
Abstract
Objective
To examine the effect of immediate chest physiotherapy (ICPT) on pulmonary function and arterial blood gases among extubated patients.
Method
This prospective study enrolled patients aged 20–60 years who had been intubated for 48 h. They were randomly assigned to either a control or study group. The study group received ICPT by trained critical care nurses and physiotherapists, which included early mobilization, breathing exercises and airway clearance. The control group received standard nursing chest care (positioning, oral and endotracheal suctioning) without ICPT. Researchers evaluated participants using pulmonary function tests, arterial blood gas tests and mechanical ventilation parameters.
Results
The study enrolled 70 patients. There were no significant differences in the sociodemographic characteristics and medical data before intubation between the two groups except for preparatory education. After extubation, the vital capacity was significantly higher in the study group compared with the control group. There were also significant differences between the two groups in other lung function tests and arterial blood gas tests. After extubation, the total lung capacity, functional residual capacity and residual volume were significantly higher in the study group compared with the control group.
Conclusion
The use of ICPT improved both pulmonary function and arterial blood gases.
Introduction
Immediate chest physiotherapy (ICPT), which includes coughing, deep breathing exercises and chest vibration, has been demonstrated to enhance lung function and reduce the period of mechanical ventilation after being extubated. 1 Studies have also found that ICPT can lower the incidence of pneumonia and lead to a shorter stay in the intensive care unit (ICU).2–5 It is important to prevent extubation failure following a critical illness, as reintubation is associated with worse outcomes, longer hospitalization and higher rates of tracheotomies.6,7
Severe deterioration, prolonged immobility and long-term mechanical ventilation are major risk factors for respiratory complications and muscle weakness in critically ill patients.8,9 Early physiotherapies have emerged as a crucial component of their care, as they can enhance physical and mental functions. 10 Chest physiotherapy refers to a group of procedures that clear secretions, improve breathing effort, expand the lungs, prevent lung collapse and enhance gas exchange.11,12
Physiotherapists have a crucial role in caring for patients with acute, sub-acute and chronic respiratory disorders and in avoiding the consequences of immobility and bed rest. 13 Physical therapy is a vital intervention in reducing the adverse outcomes of extended immobilization and mechanical ventilation during a severe illness. 14 The treatment plan devised by the physiotherapist is personalized to meet the most pressing demands of the patient, considering their level of consciousness, psychological state and physical fitness. 15
Pulmonary function testing aims to evaluate the efficiency of lung function using various tests. spirometry, which measures the amount of air the lungs can contain and the ability to forcefully exhale air, is the most basic examination used. 15 This test is used to detect disorders that affect lung volume and as a screening tool for conditions such as chronic obstructive pulmonary disease and asthma that affect the airways. 16
Numerous studies have emphasized the significance of addressing pulmonary function in critically ill patients. For instance, a study carried out in Egypt demonstrated that implementation of chest physiotherapy resulted in a notable improvement in pulmonary function and a reduced occurrence of respiratory complications among critically ill patients. 4 Similarly, previous studies reported a positive association between chest physiotherapy and improved oxygenation, reduced hospitalization duration and decreased mortality in critically ill patients.17–20 Therefore, investigating the effect of immediate chest physiotherapy on pulmonary function among extubated patients in critical care units is crucial in improving patient outcomes. Nurses play a critical role in managing pulmonary function and should be involved in the implementation and monitoring of chest physiotherapy as a respiratory therapy intervention. 21
This current study aimed to examine the effect of ICPT on pulmonary function and arterial blood gas readings among extubated patients in critical care units. The findings of this current study could potentially contribute to the existing literature and provide valuable insights into the effectiveness of chest physiotherapy as a respiratory therapy intervention. The hypothesis of the current study was that ICPT would lead to improvements in pulmonary function and arterial blood gas readings among extubated patients in critical care units.
Patients and methods
Study design, setting and population
This prospective study enrolled patients at the critical care unit of Mansoura Main University Hospital, Mansoura, Egypt between June 2018 and October 2018. The critical care unit consists of 10 beds and is well-equipped with equipment, supplies and advanced technologies needed for the care of critically ill patients. The nurse-to-patient ratio in each unit is nearly 1:2 during the morning shift. The inclusion criteria were as follows: (i) aged 20–60 years; (ii) intubated for 48 h. The exclusion criteria were as follows: (i) patients suffering from brain death; (ii) respiratory failure; (iii) ventilator-dependent patients: (iv) patients receiving palliative care; (v) patients on tracheostomy.
