
Abstract
Bradyarrhythmia as a result of significant weight loss post-bariatric surgery is slowly gaining recognition in few case reports and even fewer studies. However, awareness of its diagnosis and management amongst physicians remains modest. We report a case of asymptomatic sinus bradycardia in a 41-year-old woman who shed 19.5 kg/m2 in 4 months following bariatric surgery. The pathophysiology, diagnostics and management of post-bariatric surgery sinus bradycardia is briefly discussed.
Introduction
Bradyarrhythmia as a result of significant weight loss post-bariatric surgery is slowly gaining recognition in few case reports and even fewer studies. However, awareness of its diagnosis and management amongst physicians remains modest. We report a case of asymptomatic sinus bradycardia in a 41-year-old woman who shed 19.5 kg/m2 in 4 months following bariatric surgery. The pathophysiology, diagnostics and management of post-bariatric surgery sinus bradycardia is briefly discussed.
Case Report A 41-year-old woman with no underlying medical illnesses was found to be bradycardic during a pre-employment assessment in a walk-in clinic. She reported no light-headedness, difficulty breathing, pre-syncope or syncope and had good exercise tolerance. She was not on any prescribed medications, supplements nor alcohol and reported no previous history of coronary artery disease. Her family history was unremarkable for cardiac diseases. Her surgical history was significant for a laparoscopic sleeve gastrectomy in April 2021 before which she weighed 119 kg (BMI 50.4 kg/m2) and suffered from hypertension, pre-diabetes and irregular menses. Her pre-surgical heart rate was reportedly 90–95 bpm. Four months post-surgery, she weighed 73.0 kg (BMI 30.9 kg/m2) having lost 46 kg and had all blood pressure, glucose levels and menstrual irregularities revert to normal without treatment. On examination, she was alert, comfortable in room air, pink, afebrile and clinically euthyroid. Cardiovascular, respiratory and abdominal examinations were unremarkable except for well-healed keyhole scars on the abdomen. Her heart rate was regular at 46 bpm with a blood pressure of 124/70 mmHg and 99% oxygen saturation in room air. Electrocardiogram showed sinus bradycardia at 48 bpm with no bundle branch block or prolonged PR and QT intervals (Figure 1). Blood investigations including serum