
Abstract
Introduction
Human breast milk remains an important source of protection against infection, inflammation, allergy and long-term metabolic disorders for the breastfed offspring. In addition, breastfeeding has numerous advantages for the mother’s health as well as the establishment of the mother-child bond. There is also mounting evidence that breast milk confers immune protection during periods of maternal infection, which makes it critical that healthcare providers continue to support mothers who wish to breastfeed despite illness, where appropriate. This is particularly relevant given the current pandemic status of Coronavirus Disease 2019 (COVID-19), and the need to provide reliable answers to common questions which the medical community might face regarding breastfeeding during common illnesses.
The dilemma faced by both medical health professionals and mothers during infection is the need to balance the risk of continuing versus temporarily or permanently ceasing to breastfeed. Continuing breastfeeding entails concerns of possible infectivity through breast milk and transmission via direct or indirect contact between the mother and child during the process of breastfeeding. On the other hand, discontinuing breastfeeding may result in a loss of opportunistic immune and gut protection, and even a short-term disruption of breastfeeding may result in an unintended long-term reduction in milk supply which harms the breastfeeding relationship. Every mother wants to provide the best for her child, and many would thus worry if they could personally be responsible for infecting their babies through breastfeeding, whilst dealing with the guilt of possibly withholding something that can protect their vulnerable newborn. With increasing litigation worldwide, health professionals who are wary of the medicolegal implications of inappropriate advice would tend to err on the side of caution and recommend forgoing breastfeeding, especially in the presence of uncertainty.
Particularly during times of rapidly emerging evidence on novel pathogens, it would be prudent to remember that guidance may have to be fluid as more knowledge is uncovered regarding the nature and transmissibility of the infectious agents. This is especially clearly illustrated in the case of human immunodeficiency virus (HIV). Mothers were initially advised to abstain from breastfeeding if they were able to afford, prepare, and store formula milk safely. However, particularly in developing countries such as Africa, infant mortality actually increased when breastfeeding was withheld, due to a lack of access to clean water and sanitation for hygienic preparation of breast milk substitutes. In a World Health Organization (WHO) bulletin entitled “Breast is always best, even for HIV-positive mothers”, it was recommended that HIV-positive mothers on anti-retroviral therapy should breastfeed to maximize their babies’ health prospects. In addition, exclusive breastfeeding in the first six months of an infant’s life is associated with a three- to fourfold decreased risk of HIV transmission compared to mixed feeding. 1 Thus, the aim of our article is to review existing literature regarding breastfeeding during acute infectious and non-infectious illnesses, and to provide feasible evidence-based suggestions which can be implemented by medical practitioners during counseling of breastfeeding mothers.
Immune protection and breast milk
Breast milk contains a host of immune-active compounds, including immune cells, antibodies, growth factors, and cytokines, which support the newborn’s immature immune system. 2 Immunoglobulin A (IgA) is the main antibody in breast milk. Breast milk protects the offspring from infections via the secretory IgA antibodies, but also possibly via other factors such as the bactericidal lactoferrin. 3 During lactation, there is evidence of protection to the offspring against respiratory tract infections, urinary tract infections, diarrhea, otitis media, neonatal septicaemia and necrotising enterocolitis.
If a mother mounts an immune response to a particular pathogen following symptomatic or asymptomatic infection, it is possible that some immunity can be transferred to her offspring in the same manner via antibodies in her breast milk. Increasing evidence demonstrates that within the entero-mammary immune system, transport of plasma cells occurs continuously between gut-associated lymphatic tissue into the systemic circulation, and then back to the gut to provide local secretory immunity, as well as to distant sites to provide the same specific immunity. It is thus postulated that passive immunity from breast milk can protect infants against a number of infectious diseases and toxins to which they are particularly vulnerable. 4 Passive transplacental transfer of antibodies is the basis for antenatal influenza and whooping cough vaccinations. Passive immunity to influenza has also been documented in infants up to six months of age following maternal influenza vaccination during pregnancy. 5 The probable entero-mammary pathway is also cited as the reason why breastfeeding mothers should continue to feed their offspring with breast milk even during most maternal infections, wherever possible.
