block (FIB)
Background
First described by Dalens et al. in 1989, FIB is a popular technique to achieve analgesia in hip fracture surgery because it covers the lateral cutaneous nerve of the thigh (LCNT) which provides analgesia over surgical incision for hip surgeries. 20 The fascia iliaca compartment is a potential space lying between the fascia iliaca anteriorly and the iliacus and psoas muscles (iliopsoas) posteriorly. 20 FN, ON, LCNT and potentially genitofemoral nerve course through this potential space (at the proximal end of their anatomical course) so the deposition of LA blocks these nerves to provide analgesia for hip fracture pain. Nonetheless, anatomical studies have shown that ON lies outside the fascia iliac compartment and it is unlikely that the FIB will be able to cover the ON. 21
Technique
Landmark, ultrasound guided infrainguinal and suprainguinal techniques have been described. 22
Landmark approach
After positioning the patient supine, a line connecting the ASIS and the pubic tubercle is divided into thirds. The injection is performed at a point 1 cm caudad to the junction of the lateral third and medial two thirds. The ipsilateral femoral pulse is palpated approximately 1.5 cm medial to the point of injection. A blunt, short-bevel needle is inserted perpendicular to the skin and the needle angle adjusted to approximately 60 and directed cranially. A ‘give’ or ‘pop’ may be felt as the needle passes through fascia lata, and a second ‘give’ as it passes through the fascia iliaca. The needle angle is adjusted to approximately 30° and advanced a further 1–2 mm. Approximately 10–20 mL of LA should be injected without experiencing resistance.
Ultrasound guided infrainguinal approach
In supine position, the linear probe is placed transversely to identify the femoral artery at the inguinal crease. The iliopsoas muscle with the overlying fascia iliaca is identified and the hyperechoic FN is typically seen lying between the iliopsoas and fascia iliaca at a depth of approximately 2–4 cm, lateral to the femoral artery (Figure 3). A blunt short-bevel needle is inserted using an in-plane technique with the aim of placing the needle tip beneath the fascia iliaca around the lateral third of a line between the ASIS and pubic tubercle. Correct needle placement is confirmed by separation of the fascia iliaca from the iliopsoas muscle with LA spreading towards the FN medially and the iliac crest laterally. Approximately 10–20 mL of LA should be given. Ultrasound image of the fascia iliaca (white line and arrows) at the level of the inguinal ligament. The femoral nerve (FN) and femoral artery (FA) are visualised on the medial side and the sartorious muscle (SM) on the lateral side.
22

Ultrasound guided suprainguinal approach
In supine position, the linear probe is placed sagittal to the inguinal ligament to obtain an image of the ilium and iliacus muscle. The probe is then moved laterally and superiorly along the inguinal ligament towards the ASIS to lie laterally to the FN. The deep circumflex artery is identified superficial to the fascia iliaca and approximately 1–2 cm cephalad to the inguinal ligament, and this provides a further landmark for needle placement. The needle is inserted approximately 2–4 cm caudad to the inguinal ligament aiming ultimately to be beneath the fascia iliaca, cephalad to the inguinal ligament. LA spread should be seen between the fascia iliaca and iliacus muscle and into the iliac fossa (Figure 4). Approximately 10–20 mL of LA should be given. Ultrasound guided suprainguinal approach to the fascia iliaca compartment block. Injection of local anaesthetic under fascia iliaca shown here.
22

Evidence
Dalens et al. described in 1989 that FIB was able to provide superior analgesia in 60 children age 0.7–17 years undergoing lower limbs surgeries compared with 3-in-1 block. 20 RCTs demonstrated statistically significant decrease in morphine consumption and increase in patient-reported satisfaction for patients who received FIB before hip fixation surgery.20,23,24 In addition, a metaanalysis in 2018 revealed that the analgesic effect of FIB was superior to that of opioids during movement, resulted in lower pre-operative analgesia consumption and a longer time for first request, and reduced time to perform spinal anaesthesia. 25
Erector spinae plane block (ESPB)
Background
First described by Forero et al. in 2016 for the treatment of chronic thoracic neuropathic pain and post-operative pain in thoracic surgery, ESPB is a paraspinal fascial plane block in which the needle placement is between the erector spinae muscle and the thoracic transverse processes. 26 Typically, 20–30 mL of LA is administered, blocking the dorsal and ventral rami of the thoracic and abdominal spinal nerves.
Technique
The ESPB is most often performed between the T5-T7 paraspinal levels, but it can be performed at the lower lumbar region to provide analgesia for hip fractures. 27 To perform this, a curvilinear ultrasound transducer is placed in a sagittal orientation over the midline of the back at the desired level. The probe is then translated laterally until the transverse process is observed. In this view, the erector spinae muscle may be observed lying superficial to the transverse process. A block needle is then inserted in a cephalocaudal direction using an in-plane approach until the needle contacts the transverse process. Hydrolocalisation is then performed with the lifting of the erector spinae muscles off the transverse process indicating proper needle placement. In this plane, between 20 - 30 mL of LA may be administered.
