
Abstract
Background
All member states in the Association of Southeast Asian Nations (ASEAN) are ratified signatories of the UN Convention on the Rights of Persons with Disabilities. However, disability and oral health (DOH) can be an elusive ambition for developing nations.
Objectives
This survey aims to conceptualise ‘barriers’, ‘improvements’, ‘challenges in dental practice’, and ‘ways to collaborate’, to inform policy development for DOH within ASEAN.
Methods
The survey employed a novel quasi-qualitative design. It was electronically distributed to dentists with DOH specialty training in ASEAN within the International Association of Disability and Oral Health’s network from September 2018 to June 2020. The ‘barriers’ and ‘improvements’ would be categorised into five dimensions of healthcare - a framework by Levesque and colleagues (2013).
Results
21 valid responses were received from Brunei, Indonesia, Malaysia, Philippines, Singapore and Thailand. From the care provider’s perspective, adequate training (appropriateness) was most prioritised. From the patient’s aspect, low oral health literacy (ability to perceive) was the most significant. ‘Social perception’ was collectively ranked as the key ‘challenge in dental practices’. Suggested ‘ways to collaborate’ could be categorised into five areas: engagement; advocacy; policies; specialty, and; upskilling.
Conclusions
The findings suggest an urgent need to address low oral health prioritisation, a drive to upskill providers, a challenge of ‘social perceptions’, and a consensual appeal for state-level support. A multi-sector collaboration is needed to align current strategies in order to achieve equity for DOH in ASEAN.
Keywords
Introduction

aDentists with dedicated postgraduate training in special needs/care dentistry. These do not include specialists or general dentists without accredited training in DOH care, regardless of experience in disability sectors.
The United Nations Convention on the Rights of Persons with Disabilities (UNCRPD) has been ratified and signed by all member states in Association of SouthEast Asian Nations (ASEAN) - the regional intergovernmental organisation comprising 10 countries.3,4 This is outlined in the ASEAN initiative for disability rights, known now as ASEAN Disability Forum (ADF). One of ADF’s aims is ‘to ensure full accessibility for Persons with Disabilities (PWD) in the built environment by adopting the concept of universal design’. 5
Oral health is an often neglected aspect of disability rehabilitation. 6 The specialty of disability and oral health (DOH) is termed special needs or special care dentistry (SCD). It promotes oral care for people with physical, sensory, intellectual, mental, medical, emotional or social impairments or disabilities or, more often, a combination of these factors that affect accessing oral health. 7 Waldman and Perlman 6 urged for a structured programme for DOH in the USA, because PWD are highly susceptible to dental diseases. 6 This is consequently a combination of poor personal hygiene, physical limitations, medical complexities, parafunctions, and other factors. 6 Thankfully, SCD as a dental specialty is highly progressive, particularly in countries with developed health systems,6–8 where complex treatment modalities such as osseointegrated implants can be now considered for individuals with intellectual disability. 9
In developing nations however, dental caries and periodontal diseases are still considered epidemics. 10 Oral diseases in ASEAN’s impoverished countries further include oral mucosal lesions (due to betel quid and tobacco use), oropharyngeal cancers, HIV/AIDS oral manifestations and oral facial trauma. 10 PWD face poorer dental health outcomes, more oral diseases, and poorer accessibility to oral health services than the average person. 11 A cross-sectional screening programme for 343 adults of mixed disabilities in Singapore revealed that the average PWD of 40 years and above would retain less than 20 teeth. 12
‘Accessibility’ is defined as the opportunity to reach and obtain appropriate health services, which enlists determinants that integrate demand and supply-side factors. 13 Accessibility can be conceptualised into five dimensions, and interacts with five corresponding ‘abilities’ of the service recipients, as outlined by Levesque et al. 13 It can be understood that ‘accessibility’ corresponds to factors of the service provider, while ‘abilities’ relate to patient factors, and these two factors interact to create healthcare utilisation. Without a prior understanding of ‘accessibility’ and ‘abilities’ specific to the beneficiary cohort, health services developed as a result may risk becoming inadequate, inappropriate, or ineffective. 13
Very few known studies, if any, explicitly investigated the determinants of access and utilisation of SCD services in ASEAN. Some key questions arise. Despite the international inclusivity movement and growth of SCD in developed nations, why has DOH in ASEAN not kept up? At the time of writing, Brunei and Malaysia are the only ASEAN countries for which SCD is a recognised dental specialty, with Malaysia being the only country providing postgraduate SCD courses within ASEAN. 14 With the heterogeneous social constructs that persons with disabilities in developing nations face, a complex list of barriers to oral health exist - how do we improve sensemaking for such a phenomenon? 11 This was the starting point for our study. In order to forward ADF’s aim and improve DOH, 5 there is a need to conceptualise understanding of the difficulties and create a framework for development in ASEAN. 5
Objectives
The aims of this study are to 1. Conceptualise barriers (both demand and supply-side factors) that PWD encounter when utilising dental services, and identify their potential solutions; 2. Rank personal challenges faced in the profession of SCD; and 3. Explore potential areas of collaboration to forward DOH in ASEAN.