Mother to child transmission
Breastfeeding is safe and recommended in most acute infections, and there is no increased risk of mother to child transmission in the majority of cases. In previous published guidance by the World Health Organization (WHO), the only maternal condition which might justify permanent avoidance of breastfeeding is human immunodeficiency virus (HIV) - although there is now also increasing evidence of substantially reduced postnatal HIV transmission risk under antiretroviral therapy (ART) cover. 6 For most other maternal health conditions and infections, breastfeeding can continue, although health problems may be of concern. 7 It may be of note that the quality of evidence for much breastfeeding research is limited, as the established benefits of breastfeeding make it unethical to conduct randomized controlled trials on the subject.
For the purpose of this paper, direct breastfeeding refers to latching the infant directly at the mother’s breast. Expressing breast milk via hand expression or specialized pumping equipment also constitutes a form of indirect breastfeeding. Exclusive breastfeeding refers to the infant receiving only breast milk (with the exception of medications); mixed feeding involves the infant receiving other milks and/or foods in addition to breast milk.
Specific infections
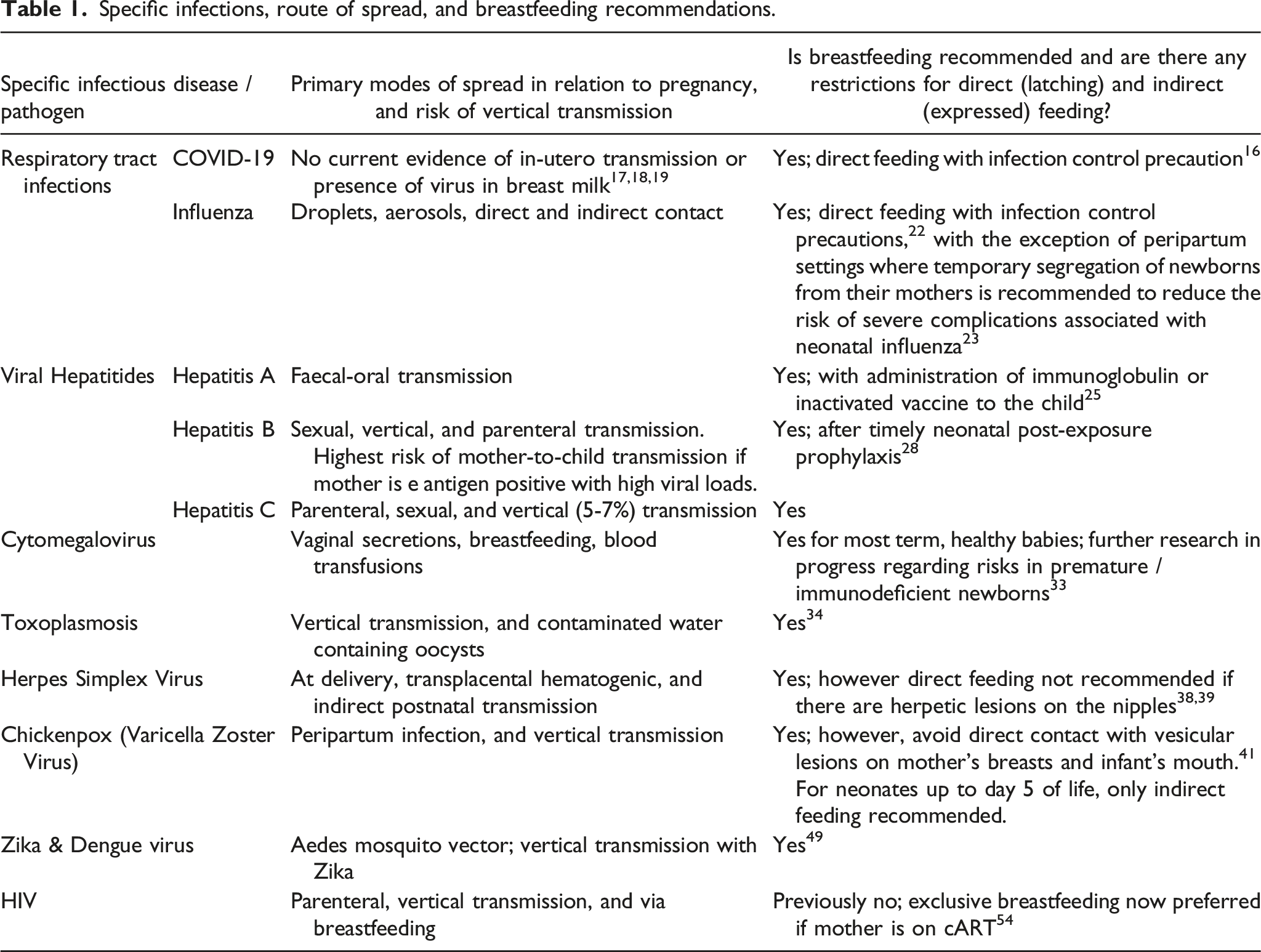
Specific infections, route of spread, and breastfeeding recommendations.
Breastfeeding may provide opportunistic immune defense to the offspring during viral pandemics. 8 We explore a few pertinent lower and upper respiratory tract infections below:
COVID-19
In the first published case series of 9 pregnant women with COVID-19 infection, samples of amniotic fluid, cord blood, neonatal throat swabs and breast milk were tested for the presence of SARS-CoV-2. All samples including breast milk tested negative for the virus. All the patients in this study were delivered by Caesarean section, and the findings suggested that no intrauterine fetal infections occurred as a result of COVID-19 infection during a late stage of pregnancy. The second retrospective series on pregnancies complicated by COVID-19 reported nine obstetric patients in Hubei, including two patients who underwent spontaneous vaginal delivery. Throat swabs from the ten neonates born from this population were all negative for SARS-CoV-2, supporting that intra-uterine transmission of SARS-CoV-2 to the fetus is unlikely. 9