Evidence
The overall evidence for the use of ESPB for hip fracture is scant and limited largely to case series. The largest case series was reported by Ahiskalioglu et al. who described the successful use of ESPB at the level of the L4 transverse process with mild sedation as the anaesthetic technique for 15 patients undergoing hip fracture surgery. 28 This technique resulted in good operating conditions and minimal post-operative pain in all the patients. One patient received a contrast-enhanced magnetic resonance imaging (MRI) study which demonstrated that the likely mechanism by which the ESPB worked was via spread to the psoas muscle (and lumbar plexus), epidural spread and transforaminal nerve root spread. Another case report in 2021 described a patient achieving mean pain score of 2.8 over 24 h after hip fixation surgery, receiving only lumbar ESPB and paracetamol. 29 While lumbar ESPB shows some promise, there is currently insufficient evidence to support the routine use of ESPB for hip fracture.
Pericapsular nerve group (PENG) block
Background
First described by Girón-Arango et al. in 2018, PENG block was devised as a novel technique to target articular branches of anterior ON and FN between anterior inferior iliac spine (AIIS) and the iliopubic eminence (IPE) as these branches were inconsistently blocked by other block techniques. 30 PENG block was described as a technique to anaesthetise the anterior hip joint. The deposition of LA in a plane between the pubic ramus and psoas tendon results in the spread of LA around the anterior joint capsule, resulting in the blockade of the terminal sensory branches of the anterior hip joint - which are namely, branches of the FN, ON and accessory ON.
Technique
In the supine position, a curvilinear low-frequency ultrasound probe (2–5 MHz) is placed in a transverse plane over the AIIS and then aligned with the pubic ramus by rotating the probe clockwise/counterclockwise (depending on right/left side respectively) approximately 45°.
30
In this view, the IPE, iliopsoas muscle and tendon, femoral artery, and pectineus muscle can be seen simultaneously (Figure 5). The needle is then inserted from lateral to medial in an in-plane approach to place the tip in the musculofascial plane between the psoas tendon anteriorly and the pubic ramus posteriorly. Following negative aspiration, the LA is injected in 5 mL increments while observing for adequate fluid spread in this plane for a total volume of approximately 20 mL. The figure on the left shows the needle position. The needle is outlined by the arrows. The figure on the right shows the LA spread following injection. FA indicates femoral artery; LA, local anaesthetic; PE, pectineus muscle.
30
*Psoas tendon. Reproduced with permission from BMJ. FA: femoral artery; LA: local anaesthetic
Evidence
Although PENG block is a relatively new technique, there has been 4 RCTs and some case reports on this topic with many trials registered and ongoing. In the study by Girón-Arango et al., the average pain score reduction was 3.4 but study population was small at 5 subjects. 30 Another small study by Sahoo et al. showed that 5 out of nine patients who underwent PENG block after a hip fracture had no pain within first 24 h of receiving PENG block. 31 Another randomised trial by Aliste et al. comparing PENG and FIB revealed that PENG block resulted in lower incidence of quadriceps muscles blockade (45% vs 90%) at 3 h post block but dynamic pain scores were similar. 32 Lin et al. compared PENG versus FNB block in 60 patients and the PENG group had higher percentage of patients with no pain post-operatively (63% vs 30%). 33
Unlike FIB and FNB, PENG block theoretically targets the pain carrying articular branches and therefore eliminates the risk of motor weakness produced by FIB and FNB. However, a scoping review reported cases of transient motor blockade associated with PENG block and the possible reasons were wrong needle placement or tracking of LA in cephalic direction into the lumbar plexus. 34
Discussion
Meta-analysis by Ritcey et al. has shown that regional nerve blocks (FIB, FNB, 3-in-1 block) provided better analgesia than standard pain control regimens, reduced the need for intravenous opioid medications for primary outcomes. 35 In addition, Guay et al. reported peripheral nerve blocks reduced pain on movement within 30 min of block placement, demonstrating that analgesia for hip fracture with nerve blocks can be achieved in a timely manner. 36 In terms of secondary outcomes, there is reduced risk of delirium, chest infection and time to first mobilisation. 36 Overall, high-quality evidence shows that regional blockade reduces pain on movement within 30 min after block placement and moderate-quality evidence shows reduced risk for pneumonia, decreased time to first mobilisation and cost reduction of the analgesic regimen. 37
Ritcey et al. and Guay et al. conducted comprehensive reviews in 2015 and 2020 respectively but no PENG block trials were included due to lack of quality studies.35,36 While we await further quality studies to conclude for the next meta-analysis to include the PENG block, this paper is the first one to compare current evidence available for all the various peripheral nerve blocks available for hip fracture pain management, including the PENG block.