Methods
Study design
The study design utilised concepts of coding themes and analysis from the grounded theory method.15,16 This method focuses on social processes and in this context, how their interaction creates accessibility. Here, we utilised short open-ended responses and ranking in a survey to focus on barriers and solutions, instead of the classical interview.
16
This allowed respondents to consolidate and prioritise their own themes and concepts, as opposed to the researcher’s interpretations, which may introduce biases. This also avoided excessive need for open-coding (where bulk data in an interview are broken down into discrete ideas) prior to axial coding (drawing connection between ideas).15,16 An additional modification made was for the inputs to be categorised into the five domains of ‘accessibility’ and ‘abilities’ by Levesque et al.
13
This was necessary to relate our findings in DOH to public health accessibility frameworks. Six questions were constructed according to the four processes:
16
1. The phenomenon to be studied - DOH in ASEAN as a research question is defined in the ‘Introduction’ and ‘Objectives’ section. 2. The conditions and context of the phenomenon - The factors around DOH that result in difficulties are studied through ‘accessibility’ and ‘abilities’ (objective 1), and ‘ranking of importance of personal challenges’ (objective 2). 3. The strategies or actions to manage the phenomenon - The solutions are studied through ‘accessibility’ and ‘abilities’ (objective 1) and ‘ways to collaborate’ (objective 3). 4. The considerations and consequences of strategies or actions related to the phenomenon - These are described in the ‘Discussion’ section.
After the pilot test and pilot data analysis, the survey questions were refined before use (Appendix 1). The rationale and details of each questions are described:
Question 1 and 2 - Country of Residence and Profession
Information on the country of residence and profession provides a background of the perspective.
Question 3 and 4 - National Barriers/Challenges Faced in SCD and Ways to Improve
Question 3 collates short descriptions of national barriers faced in SCD, while question 4 collates ways to improve. Respondents may enter up to five responses for these two questions. The responses for ‘national barriers faced’ in questions 3 will be axial-coded then grouped accordingly into the five core domains of ‘accessibility’ and ‘abilities’ as conceptualised by Levesque et al. 13 The responses for ‘ways to improve and forward SCD’ in question 4 is similarly treated. This reflects the first objective of conceptualising barriers.
Question 5 - Personal Challenges and Difficulties in Service
Question 5 relates to the second objective by investigating the level of importance of various personal difficulties challenges in SCD clinical practices. This is because day-to-day challenges faced in the disability sector may not necessarily reflect policy intentions, thereby this question aims to create a juxtaposition of top-down versus ground-up experiences in the DOH field. For this, five broad categories of challenges were adapted from social and determinants to healthcare utilisation by the main author and an epidemiologist, according to appropriateness for the regional context. 17 These were refined after the pilot test to: Quality/quantity relates to the ability of the healthcare manpower to overcome difficulties in DOH; Access relates to geographical distance and infrastructure to enable travel; Social-economics relates to affordability of service; Social perception relates to whether oral health literacy specific to disability has been reached in order for health-seeking behaviours to commence; Policies/facilities relate to healthcare system’s resources, structuring and organisation such as lack of facilities, logistical limitations, or legal-ethical restrictions.