Wang et al. 10 reported a case of a neonate diagnosed with COVID-19 infection 36 hours after birth. The mother was admitted with presumed COVID-19 infection based on computerized tomography (CT) and clinical findings and underwent a caesarean delivery at 40 weeks. Her pharyngeal swab subsequently returned positive for SARS-CoV-2, and thereafter her baby’s pharyngeal swab was collected 36 hours after birth, and returned as positive. Umbilical cord blood and placental swabs were negative. Expert consensus remains that mother-to-child transmission is unlikely, however cannot completely be excluded. 11
Given that no pathogen has been isolated in maternal milk in the studies carried out to date, transmission via breastfeeding is currently regarded as improbable. 12 However, the primary concern is that an infected mother might transmit the virus via respiratory droplets during the period of breastfeeding. In the Chinese hospitals, all babies were isolated from the mothers and none were infected. There are varying policies internationally regarding postnatal physical isolation and depend in part on prevailing healthcare resources. 13 It is prudent to remember that whilst most reproductive aged women who contract COVID-19 tend to have mild or asymptomatic infections, there have been reports of severe maternal morbidity and perinatal death associated with COVID-19 infection during pregnancy. In a recent review of 108 pregnant women with confirmed COVID-19 infection, there was a 3% rate of maternal intensive care unit admission, with one neonatal and one intrauterine fetal death reported. 14 This underscores the importance of careful monitoring of pregnancies with COVID-19 infection.
Recent clinical guidelines from the Royal College of Obstetricians & Gynaecologists (RCOG) 15 and American College of Obstetricians & Gynecologists (ACOG) 16 advise that the benefits of breastfeeding outweigh potential risks of the virus transmission through breast milk. Breastfeeding mothers who have confirmed or suspected COVID-19 infection can choose to breastfeed directly or express their milk and engage a healthy assistant to feed this to their baby. Breast pump equipment should be carefully sanitized before and after usage. Additional infection control precautions to be taken by the mothers include washing hands thoroughly before handling their babies and wearing face masks during direct latching. If the mother is not well enough to breastfeed or express or choose to use breast milk substitute, her choice should also be supported.