Study participants were randomly assigned to either a control or study group. Random assignment was achieved through drawing from a hat, ensuring each patient had an equal chance of being placed in either group. The study group received ICPT by trained critical care nurses and physiotherapists, which included early mobilization, breathing exercises and airway clearance. The control group received standard nursing chest care (positioning, oral and endotracheal suctioning) without CPT management.
Ethical approval was obtained from the Ethical Committee of Faculty of Nursing, Mansoura University, Mansoura, Egypt (no: P.0443). Signed informed consent was obtained from the families of the patients and verbal approval from obtained from the patients. Coding was used to refer to the patients instead of using their names, thereby ensuring their anonymity and de-identifying all patient details. The participants were duly informed that all data gathered during the research would be held in strict confidence and solely used for scientific purposes. The reporting of this study conforms to the STROBE guidelines. 22
Pilot study methods
The study began with a pilot study that included 10% of the total sample. The pilot study was conducted to evaluate the feasibility and clarity of the study tools; and necessary modifications were made accordingly. Data collection for the study included four assessments for each patient as follows: (i) a pulmonary function test was conducted using a spirometer; (ii) arterial blood gases (ABG) were tested and recorded; (iii) mechanical ventilation parameters were recorded within the first 4 h before extubating the patients; (iv) ICPT was administered to extubated patients and the effect on pulmonary function was evaluated for 1 week.
Fieldwork for nurse training programmes
An experienced physical therapist conducted training programmes for the nurses who provided direct care for the study group. The training covered the aim, steps, types and techniques of CPT. Patients were assessed and received chest physiotherapy from physiotherapists and trained qualified nurses. The treatment protocol for chest physiotherapy included ‘exercises for the inspiratory muscles, manual hyperinflation, chest wall mobilization, rib-cage compression, postural drainage, secretion removal, cough function training, and early mobilization’ based on evidence-based protocols.13,23
ICPT methods
The following physical therapy methods were used in the study group for ICPT: (i) chest percussion: also known as clapping or cupping, this technique involves rhythmic and gentle striking of the chest with cupped hands or specific percussion devices. It helps to dislodge and mobilize thick secretions in the airways; (ii) postural drainage: patients are positioned in specific postures to facilitate the drainage of secretions from different lung segments. Gravity assists in moving the mucus towards larger airways for easier clearance. Different positions may include lying flat with head down, on the side, or at an incline; (iii) chest vibration: after percussion or during exhalation, the hands are placed on the chest wall, and gentle vibrations are applied to help loosen and mobilize secretions. The level of exercise intensity was determined based on the physiological responses of the patients. Range-of-motion exercises were also conducted, including upper and lower extremities. Pulmonary function was assessed for both groups using mechanical ventilation parameters, arterial blood gases tested three times per day.
Validity and reliability of the questionnaire
Prior to implementation, a meticulous evaluation of the questionnaire's face and content validity was conducted by a panel of three distinguished experts in the field of critical care. These experts were selected based on their extensive knowledge and expertise in the domain, and their valuable feedback and comments were sought to ensure the instrument's validity. The reliability of the tool was statistically tested using the Cronbach alpha test, which yielded a coefficient of 0.876.
Data collection
The primary and secondary outcomes of the study were measured as follows. The primary outcomes included pulmonary function tests and ABG.
Pulmonary function tests were conducted noninvasively using a spirometer, measuring vital capacity (VC), forced vital capacity (FVC), forced expiratory volume in 1 s (FEV1), FEV1/FVC ratio and maximal voluntary ventilation (MVV) as described previously. 24 This test was conducted once per day for 3 days.
Arterial blood gases were measured as previously described. 25 The ABG tests were used to examine the effect of ICPT on a gas exchange, including pH, PaO2, PaCO2, HCO3 and SaO2. This test was conducted three times a day, once per shift, and the mean was calculated per day.
Mechanical ventilation parameters were measured using a tool developed previously. 26 The assessment was conducted within the first 4 h before removing the endotracheal tube (ETT). The tool consists of seven items, including modes of ventilation, fraction of inspired oxygen, tidal volume and positive end-expiratory pressure (PEEP).
For the secondary outcomes, baseline characteristics were recorded using a questionnaire, which was designed to gather sociodemographic characteristics (age, sex, marital status, residential location, employment status) and medical information (medical diagnoses, chronic illnesses, prior hospitalizations, prior operations).
Statistical analyses
The sample size was calculated based on the G*Power 3.1.2 tool with a power of 85%, confidence level (1-alpha error) 95%, alpha 0.05 and beta 0.15. Each group required a minimum sample size of 26.