Question 6 - ways for collaboration within ASEAN
Question 6 reflects the third objective of finding potential areas to forward DOH collaboratively as an entity. Respondents provide up to five open-ended responses for question 6. These are then axial-coded into main themes, or broad areas of ‘ways to collaborate’.
Selection criteria
Inclusion and exclusion criteria of survey respondents. a
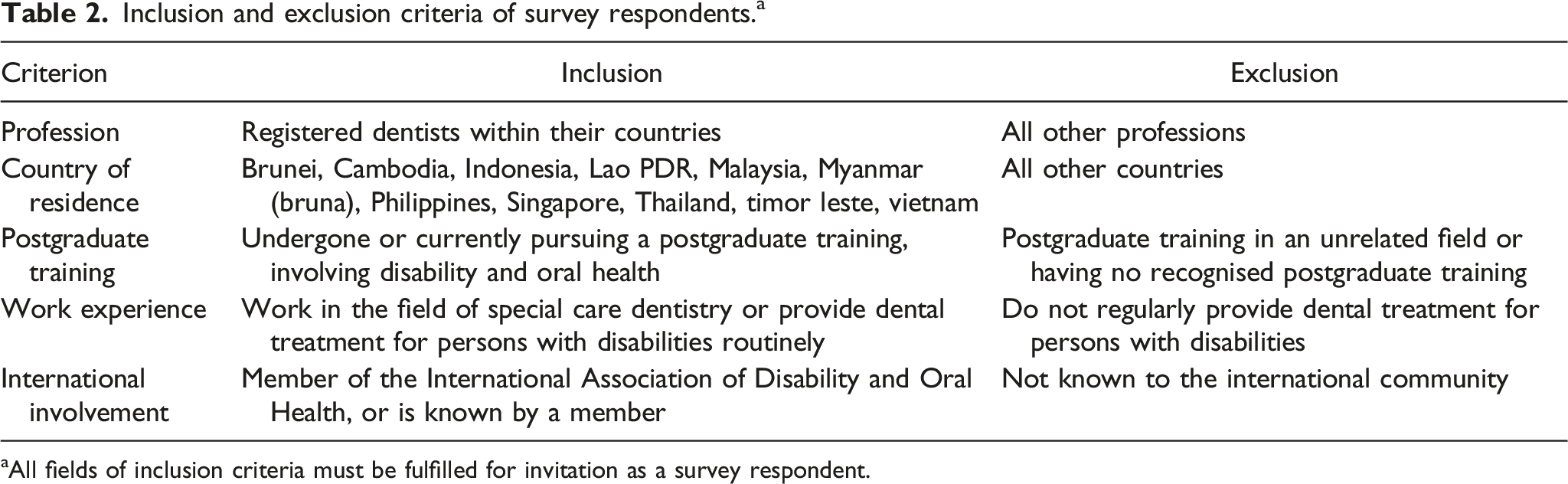
aAll fields of inclusion criteria must be fulfilled for invitation as a survey respondent.
Data collection
Participants were invited for the survey through members of the International Association of Disability and Oral Health (iADH). The survey distribution was done entirely via an online platform (www.surveymonkey.com/r/ZJ3Q783) and started during the 3rd quarter of 2018.
Data analysis
The responses to question 3, 4, and 6 were manually grouped according to their similarities and connectedness. The axial-coding was first done individually by two assessors, the main author and an epidemiologist-cum-data analyst. They were then compared for agreement. Where disputes arose, they were discussed until a consensus was reached. This produced the finalised findings.
For question 5, the ranking was computed by allocating points to each category according to ranks. For example, when a category was ranked first by a respondent, it received 5 points. The category ranked second received 4 points, and so on. The category ranked fifth (or last) received 1 point. By tallying the total points for each category, the final and overall ranking was determined (highest total point ranked overall first). If there was a tie between two categories (same overall points), the higher rank would be given to the category that was more frequently ranked higher.