International organisations such as World Health Organisation (WHO), 17 the Academy of Breastfeeding Medicine 18 and the Centre for Disease Control and Prevent (CDC) 19 recommend breastfeeding women who have received COVID-19 vaccine to continue breastfeeding post vaccination because the mRNA vaccine is unlikely to cause harm. Recent reports have shown that breastfeeding people who have received mRNA COVID-19 vaccines have antibodies in their breastmilk, which could protect their babies. These protective antibodies can be detected in breast milk as early as five to seven days after vaccination. 20
Influenza
Human influenza is transmitted via droplets, aerosols and direct or indirect contact. 21 In a peripartum setting, temporary segregation of newborns from their mothers is recommended to reduce the risk of severe complications associated with neonatal influenza. However, breastfeeding mothers should continue to express their milk and their babies should continue to be fed this via a healthy caregiver. This will benefit the neonates due to the production of specific IgA antibodies, and also helps to support the breastfeeding mothers’ milk supply. 22 Mothers with influenza should take similar infection control measures to those proposed for suspected or confirmed COVID-19 infections. This includes washing hands prior to touching their babies, wearing face masks during feeding at the breasts, and maintaining high sanitary standards when handling expressed milk and pump equipment. Antenatal vaccination against influenza effectively reduces the rates and severity of disease in vaccinated mothers as well as their children and hence should be offered routinely. Neonates and infants may also be protected against influenza directly by antibodies of maternal origin that cross the placenta or are transferred via breast milk, with the duration of passively acquired antibodies lasting up to six months. 23
Hepatitis A, B, and C
Breastfeeding does not increase the transmission of hepatitis A, B or C. While mother-to-child transmission of these viruses has been known to occur at any time during pregnancy, the majority of risk remains during labour and delivery. Appropriate treatment of all mothers and neonates can further help to reduce this risk.
Hepatitis A
Hepatitis A is transmitted via the faecal-oral route. Infection during the second and third trimesters of pregnancy is associated with preterm labour and other complications. 24 Although viral RNA has been detected in breast milk of mothers with acute hepatitis A virus (HAV) infection, there is no evidence that breastfeeding transmits HAV to suckling infants. Therefore, breastfeeding should be encouraged, and the child should be protected through administration of immunoglobulin or the inactivated vaccine. 25
Hepatitis B
Vertical transmission of hepatitis B occurs in 90% of pregnancies where the mother is hepatitis E antigen positive, versus 10% of pregnancies with e antigen being negative. Tenofovir monotherapy can be considered in the third trimester when the viral load (HBV DNA) exceeds 107 IU/mL. In addition, hepatitis B specific immunoglobulin can be given intramuscularly to infants of highly infectious mothers, and this reduces vertical transmission by 90%. 26 Compared with the administration of hepatitis B vaccine alone, vaccine plus hepatitis B immunoglobulin reduces hepatitis B occurrence in newborn infants of seropositive mothers. 27 Although hepatitis B surface antigen (HBsAg) has been detected in breast milk, it is considered safe for the mother to breastfeed as long as the immunoglobulin and vaccine are administered before the first feed. Even in the presence of nipple injuries which may expose the offspring to small amounts of maternal blood, breastfeeding is not considered to increase the transmission of hepatitis B. 28
Hepatitis C
There is no firm evidence that breastfeeding increases the risk of hepatitis C transmission to the newborn. While there is a small potential risk of vertical spread (around 5%) during pregnancy, no interventions have been shown to reduce this risk, including Caesarean delivery. In addition, Ribavirin therapy is teratogenic and should be avoided during pregnancy. Co-infection with HIV increases the risk of mother-to-child transmission to at least 7%. 29 This emphasizes the importance of routine serological screening during pregnancy. Standard precautions, which encompass universal precautions and body substance isolation, should be taken at delivery and other invasive procedures to prevent transmission of bloodborne viruses such as hepatitis B and C in healthcare settings. 30
Cytomegalovirus
Cytomegalovirus can be contracted postnatally via vaginal secretions, breastfeeding, or blood transfusions, with up to 93% of CMV-seropositive mothers shedding CMV into their breast milk. 31 However, in a study of 32 patients with severe combined immunodeficiency (SCID), it was found that only 6% contracted CMV, with breast milk being the only identifiable source. A subsequent study also found that there was no significant difference in CMV infection between breast-fed and non-breast-fed infants. 32 It is generally accepted that the benefits of breastfeeding outweigh the risks of CMV transmission in most term, healthy, non-immunodeficient infants. 33 Research is being directed towards determining the impact of breastfeeding on CMV infections amongst premature and immunodeficient newborns, and some studies have shown success in various methods such as freeze-thawing of breast milk in reducing the viral load of CMV.