All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 25.0 (IBM Corp., Armonk, NY, USA). In terms of demographic characteristics and medical information, continuous data are presented as mean ± SD and categorical data as frequencies (%). Student’s t-test was used to compare continuous data between the two groups. χ2-test was used to compare categorical data between the two groups. A P-value < 0.05 was considered statistically significant.
Results
This prospective study enrolled 70 patients who were randomly assigned to either the control group (n = 35) or the study group (n = 35) (Figure 1). The sociodemographic data for both groups are shown in Table 1. The mean ± SD age of control group was 37.9 ± 6.5 years and that of the study group was 38.2 ± 7.3 years. In the control group, 22 of 35 patients (62.9%) were male and 25 of 35 patients (71.4%) were married. In the study group, 20 of 35 patients (57.1%) were male and 27 of 35 patients (77.1%) were married. There were no significant differences in the sociodemographic characteristics between the two groups except for preparatory education, which was significantly more common in the study group (P = 0.047).

Flow chart showing progress through enrolment, randomization and analysis of patients (n = 70) who had been intubated for 48 h and were included in a study to examine the effect of immediate chest physiotherapy (ICPT) on pulmonary function and arterial blood gas readings.
Comparison of the sociodemographic characteristics between the control (n = 35) and study (n = 35) groups of patients who had been intubated for 48 h and were included in a study to examine the effect of immediate chest physiotherapy on pulmonary function and arterial blood gas readings.

Data presented as n of patients (%).
P = 0.047; χ2-test was used to compare categorical data; no other significant between-group differences (P ≥ 0.05).
The medical data for both groups are shown in Table 2. There were no significant differences in the medical data between the two groups.
Comparison of the medical data between the control (n = 35) and study (n = 35) groups of patients who had been intubated for 48 h and were included in a study to examine the effect of immediate chest physiotherapy on pulmonary function and arterial blood gas readings.
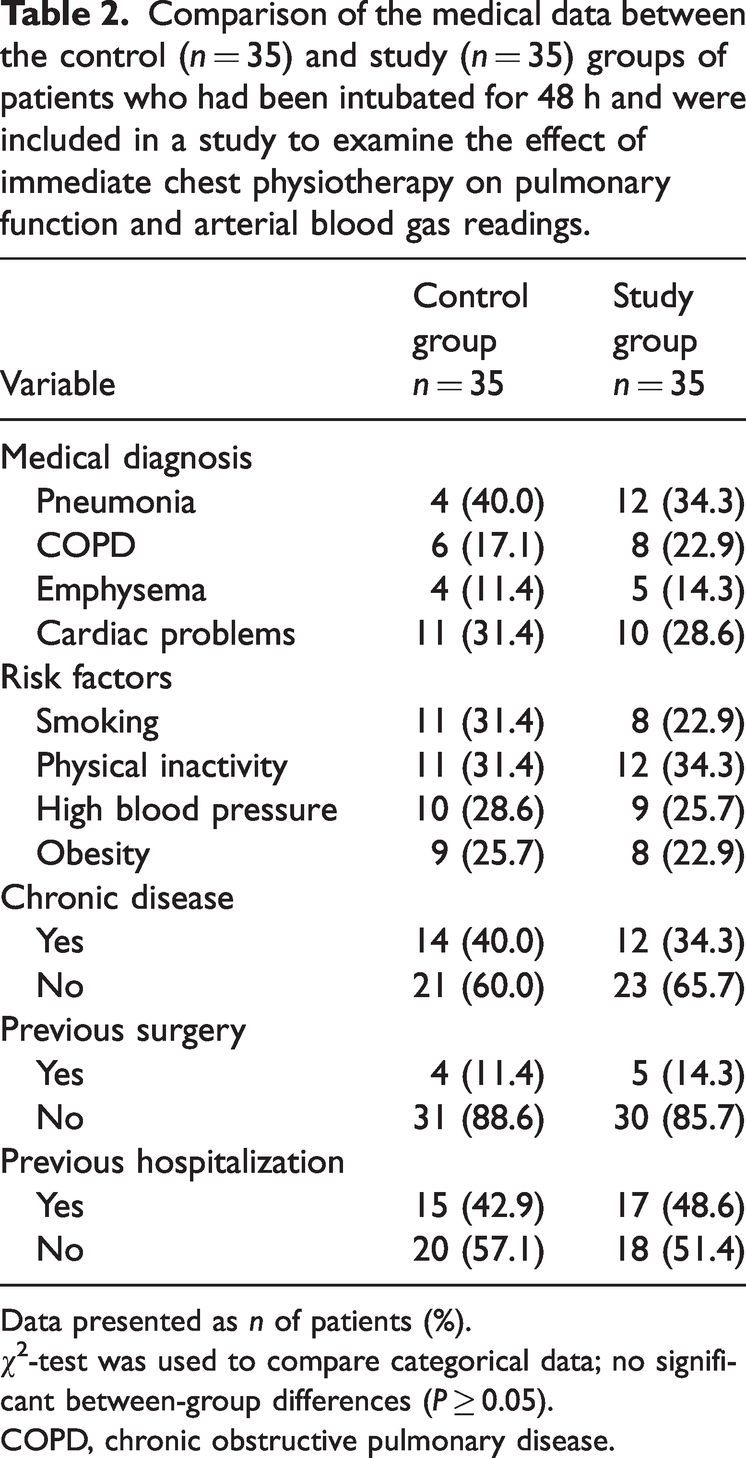
Data presented as n of patients (%).