Ethical approval
This survey was done in accordance with the Declaration of Helsinki. Confidentiality, anonymity, and privacy were exercised inline with the Personal Data Protection Act of Singapore. 18 This constituted an evaluation survey not regulated by the Human Biomedical Research Framework, hence no ethical approval was sought.
Figure 1 provides a flowchart which summarises the study design. Flowchart of study design.
Results
The study was designed to understand the three aims, which required respondents to be widely involved in DOH at the clinical level and beyond, in addition to having a validated training background. Only 26 dentists in ASEAN were known to fulfil the inclusion criteria, and they were all invited to participate. A total of 22 responses were received between 11 September 2018 and 15 June 2020, of which 1 was invalid (registered attempt without any answer). The response rate was 80.8%.
Question 1 and 2 - country of residence and profession
Distribution of respondents from different ASEAN countries.

Despite efforts to encompass perspectives from all ASEAN nations over an extended time of almost 2 years, the authors did not manage to achieve representation from Cambodia, Lao PDR, Myanmar, Timor Leste and Vietnam. Nonetheless, the diversity of viewpoints received has provided valuable preliminary insights. It was agreed amongst the authors that planning of DOH programmes must be tailored to local context and communities. If they were planned generically for the region, the programmes risk losing effectiveness. However, the key purpose of this study is to create a conceptual framework, which would aid in advocacy at an international level.
Question 3 and 4 - national barriers/challenges faced in SCD and ways to improve
There were 101 responses for ‘barriers/challenges’ for DOH services (question 3), which were grouped to either a supply-side (five domains of ‘accessibility’ under service provider factors) or demand-side barrier (five domains of ‘abilities’ under factors pertaining to patients and their ecosystem). For example, the response ‘lack of awareness among the health professionals’ would be grouped under the supply-side barrier of ‘acceptability’ (orange), while ‘lack of awareness among caregivers’ would constitute the demand-side barrier of ‘ability to perceive’ (red). The 97 responses for ‘ways to improve SCD’ (question 4) were also treated similarly for provider-side solutions and patient-side solutions. This is illustrated in Figure 2 with a visual illustration of the conceptual framework. Barriers and improvements for special care dentistry in ASEAN - categorisation into domains of healthcare utilisation.
13

Common barriers/improvements and their distribution according to countries.
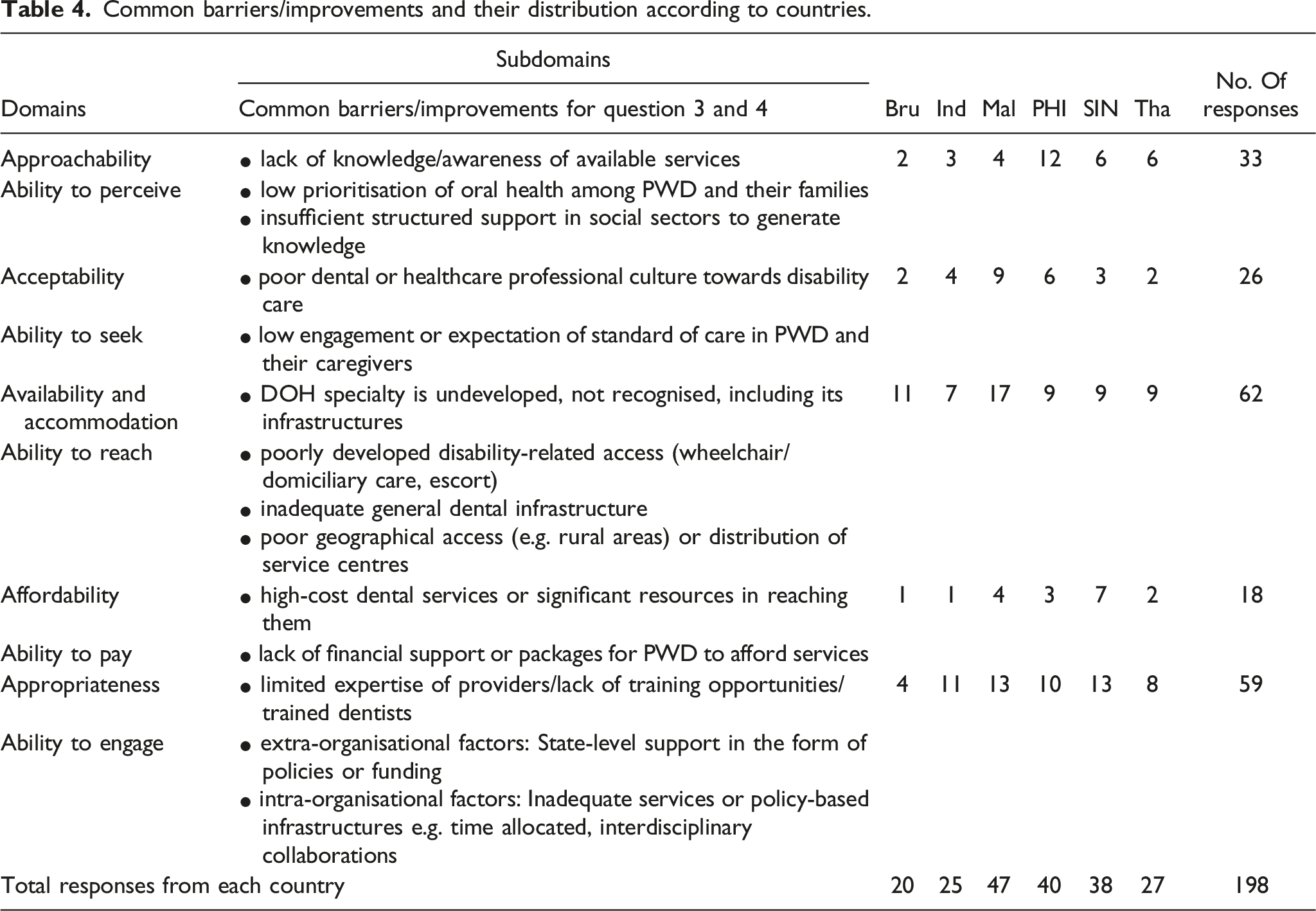
In view of the interconnectedness of barriers (question 3) and solutions (question 4), all 198 responses were pooled to illustrate the 14 subdomains generated, and the distribution of responses per country (Table 4).