Toxoplasmosis
Although the presence of Toxoplasma has been found in the milk of several animals, no cases of human transmission via breastfeeding have been confirmed to date. 34 In addition, anti-T gondii antibodies in breast milk may exert protective effects for the infant. Contaminated water containing oocysts is a more likely route of transmitting acute Toxoplasmosis infection amongst breastfeeding mothers and newborns, and measures to improve the sanitation of drinking water remain the focus of public health in many developing countries. 35
Herpes Simplex Virus (HSV)
Neonatal HSV infection can have devastating long-term sequelae, especially with central nervous system involvement. 36 Transmission to newborn can occur via transplacental hematogeneous passage, at delivery (the most frequent route), or during the postnatal period (indirect transmission). 37
Antiviral treatment of pregnant mothers and caesarean section delivery confer the greatest protection against neonatal herpes when maternal HSV infection is confirmed close to term. However, professional consensus is that breastfeeding is not contraindicated in cases of maternal herpes, except if there are herpetic lesions on the nipples. 38 Health institutions should support lactation and a return to breastfeeding during maternal and neonatal infections with HSV. 39
Varicella Zoster Virus (Chicken pox)
Peripartum maternal varicella infection poses the most severe risk of neonatal varicella which can be severe, and separation of the mother and infant is recommended until the viral lesions crust over. Varicella zoster immunoglobulin (VZIG) can be administered to the neonate to further reduce the risk of transmission. There is no clear evidence that the virus is transmitted via breast milk, hence expressed breast milk of infected mothers can continue to be fed to their infants. 40 If the onset of varicella disease occurs more than five days before delivery, maternal antibodies may be transferred via breast milk, and neonatal infection tends to be milder. In this case, direct breastfeeding may proceed after the lesions are covered up, with standard hygiene precautions in place. 41 WHO advises that direct contact between lesions on the mother’s breasts and the infant’s mouth should be avoided until all active lesions have resolved. 42
Herpes zoster, commonly known as shingles, is caused by VZV reactivation. It typically presents as a localized, painful, vesicular rash involving one or adjacent dermatomes, 43 and VZV is spread through direct contact from these rash blisters. If a mother has active shingles infection, she can continue to breastfeed if she does not have skin lesions on her breast. Direct latching on the affected breast is not recommended if there are lesions on or near the areola. 44 In mothers who received varicella vaccination postpartum, no evidence of varicella virus excretion was found in breast milk, suggesting that breastfeeding should not be a contraindication to vaccination of varicella-susceptible women, and vice versa. 45
Zika & Dengue Virus
Zika virus and dengue virus (DENV) are arboviral infections transmitted by the Aedes mosquito, with dengue being endemic in Singapore. 46 Zika infection is associated with neonatal and postnatal microcephaly, as well as other birth defects. A systematic review found no evidence of long-term complications in breastfed infants of mothers with suspected, probable or confirmed Zika infection. One case study in 2013 reported breast milk as a possible route of vertical transmission of DENV. 47 Despite this, CDC continues to encourage mothers to breastfeed even in areas with risk of dengue, 48 as well as in the event of infection or exposure to Zika virus. 49
Human Immunodeficiency Virus