χ2-test was used to compare categorical data; no significant between-group differences (P ≥ 0.05).
COPD, chronic obstructive pulmonary disease.
There were no significant differences in the mean ± SD values for tidal volume, FiO2, PEEP, pressure support (PS), ETT size and cuff pressure between the two groups at 4 h before extubation (Table 3). There was a significant difference in the mean ± SD rate of mechanical ventilation between the two groups (P = 0.016).
Comparison of the mechanical ventilation parameters prior to extubation between the control (n = 35) and study (n = 35) groups of patients who had been intubated for 48 h and were included in a study to examine the effect of immediate chest physiotherapy on pulmonary function and arterial blood gas readings.

Data presented as mean ± SD.
P = 0.016; Student’s t-test was used to compare continuous data; no other significant between-group differences (P ≥ 0.05).
PEEP, positive end-expiratory pressure; PS, pressure support.
After extubation, the mean ± SD VC was significantly higher in the study group compared with the control group (P = 0.008) (Table 4). The mean ± SD FVC, FEV and MVV were also significantly higher in the study group compared with the control group (P < 0.05 for all comparisons). The mean ± SD FEV1/FVC ratio was significantly lower in the study group compared with the control group (P = 0.036).
Comparison of the pulmonary function after extubation between the control (n = 35) and study (n = 35) groups of patients who had been intubated for 48 h and were included in a study to examine the effect of immediate chest physiotherapy on pulmonary function and arterial blood gas readings.

Data presented as mean ± SD.
Student’s t-test was used to compare continuous data.
FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity.
After extubation, the mean ± SD pH, PaO2, HCO3 and SaO2 were significantly higher in the study group compared with the control group (P < 0.05 for all comparisons) (Table 5). The mean ± SD PaCO2 was significantly lower in the study group compared with the control group (P = 0.031).
Comparison of the arterial blood gas test results after extubation between the control (n = 35) and study (n = 35) groups of patients who had been intubated for 48 h and were included in a study to examine the effect of immediate chest physiotherapy on pulmonary function and arterial blood gas readings.

Data presented as mean ± SD.
Student’s t-test was used to compare continuous data.
After extubation, the mean ± SD values of total lung capacity, functional residual capacity and residual volume were significantly higher in the study group compared with the control group (P < 0.05 for all comparisons) (Figure 2).

Comparison of the pulmonary function tests between the control (n = 35) and study (n = 35) groups of patients who had been intubated for 48 h and were included in a study to examine the effect of immediate chest physiotherapy on pulmonary function and arterial blood gas readings. Data presented as mean ± SD; Student’s t-test was used to compare continuous data between the two groups; #P < 0.05. The colour version of this figure is available at: http://imr.sagepub.com.
Discussion
This current prospective study demonstrated that ICPT improved both pulmonary function and arterial blood gases. ICPT was executed efficiently. The findings of the current study showed that at 4 h before extubation, there were no significant differences between the two groups in tidal volume, FiO2, PEEP, PS, ETT size and cuff pressure. However, a significant difference was observed in the rate of mechanical ventilation between the two groups. Attempts were made to standardize the variables and characteristics of the patients as much as possible to identify the effects of the interventions. The lack of significant differences between the control and study groups in relation to the mechanical ventilation parameters might be due to standardization of patient variables and characteristics to ensure any observed effects were related to the interventions. These findings differ from those previously reported, 27 which described differences in ventilator parameters between the studied groups.
