
Abstract
Introduction
The incidence of proximal femoral fractures has increased with a greater number of patients who are in the elderly population with osteoporosis. Reverse oblique fractures is a unique fracture pattern that is anatomically and mechanically different from the other trochanteric fractures. The fracture line extends from the proximal medial cortex out through the distal lateral cortex. Thus it is more difficult to treat due to medial displacement of femoral shaft. Reverse oblique fractures have two main types of implants available, which are the dynamic hip screw (DHS) and intramedullary implants. However, there is a high rate of incidence of fixation failures when the dynamic hip screw are used, due to the anatomical structure of the reverse oblique fracture which would result in a varus deformity of the fracture during the recovery phase.
Methods
The surgery involves a stainless-steel intramedullary nail, 2.7 mm mini plate with 3 screws.
Discussion
Dynamic Hip Screw can be used to fix reverse oblique fractures, however, it results in extensive medialization of the shaft and poor fracture healing, resulting in higher risk of implant failure. Conversely, intramedullary femoral nail can also result in lateral migration of fracture fragments, hindering effective reduction. Thus in this study, 2.7 mm mini plates and 3 screws are used to counter the virus movement of the muscles to achieve good reduction. By using 3 screws, it provides better rotational control of the proximal fracture fragment and decrease the cut out of the femoral head by preventing toggling of the proximal fragment.
Keywords
Introduction
The incidence of proximal femoral fractures has increased with a greater number of patients who are in the elderly population with osteoporosis. 1 Intertrochanteric fractures are common extracapsular fractures of the proximal femur at the level of the greater trochanter and lesser trochanter. 2 Intertrochanteric fractures are most commonly seen following low-energy trauma in the elderly population. 3
Fractures in the trochanteric area are classified according to the Orthopaedic Trauma Association Classification system as AO/OTA 31-A, which classifies these fractures as extracapsular fractures of the hip. 4 These fractures are subdivided into groups A1, A2 and A3. A1 fractures are simple two-part fractures. A2 fractures involve multiple fragments. A3 (3.1 to 3.3) fractures include reverse oblique and transverse fracture patterns. 5
The reverse oblique fracture of the proximal femur is a unique fracture pattern that is anatomically and mechanically different from the other intertrochanteric fractures. 6 The fracture line extends from the proximal medial cortex out through the distal lateral cortex. It is more difficult to treat due to the medial displacement of the femoral shaft from the movements of the adductors, causing a shearing force when weight is loaded. 7
Reverse oblique fractures have two main types of implants available, which are the dynamic hip screw (DHS) and intramedullary implants. 8
During recovery, there is a high rate of fixation failure when DHS is used due to the anatomical structure of the reverse oblique fracture, which results in varus deformity during healing. 9
Hence, most surgeons advocate intramedullary nailing for reverse oblique fractures. 10 However, the challenges of intramedullary nailing include difficulty in obtaining good reduction—especially when using a traction table—and risk of varus collapse after fixation. 11
Additionally, the clinical reports regarding intramedullary implants for reverse oblique fractures are few in number. 12 The purpose of this case series is to present results of intramedullary nailing with a mini-plate performed for reverse oblique intertrochanteric fracture, including evaluation of postoperative quality, functional status, and complications.
Materials and methods
From 2021 to 2022, three patients with AO/OTA 31-A3 fractures were treated with intramedullary femoral nail and 2.7 mm mini-plate fixation with three screws at Singapore General Hospital (SGH).
Patients with reverse oblique fractures were selected for the surgical procedure and appropriately consented. The surgery involved an intramedullary nail, 2.7 mm plate and screws, traction table, and isolation drape. Gentle traction was applied to reduce the fracture in abduction and an open incision was created at the fracture site. The fracture was reduced under direct vision. The 2.7 mm plate was applied and fixed at the anterolateral surface of the proximal femur to resist flexion and abduction forces of iliopsoas and gluteus medius. 13 The plate provided initial reduction stability; once the nail was inserted, the plate acted as augmentation to prevent varus collapse. The hip was adducted to ease Kirschner-wire insertion for the entry point. Short proximal femoral nailing was performed.