Previously, HIV was the rare exception in which both exclusive and partial breastfeeding was contraindicated. However, as discussed earlier in this paper, the recommendations regarding breastfeeding and HIV have since changed. Although HIV is excreted into the breast milk of infected mothers, and, depending on the viral load, can confer up to an additional 20% risk of mother to child transmission, 50 combined antiretroviral therapy has been shown to reduce the rates of transmission in low resource countries, allowing breastfeeding of up to six months.51,52
Antenatally, patients with HIV should be cared for with a multidisciplinary team approach, involving infectious disease and neonatal specialists. The recommended mode of delivery is influenced by the viral load near term, and the type of treatment which the obstetric patient is on. The actual viral load, trajectory of the viral load, length of time on treatment, adherence issues, obstetric factors, and the woman’s views should also be considered. If Caesarean delivery is indicated to prevent vertical transmission, this should be performed between 38 and 39 weeks’ gestation. 53 Standard precautions should be taken at delivery to prevent the transmission of HIV in healthcare settings. In all instances, infant postexposure prophylaxis up to 4 weeks of life should be implemented in accordance with prevailing guidelines.
The decision to pursue breastfeeding in a HIV positive mother should be individualized based on treatment factors and her unique social circumstances. There is increasing evidence to reassure that breastfeeding in patients treated with antiretroviral therapy is safe. 54 Physicians should assist by providing objective and up to date evidence to support families in the decision-making process and thereafter. If a HIV infected mother chooses to breastfeed, she should be placed on combination antiretroviral therapy (cART) to minimize HIV transmission, and she and her infant should be reviewed regularly in a dedicated clinic to monitor the HIV viral loads. Lactation suppression should be given to mothers who choose to abstain from breastfeeding.
Human T-lymphotrophic virus 1 and 2
HTLV-1 occurs endemically in limited areas worldwide, including Southwest Japan, South America and sub-Saharan Africa.55,56 It results in adult T-cell leukemia/lymphoma (ATL), and is associated with other chronic conditions, such as uveitis, arthritis, Sjogren’s syndrome, infective dermitis and a persistent lymphadenitis in children. HTLV-2 results in at least two forms of chronic ataxia, and is also associated with several other conditions, such as arthritis, glomerulonephritis, myelopathy, T-hairy cell leukemia, and large granulocytic leukemia. 57
Transmission of HTLV-1 and HTLV-2 via breast milk is documented, 58 and complete avoidance of breastfeeding is recommended to prevent mother-to-child transmission from infected mothers. Donated breast milk should be screened for antibodies against HTLV-1 and HTLV-2. In addition, breast milk delivered by milk banks is pasteurized before freezing, which inactivates the pathogens. 59 Informal sharing or donation of un-screened and un-pasteurized breast milk amongst mothers is therefore a potential route of transmitting HTLV to the neonates, and should be cautioned against, especially in developed countries. 60
Gastroenteritis & Diarrhoea
Consistent evidence shows that exclusive breastfeeding protects against gastroenteritis and diarrhoea in the first 4-6months of life. Moreover, infants who are breast fed during diarrhoea experience milder symptoms. 61 This is because breast milk contains immune components which increase an infant’s resistance to infection. Exclusive breastfeeding is more beneficial as it avoids the risk of introducing pathogens to the infant’s gut via supplementary feeding.