Question 5 - personal challenges and difficulties in service
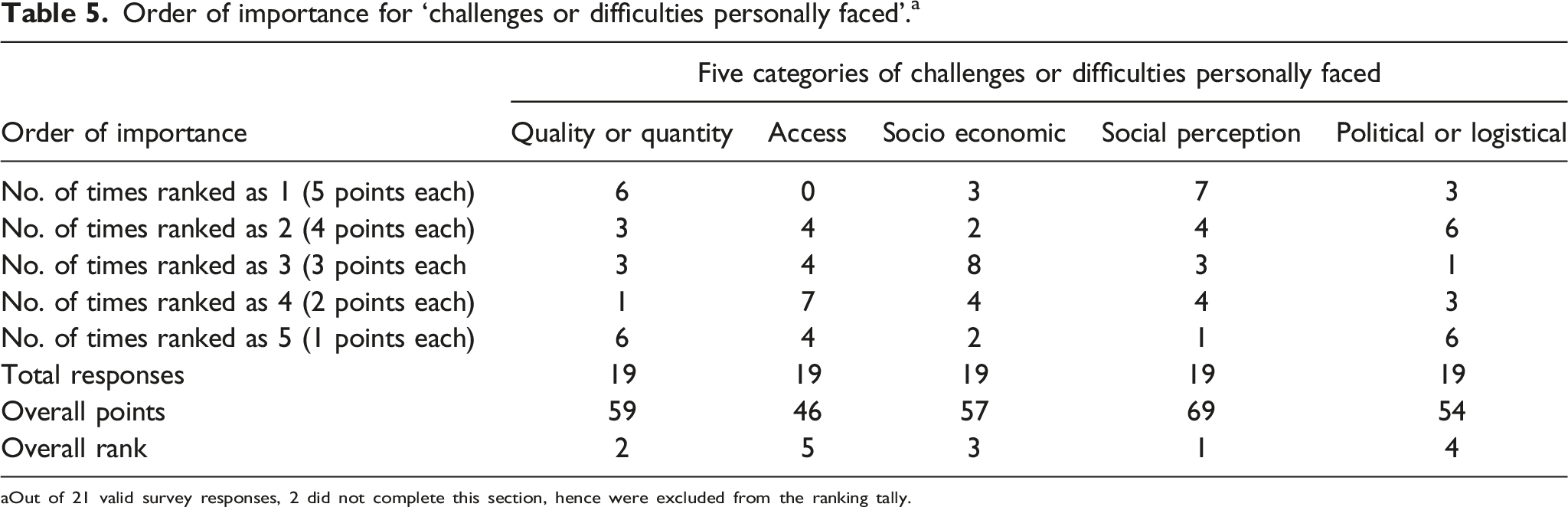
Of the 21 respondents, 2 were invalid (due to incomplete entries) and excluded. Table 5 illustrates the computation of the ranking. The overall rank of ‘challenges or difficulties personally faced’ in order of importance are: 1. Social perceptions: lack of public recognition of importance of oral health; lack of recognition of rights and health needs for people with disabilities 2. Quality/Quantity of manpower: lack of training of dentists/dental staff; too many patients with disabilities 3. Social-economics: financial constraints affecting service provision directly or indirectly 4. Political and adequate facility concerns: limitations in logistics/equipments/services (e.g. GA) affecting delivery of adequate care; restriction in care due to various existent policies/protocol 5. Physical accessibility: difficulty for distant outreach; lack of mobility-enabled dental services Order of importance for ‘challenges or difficulties personally faced’.
a
aOut of 21 valid survey responses, 2 did not complete this section, hence were excluded from the ranking tally.
Question 6 - ways for collaboration within ASEAN
Broad areas that ASEAN can collaborate to further special care dentistry.

Discussion
Understanding barriers and challenges in context
Despite differences in health economics, geography, political situations, and disparate disability aetiologies (Table 1), the ASEAN DOH community face similar barriers (Table 4). In fact, these barriers are often interdependent factors. For example, a PWD’s ‘inability to physically reach a dental service’ could be due to an inability to afford ambulance services, personal mobility challenges, lack of public domiciliary service (inadequate service infrastructure), or simply geographical reasons (living rural or offshore). ‘Long waiting times for PWD in specialist services’, another difficulty raised frequently, may be due to lack of guidance on adequacy of referrals (policy aspects), lack of training avenues for primary dental services (education), lack of training funds (financial), lack of willing dentists (cultural), lack of absolute number of dentists (quantity) or a combination. This makes problem analysis more complex. In view of designing DOH programmes, it is paramount to look deep into the cause across all five domains of ‘accessibility’, evaluate effectiveness, and evolve the approach as the field matures. 19
Understanding solutions to barriers in context
When implementing improvements for disadvantaged cohorts, one has to reflect if the suggested solutions would indeed create the intended social impact (i.e. betterment of oral health in PWD). This is further elaborated in the concept of ‘theory of change’. 19