Weight-bearing status post-surgery was decided by each patient’s bone quality. All were referred to physiotherapy for rehabilitation and followed for 1 year with serial radiographs. Quality of life and complications were documented.
Case 1
88 year old Chinese female, pre-morbidly activities of daily living (ADL) and instrumental activities of daily living (IADL) independent. She was also community ambulant without walking aid, ASA Class II. She does not have any past acute myocardial infarction (AMI), no past cerebrovascular incident (CVI). However, she has a history of severe osteoporosis.
She had sustained a witness fall while getting off a weighing machine and had a direct impact on the left hip, resulting in a reverse oblique trochanteric fracture of the left femur (Figure 1(a)) She was treated with a intramedullary femoral nail and a 2.7 mm mini plate. (Figures 1(b) and (c)). A reverse oblique trochanteric fracture of the left femur (Figure 1(a)) Immediate post-surgical fixation (Figure 1(b) and (c)) 3 months post operation, callous formation and fracture is in good position (Figure 1(d)) 9 months post operation (Figure 1(e)).
The operation duration was 2 h and 15 min with blood loss of 250 ml.
Bony union was achieved in 3 months and there was no displacement (Figure 1(d)). With the aid of a physiotherapist, she began weight bearing at 4 weeks post operatively. She presented with good range of motion without pain. The patient was also given advice to start on anti-osteoporotic medication in view of her severe osteoporosis.
1 year post operative, the patient progressed to the use of a walking stick with full weight bearing. Radiograph showed good peri-prosthetic alignment and hard callous formation. (Figure 1(e)).
Case 2
92 year old Chinese female, pre-morbidly ADL and IADL independent, community ambulant without walking aid, ASA Class III. She had a past medical history of a transient ischemic attack, left parietal meningioma and an ischemic heart disease status post percutaneous coronary intervention.