The current study utilized spirometry to assess pulmonary function postextubation and found a significant difference in the VC between the control and study groups. There were also significant differences between the two groups in terms of FVC, FEV, FEV1/FVC ratio and MVV. These results were consistent with previous studies,28,29 which demonstrated that chest physiotherapy can prevent airway secretion retention, maintain lung compliance and improve lung secretions in mechanically ventilated patients. In addition, the current findings were in line with a previous study that demonstrated significant improvements in all parameters for patients undergoing chest physiotherapy compared with the control group. 30
The findings of the current study indicate a slight but significant improvement in total lung capacity, functional residual capacity and residual volume in the study group when compared with the control group. These current findings were in agreement with a previous study, 31 which reported a significant increase in maximum inspiratory pressure in the training group. In another study, 32 the study group's lung capacity and inspiratory muscle strength were significantly higher than those of the control group. Chest physiotherapy is commonly utilized to enhance ventilation and gas exchange in infants and children with lung disease who are mechanically ventilated. 33
Previous research studies have highlighted the potential competition for energy between respiratory muscles working extremely hard and other organs during the shift from mechanical ventilation to spontaneous breathing trial (SBT).34,35 The respiratory muscles may deprive the brain of blood and oxygen in this situation, which would contribute to weaning failure. 36 Additionally, during the weaning process, restrictions in cerebral cortex blood flow may aggravate stress and anxiety sensations, which may then contribute to tachypnoea and uncoordinated breathing. 37 A recent study conducted in Belgium found that SBT-failure patients experienced an inadequate increase in prefrontal brain perfusion, which may have contributed to the lower differential response in prefrontal cortex oxygen saturation (%StiO2) compared with the success group. 38 Prefrontal cortex %StiO2 decreases of greater than 1.6% during SBT were identified as sensitive indicators of SBT failure. 38 The current study showed slight but significant differences between the control and study groups in ABG parameters, including pH, PaO2, PaCO2, HCO3 and SaO2. This was consistent with previous studies,19,20 which also reported improvements in oxygen saturation after chest physiotherapy. A previous study also found a significant increase in PaO2/FiO2 in the CPT group compared with the control group. 39 Chest physiotherapy has been demonstrated to improve lung mechanics and aid in secretion clearance. Consequently, the reduction in airway resistance and obstruction caused by secretions and bulges that cause higher airway pressure and decreased lung compliance, may account for the improvement in ABG. 40 Furthermore, CPT was found to be effective in acute lung collapse, improving oxygenation and recruiting collapsed alveoli. 41
This current study had several limitations. First, the study lacked any long-term follow-up, which prevents an assessment of whether the observed improvements were sustained over time. Secondly, the limited sample size may affect the generalizability of the study.
In conclusion, ICPT provided a significant improvement in FVC, FEV, FEV1/FVC ratio MVV indicating enhanced lung function. Moreover, there was an improvement in ABG after ICPT. Incorporating chest physiotherapy may have the potential for shorten hospitalization duration and healthcare costs, which could benefit patients and healthcare systems. However, it is important to note that while these results are promising, further research and clinical evaluation are needed to determine the full extent and generalizability of the effect of chest physiotherapy on critically ill patients.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605231208600 - Supplemental material for Enhancing pulmonary function and arterial blood gas readings through immediate chest physiotherapy among extubated patients in ICU
Supplemental material, sj-pdf-1-imr-10.1177_03000605231208600 for Enhancing pulmonary function and arterial blood gas readings through immediate chest physiotherapy among extubated patients in ICU by Fadia Ahmed Abdelkader Reshia, Basma Salameh, Nourah Alsadaan, Mohammed Alqahtani, Ahmad Ayed, Maysa Fareed Kassabry and Asmaa Ibrahem Abo Seada in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605231208600 - Supplemental material for Enhancing pulmonary function and arterial blood gas readings through immediate chest physiotherapy among extubated patients in ICU
Supplemental material, sj-pdf-2-imr-10.1177_03000605231208600 for Enhancing pulmonary function and arterial blood gas readings through immediate chest physiotherapy among extubated patients in ICU by Fadia Ahmed Abdelkader Reshia, Basma Salameh, Nourah Alsadaan, Mohammed Alqahtani, Ahmad Ayed, Maysa Fareed Kassabry and Asmaa Ibrahem Abo Seada in Journal of International Medical Research
Footnotes
Acknowledgements
We extend our heartful gratitude to all the patients who participated in this study.
Declaration of conflicting interests
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.