In the survey, the ‘ability to perceive’ was the most frequently raised patient-related factor affecting health-seeking behaviours (lower red box, Figure 2). In question 5, respondents also ranked ‘social perceptions’ as the most important challenge. The mirroring of findings demonstrated perceptual consistency. These findings resonate with and further endorse the theory of the 5 domains by Levesque et al. 13 - where social perceptions of care recipients must change first (eg. realising that treating dental pain in a PWD is socially acceptable) in order to initiate healthcare utilisation behaviours. Therefore when developing solutions for DOH services, one might expect significant focus on the corresponding supply-side ‘approachability’ to bridge the low health literacy and awareness. However in reality, ‘appropriateness’ and ‘availability and accommodation’ were instead considered the main supply-side factors to tackle (lower purple and green boxes, Figure 2). In fact, under question 6’s ‘ways to collaborate’, there were more mentions of developing training and specialty (green and blue boxes, Table 6) than engaging PWDs (red box, Table 6). This calls to question the above notion of ‘theory of change’ - if the embarked solution could indeed address the defined problem. 19
One hypothesis for this mismatch was that individuals address problems through lenses of their personal competencies, often profession-based. Clinicians could approach DOH from the perspective of clinical services, while public health or epidemiology experts might influence policies. These postulations would require further analysis, such as follow-up interviews with respondents. This emphasises the need for multi-sector insights when developing DOH services. 1
To address the low ‘ability to perceive’, a possible targeted ‘theory of change’ would be through public health promotion. In this context, caregiver oral health training could be implemented by disability support communities, training institutions, or healthcare services. Studies of this approach demonstrated that oral health educational programmes for care service providers and caregivers were effective in improving oral hygiene in the long-term, notably across different cultural landscapes and profiles of PWD.20–23 This ‘theory of change’ has to be person-centred to address the first step - ‘approachability’ (Figure 2), therefore spur subsequent steps of health-seeking behaviours.1,24
Specialisation
Commissioning SCD as a recognised dental specialty is a theme that has repeatedly surfaced in the responses. It was also raised as an area of collaboration for the ASEAN DOH community (Table 6). Comparing the financial structures, such as state-funded or privately-sustained programmes, health literacy levels, 25 and varying stages of health system development, the limited literature imply there could be considerable difficulties when implementing a specialty such as SCD in the public health system.14,16,25–27
The extent to which specialty recognition can efficiently improve the oral health status across cohorts of PWD is often debated. With further ‘specialisation’, out-of-pocket expenses for patients may be raised, particularly in privately-funded dental systems encouraging inter-provider competition. 28 In addition to higher indirect costs of dental treatment, 1 an ASEAN study identified a lower “willingness-to-pay” for dental services particularly for the cohorts with lower oral health-related quality of life. 29 Another article even projected that the cost of treating dental caries would in fact exceed the total health care budget for children in developing countries. 30