She suffered from a non-vertiginous giddiness, resulting in a fall and a direct impact to the left hip. (Figure 2(a)). Reverse oblique intertrochanteric fracture of the left femur (Figure 2(a)) Immediate post fixation and reduction radiographs (Figure 2(b) and (c)) 3 months follow up, intramedullary implant was stable, has good alignment and no signs of periprosthetic fracture. (Figure 2(d)) 6 months follow up, implants are stable and in alignment. Interval healing is also noted in the left proximal femur fracture site. Bones are also noted to be severely osteoporotic. (Figure 2(e)).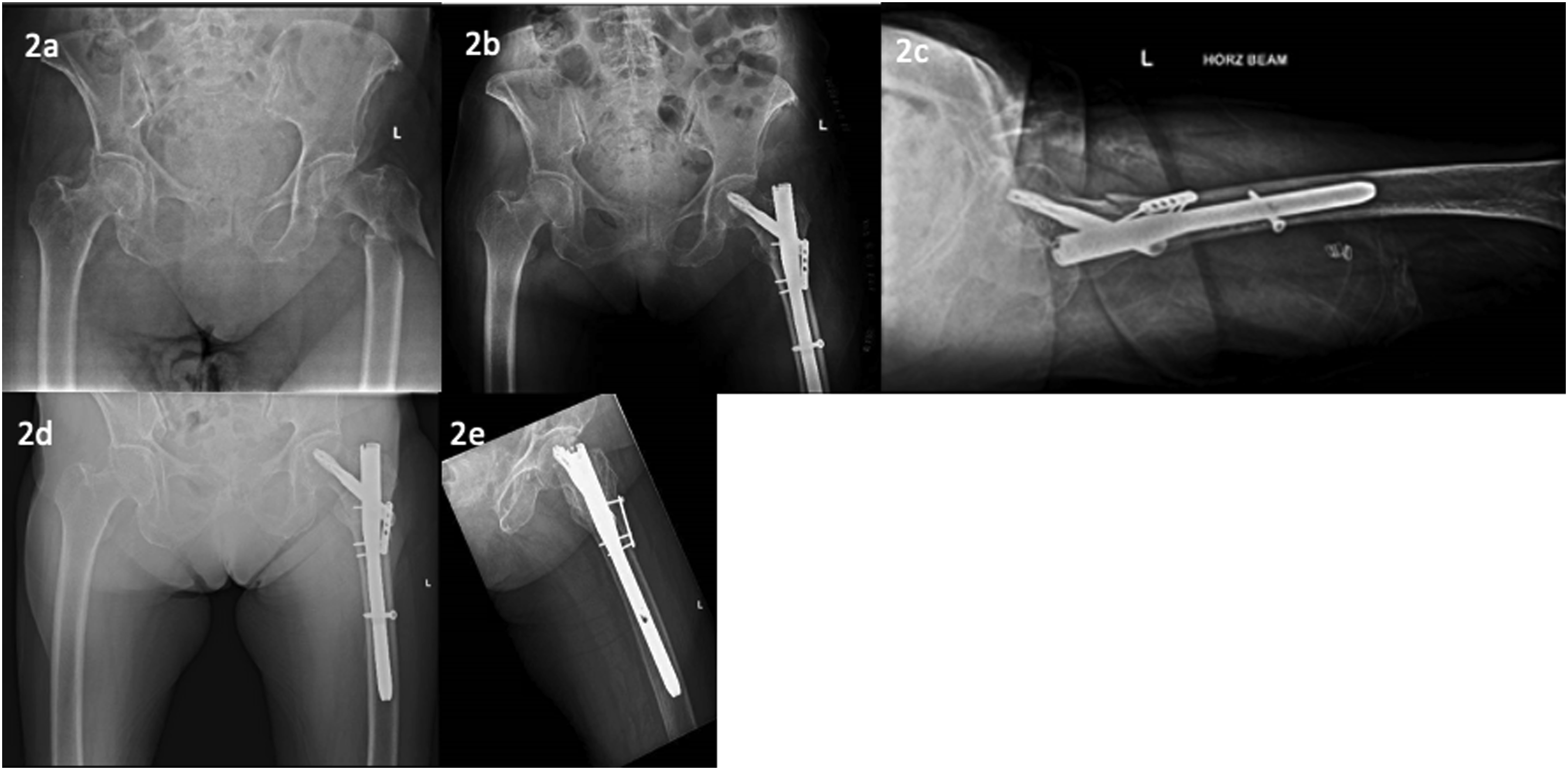
She was unable to ambulate after and required assistance to the emergency department. Patient subsequently underwent surgical fixation of left intertrochanteric oblique fracture with intramedullary nailing and plating. The operation duration was 1 h 45 min with blood loss of 200 ml.
Post-operative x-rays show satisfactory reduction and alignment. (Figures 2(b) and (c)).
She was able to ambulate with a walking frame at 3 months follow up. (Figure 2(d)).
At the 6 months follow up, the patient was ambulating without any walking aids and radiographs showed that the fracture had been healing at a satisfactory progress. (Figure 2(e)).
During the 1 year post operative follow up, she did not have any new symptoms and was ambulating well. No radiographs were repeated as the previous radiograph at the 6 months mark showed that the fracture had healed.
Case 3
64 year old Chinese female, pre-morbidly ADL independent, community ambulant without walking aid, ASA class 3. She has a past medical history of adult-onset polycystic kidney disease, hypertension and chronic venous insufficiency.
She sustained a mechanical fall and was unable to get up and ambulate thereafter. She presented to the emergency department with a shortened and externally rotated left lower limb. There was also tenderness over the left hip. Radiographs shows that there is a reverse oblique intertrochanteric fracture with external rotation of the femur. (Figure 3(a)). Reverse oblique intertrochanteric fracture of the left femur. Left femur is noted to be shortened and externally rotated (Figure 3(a)) Immediate post-op fixation (Figure 3(b) and (c)) 3 months follow up, radiographs shows breakage of the distal screw of the mini plate. Alignment of the implant is otherwise non-displaced. Soft callous formation can be seen. (Figure 3(d)) 6 months follow up, alignment of the implant is stable, good healing progress of the fracture (Figure 3(e)).