Mastitis & Breast Abscess
Mastitis is common in breastfeeding mothers. Acute mastitis can be painful and distressing, leading to disrupted feeding and a reduction in milk supply. The main risk factor for mastitis is milk stasis, which can arise due to factors such as poor latch, nipple injuries and infrequent or missed feedings. It is imperative to actively look for and treat underlying causes of milk stasis to enable effective milk removal and prevent recurrences and further infective complications. Frequent feeding, starting on the affected breast, should be encouraged. A warm pack may be placed on the breast just before feeding to encourage let-down. The infant may be positioned such that her chin or nose points to the area of blockage, as this will help to drain the affected area. Massaging from the blocked area towards the nipple, and hand or pump expression after feeding will also help improve removal of milk. Board certified lactation consultants may be helpful in improving infant latch and screening for infant mouth abnormalities. If a short frenulum is detected, a frenotomy can be performed without anaesthesia, thereafter, facilitating more effective milk removal and reducing repeated nipple trauma. 62
Infective lactational mastitis is a significant cause of peripartum sepsis, resulting in the mother becoming rapidly systemically unwell. A Cochrane review 63 concluded that there is currently insufficient evidence to confirm or refute the effectiveness of antibiotic therapy for the treatment of lactational mastitis, and high-quality research should be conducted on the subject. Amoxicillin/clavulanate (Augmentin) has been suggested as a first line empirical oral antibiotic Staphylococcus aureus (S. aureus) is the most common infecting organism. RCOG recommends Clindamycin in combination with Flucloxacillin (for methicillin-sensitive S. aureus) and Vancomycin (for methicillin-resistant S. aureus). 64 Cold packs can be applied after feeds to reduce pain and edema, and NSAIDS such as ibuprofen can be prescribed.
Breast abscesses are diagnosed on breast ultrasound. Pus from a breast abscess can usually be removed via needle aspiration, with the fluid sent for culture to guide antibiotic therapy. Surgical incision and drainage should be reserved for large or multiple abscesses. Based on a number of studies demonstrating that continued breastfeeding is generally safe, even in the presence of S. aureus, WHO advises mothers to maintain lactation even during mastitis or in the presence of a breast abscess. 65 Regular feeding reduces milk stasis and is helpful for the mother’s recovery and infant’s health. However, patients with breast abscesses should avoid placing the infant’s mouth in contact with purulent drainage or infected tissue, and HIV-positive mother should stop feeding from the affected breast until it has recovered.
Nipple & Mammary Candidiasis
Patients with symptoms such as burning nipple pain and/or deep or shooting breast pain are sometimes diagnosed with “mammary candidiasis”. The evidence for this condition is however conflicting and controversial. Several studies including a recent case-control report 66 have found no significant differences in positive Candida cultures taken from symptomatic and non-symptomatic women, but others have reported a higher chance of isolating Candia in the milk collected from women with breastfeeding-associated pain. 67
The current expert consensus recommendation for women with suspected candidiasis is a trial of antifungal medications. However, a differential diagnosis such as Raynaud’s syndrome should also be excluded. Women with Raynaud’s phenomenon usually complain of persistent severe nipple pain precipitated by cold temperatures and associated with blanching of the nipple followed by cyanosis and/or erythema. The condition can be managed by avoiding cold exposure and vasoconstrictors such as nicotine or nifedipine may also be prescribed. 68
Conclusion
Recognising the value of breastfeeding, there is a strong need to support mothers who wish to breastfeed during periods of acute infections. As always, the decision to breastfeed remains deeply personal, and is dependent on multiple factors including societal norms, the individual’s unique circumstances, and personal desires. 69 It is important for physicians to be sensitive to the thoughts and needs of new mothers, to facilitate breastfeeding wherever possible. By ensuring awareness of updated literature and maintaining non-judgmental attitudes towards counseling, physicians can play an important role in securing positive experiences for breastfeeding mothers and optimizing infant outcomes in this post COVID-19 era.
Footnotes
Author contributions
Samantha Yeo researched literature, conceived the study, and wrote the first draft of the manuscript. Yang Liying researched literature and contributed a significant number of paragraphs to the first draft of the manuscript. Kirsten Ong researched literature and contributed to the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability
Data sharing is not applicable to this article as no datasets were generated or analysed during the current study.