Historically, healthcare specialisation (and sub-specialisation) has been known to encourage sustainability, quality, scholarship, and progress, 31 as demonstrated from established SCD services. 8 Therefore when developing SCD as a specialty, themes such as end-user experience, cost, equity, utilisation trends and bottle-neck waiting times, has to be considered.1,31
Limitations
There are some limitations to this study. Firstly, the sample was small because of the small population of DOH-trained dentists in ASEAN.
Secondly, this survey predominantly studied dentists’ perceptions. A patient-centred (end-user) survey might yield different results. However, such a survey would be practically difficult considering the large-scale international effort to encompass a wide range of disabilities across representative cohorts. Nonetheless, since this survey’s respondents routinely engage face-to-face with PWD, their families, and patient advocacy groups, it can be considered that the SCD dentists are at least partially representative of their communities.
In the methods used, categorisation, or sometimes understood as stereotyping, causes generalisation, and attrition of data granularity. However, categorisation could facilitate conceptual development and initial understanding of this complex and heterogeneous field. 32 For policy makers or funders who are seldom directly involved in disability work, our specific design enables sensemaking for strategic planning and decision making.
Future directions
The enigma between perceived barriers (low oral health literacy) and solutions (further training and specialisation) evokes the urgency to articulate a ‘theory of change’ prior to designing policies or oral health programmes. Particularly for developing countries where resources are constrained, there is an impetus to channel funds to effective and appropriate programmes in order to unlock public health bottlenecks.
This then raises the next question of being comprehensive in our approach to the problem. Firstly, both research and dental programmes should be designed by a multidisciplinary team across all socio-economic strata. Secondly, there is also a need for countries to investigate their unique challenges through a range of research methods, such as utilisation surveys, patient interviews, observations, stakeholder’s focused groups etc. Utilising a single method like large-scale population surveys would yield general oral health trends. 33 However due to difficulty in sampling the most socially compromised cohort, these findings may have attenuated effectiveness for PWDs. Further qualitative studies would be required to iterate the complex social processes that influence DOH.