2 days post fall, she was treated with the same technique. (Figures 3(b) and (c)).
The operation time was 1 h 50 min with blood loss 400 ml.
The operative fixation was satisfactory and the patient was advised to partial weight bear with the aid of in-patient physiotherapist.
The patient was subsequent discharged 2 days later with 50% partial weight bear advice.
During the 3 months follow up, she ambulated with a walking frame. There was good range of motion without pain. The repeat radiograph showed that the distal screw of mini plate had broken, although no implant/fracture malalignment was detected. There was also presence of soft callous formation indicative of good healing process. (Figure 3(d)).
At 6 months follow-up, she had good hip range of motion without pain and was able to ambulate with a quad stick. X-rays showed that the fracture had completely healed. (Figure 3(e)). The patient also feedbacked that she was happy with the progress.
During the 1 year post operative follow up, she did not have any new symptoms and was ambulating well. No radiographs were repeated either as the previous radiograph at the 6 months mark showed that the fracture had healed.
Discussion
Fractures in the trochanteric area are classified as AO/OTA 31-A. 4 Although AO/OTA 31-A3 fractures comprise only 5.3–23.5 % of all trochanteric fractures, they show higher implant-failure rates than A1 or A2 types. 14
Reverse oblique intertrochanteric fractures are unstable due to their unique anatomical and mechanical structure: the main fracture line extends from proximal-medial to distal-lateral, creating a shearing vector that displaces the shaft medially.6,7
According to the Norwegian Hip Fracture Register, failure rates are 10.3 % for DHS versus 5.6 % for intramedullary nailing. 19
When using DHS, distraction and medialization of the shaft can occur, leading to varus malalignment and telescoping.10,19
Conversely, intramedullary nailing can cause migration of fragments, hindering reduction (Figure 4(a)).
11
Cerclage wires may assist reduction but risk periosteal strangulation and delayed healing.15,18 Intraoperative images: Use of intramedullary femoral nail alone causing lateral migration of the fracture fragment. (Figure 4(a)) Intraoperative image: Implementation of mini plates countering the varus movement of muscles. (Figure 4(b)).
In this study, a 2.7 mm mini-plate was used to maintain reduction prior to nail insertion. The anterolateral mini-plate resists abductor forces, facilitates adduction for entry point exposure, and functions as a buttress to prevent varus collapse.16,17 The trapezoidal proximal femur allows screw placement without interfering with the nail trajectory. Using three screws provides rotational control and minimizes femoral-head cutout. 9
Perfect reduction is difficult with traction table alone. The plate provides direct control of the proximal fragment, aligning the lateral cortex before nail insertion. 12 After intramedullary fixation, load is transmitted mainly through the nail, while the plate resists shear and aids in osteoporotic bone stabilization. 17
The average operation time was 1 h 56 min and mean blood loss 283 mL. All three patients demonstrated radiological union by 6 months, consistent with other PFN outcomes.3,5,13,20
Reverse oblique fractures are an important cause of morbidity and mortality in elderly patients; early surgical stabilization reduces complications and mortality. 21
In conclusion, AO/OTA 31-A3 fractures are uncommon but prone to fixation failure. The combined intramedullary nail with mini-plate method provided good outcomes at 9 months follow-up.
However, we do know that the limitations of our study is that this is a case series, and it also lacks a control group. A larger study is also required to determine the quality of reduction and fixation using intramedullary nailing and mini plates as it would be difficult to extrapolate that the method will work for broader populations.
We acknowledge that there are different proximal femoral nails used between the 3 patients. However, most studies do not conclude if either of the implant is more superior than the others especially in the event that cut out rates are generally low in intertrochanteric fractures treated with intramedullary nailing.
Lastly, we also acknowledge that the patient can be followed up for a longer period of time to better understand the prognosis of the method.
Footnotes
Author contributions
Yang Kai Chan, Yew Lok Woo
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing is not applicable to this article as no datasets were generated or analysed during the current study.