The next issue involves choosing the most effective technique to improve outcomes in patients with hip fractures. Each technique has its advantages and disadvantages so it is crucial the procedurist is aware so that the most appropriate technique can be performed for the individual patient. The factors to consider are: - Expertise of procedurist: Technique such as PENG is newer and many procedurists may not be as familiar compared with other techniques. - Requirement for motor blockade: Though motor blockade is generally detrimental to post-operative recovery/physiotherapy, lack of muscle movement pre-surgery may be beneficial to reduce pain secondary to muscle spasm. One trial has shown that PENG block results in lower incidence of quadriceps muscles blockade compared with FIB.
32
- Need for preservation of nerve block catheter for post-operative analgesia: FIB insertion site is closest to surgical field so a FIB catheter is likely to either be removed by surgeon or risk being dislodged during surgery or removal of drapes. - Availability of ultrasound: In an environment where ultrasound is not readily available, the procedurist may want to consider performing blocks with well described landmarks techniques, such as FIB, FNB or 3-in-1 block. - Location of hip fracture: Extra-articular hip fractures may respond better to FIB than PENG block.
Conclusion
In Singapore, one in six adults aged 60 and over dies within 12 months of suffering a hip fracture. 38 In another study, Older adults have a five-to-eight times higher risk of dying within the first 3 months of a hip fracture compared to those without a hip fracture. 39 One of the reasons may be the detrimental effect of pain and or due to side effects of analgesia such as renal impairment from NSAID or respiratory depression from opioids. Despite the effectiveness of nerve blocks in managing hip fracture pain, it is necessary to recognise that a single nerve block may not suffice as the sole mode of analgesia and a multimodal technique should remain a priority. In formulating a multimodal strategy for hip fracture analgesia, it may be helpful to consider the interventional therapies discussed in this article to reduce the use of systemic analgesia, and also improve functional capacities which will reduce morbidity and mortality.
Footnotes
Author’s contributions
LZW: Drafted the article and made a substantial contribution to the concept or design of the work; or acquisition, analysis or interpretation of data. CLWY: Made a substantial contribution to the concept or design of the work; or acquisition, analysis or interpretation of data. DCXH: Made a substantial contribution to the concept or design of the work; or acquisition, analysis or interpretation of data.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Not applicable
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Not applicable
Appendix
Annex 1
FA: femoral artery; LA: local anaestheti; FIB: fascia iliaca block; ESPB: erector spinae plane block; PENG: pericapsular nerve group; LCNT: lateral cutaneous nerve of thigh; RCT: randomised controlled trials.
Block
Primary author (Year)
Outcome
Pros
Cons
FN
Skjold 2020
5
Decreased pain score versus systemic analgesia
- Ease of performing
- Motor blockade may be beneficial in avoiding muscle spasm secondary to pain- Does not cover other nerves
3-IN-1
Graham 2015
12
Not more effective than IV morphine
- Ease of performing
- Inconsistent coverage of nerves other than FN
Lumbar plexus block
Turker 2003
17
Auroy 2002
19
As effective as epidural for analgesia
Higher risk of severe complication versus FN- Covers ON well if block is done properly
- Technically challenging as it is a deep block
- May be challenging to position in lateral position for a patient with hip fracture
- Risk of severe complication
19
(intravascular injection or bilateral anaesthesia such as epidural or intrathecal)
FIB
Dalens 1989
20
Thompson 2020
23
Schulte 2020
24
Steenberg 2018
25
Superior analgesia vs 3-in-1 block
Statistically significant decrease in morphine consumption and increase in patients’ satisfaction versus control
Decrease opioid consumption and earlier discharge versus control
Analgesic effect superior to opioid, low pre-operative analgesia consumption, reduce time to perform spinal anaesthesia- Covers LCNT reducing posterolateral surgical incision pain
- Catheter insertion site near surgical field resulting in contamination or premature removal
ESPB
Ahiskalioglu 2020
28
Mujahid 2021
29
ESP as sole anaesthetic technique for hip surgeries
Provides adequate analgesia for post hip surgery for 24 h without strong opioids- Possibility of provide anaesthesia for hip surgery
- Requires ultrasound as this is a much deeper block
- Possible risk of injuring structure near to spine such as nerve roots and deeper vessels
PENG
Girón-Arango 2018
30
Sahoo 2021
31
Aliste 2021
32
Lin 2021
33
Average reduction of pain score of 3.4 and median drop of 7 points in pain score following the PENG block versus control
Overall reduction in pain score at 6H, 12H & 24H post-operatively
Lower incidence of motor block but no significant difference in post-operative pain scores, cumulative opioid consumption at 24H and 48H, opioid related side effects, ability to perform physiotherapy or length of stay versus FIB
Less pain and better quadriceps muscle strength preservation versus FNB- Similar analgesia to FIB based on one RCT
32
while reducing incidence of quadriceps motor blockade
- Possibly more reliable since it does not depend on LA spreading over a large area- Require ultrasound as there has been no landmark technique described
- May not be as helpful for extra-articular fractures (i.e. intertrochanteric/ subtrochanteric fractures) though more studies are needed to elucidate this spread of LA over surgical site