Overall, the five ‘broad areas of collaboration within ASEAN’ (Table 6) are a comprehensive framework in tackling the problem of DOH, and could be applied as ‘five strategic directions’ should a coalition in ASEAN be formed.
Conclusion
This research studied an extremely niche group of disability healthcare providers in ASEAN, many of whom influence public policies, engage in academia, and routinely practise SCD dental services. Despite the conflux of political, geographical, and cultural backgrounds, the findings suggested these key points: 1. The low prioritisation and poor oral health literacy within ASEAN has to be urgently addressed before other changes can effectively occur. 2. There is a drive for more training of dental providers in DOH care, across primary to specialist services in ASEAN. 3. Social perceptions is an important challenge in SCD services within ASEAN. 4. There is a consensual appeal for more state-level support to enhance DOH in ASEAN.
This is the conundrum of a disadvantaged cohort, an overlooked health aspect, within impoverished communities. A purposeful multi-sector effort is paramount to internally align national strategies, in order to achieve equity for DOH in each country of ASEAN.
Footnotes
Acknowledgements
The authors would like to express their heartfelt gratitude to the International Association of Disability and Oral Health for this trans-national research. In addition, many thanks to Ms Luo Xue Shi, senior analyst epidemiologist from the Ministry of Health Holdings Singapore for her relentless work, and the ASEAN dentists who provided their insights to the survey.
Author contributions
Lim GXD has worked through all stages of the study including planning. All authors distributed the surveys and liaised with their respective national health departments for congruence. All have reviewed and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Correction (November 2023):
Article title has been revised in this version.
Ethical approval
Ethical approval was not sought for the present study because it constituted an evaluation survey. This study was completed in accordance with the Declaration of Helsinki and Personal Data Protection Act (Singapore).
Informed consent
Written informed consent was obtained from all subjects before the study.
Trial registration
(where applicable): Not applicable because this study is not a clinical trial.
Availability of data
The datasets generated and/or analysed during the current study are available from david.lim.g.x@ndcs.com.sg.
All ASEAN countries are signatories of the UN Convention on the Rights of Persons with Disabilities. As advocacy for disability thrives, the recognition of oral health as an indispensable chapter of holistic health is concurrently growing.
Each ASEAN member country faces vastly unique challenges. The main cause of disability in an ASEAN nation varies, such as unexploded ordnance, herbicide remnants, non-communicable and communicable diseases. Hand-in-hand collaboration has brought about massive improvements, as seen from the ASEAN Disability Forum. So why not special care dentistry in ASEAN?
This (anonymous) survey hopes to bring about a preliminary understanding of challenges, efforts and hopes for special care dentistry in each ASEAN country. 1 Which ASEAN country do you (mainly) reside in? 2 What is your profession? • Dentist • Oral health therapist • Medical professional • Others: 3 List the five main barriers/challenges in your country that affect the adequate provision of oral health services for people with disabilities. (Open-ended) 4 List five ways to improve and forward special care dentistry in your country. (Open-ended) 5 Rank the challenges or difficulties that you • Quality/Quantity: lack of training of dentists/dental staff; too many patients with disabilities • Access: difficulty for distant outreach; lack of mobility-enabled dental services • Social-economics: financial constraints affecting service provision directly or indirectly • Social perception: lack of public recognition of importance of oral health; lack of recognition of rights and health needs for people with disabilities • Policies/facilities: limitations in logistics/equipments/services (e.g. GA) affecting delivery of adequate care; restriction in care due to various existent policies/protocols 6 In what ways do you think ASEAN member countries, despite their unique challenges, can collaborate to support the development of special care dentistry in the region? (Open-ended) 7 This survey may be used in reports/policies/guidelines/publications/proposals. The responses are confidential. You can withdraw your responses anytime you deem required. After entering the data base, the responses are anonymised and can be impossible to trace. Only the two researchers will have access to anonymised data. For further enquiries, please email: • Yes, I understand and permit the use of my responses for its intended purpose. • No, I do not permit the use of the responses.