sodium, potassium, magnesium, calcium, phosphate, thyroid-stimulating hormone, CK-MB mass and high-sensitivity C-reactive protein were within reference limits. eGFR was > 90 mL/min/1.73 m2 and urine toxicology screening returned negative results (Table 1). A chest X-ray that was done as part of the pre-employment assessment was also normal. Electrocardiogram tracing of the patient at rest. Serum Biochemistry Test Results of the Patient on Presentation. Given her clinical status and unremarkable diagnostic test findings, no further investigations were conducted, and she was allowed to self-monitor at home without treatment. On outpatient reassessment 2 months later, her heart rate had normalized to 80 bpm and she reported good tolerance of moderate-intensity exercise.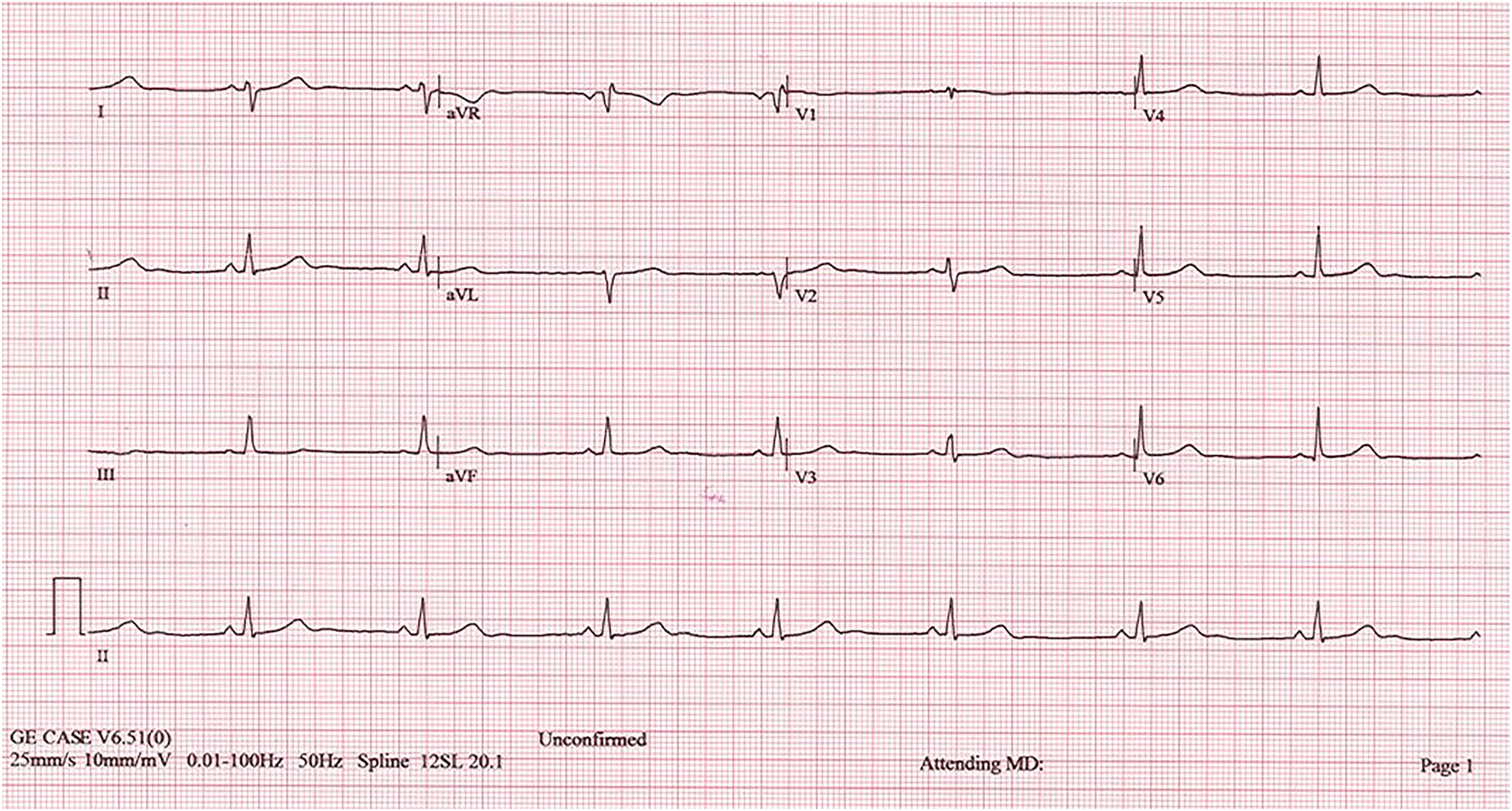

Discussion
Obesity has become a global epidemic, having tripled to 13% of the population worldwide since 1975. It is a recognized contributor to multiple non-communicable diseases including diabetes mellitus, coronary artery disease and cancers, causing at least 2.8 million deaths per year. 1 Bariatric surgery is an effective long-term weight-loss modality that has been shown to reduce the risks of obesity-related diseases, hospitalization rates, total direct healthcare costs as well as mortality rates. 2
Although weight loss has been shown to produce favourable medical outcomes including reversal of metabolic diseases, it is not without physiological ramifications. Based on the few reported cases in medical literature, increased cholinergic tone manifesting as bradycardia and delayed chronotropic response on stress test has been reported in post-bariatric surgery patients with significant weight loss.3–5
In a systematic review by Malik et al. 6 involving 137 obese subjects undergoing bariatric surgery, 18.2% of the subjects were found to have asymptomatic sinus bradycardia (SB) post-operatively. The same review also showed a positive relationship between the degree of BMI lost with the overall occurrence of SB as well as the persistence of SB. Whilst most subjects in the study were found to have SB between 393–436 days post-surgery, the diagnosis of SB in our case was made earlier at 4 months post-surgery. It should be noted that Malik’s study defined bradycardia as a heart rate of < 60 bpm in contrast to the American Heart Association’s cutoff of 50 bpm 7 ; thus, overestimation is plausible where definitions differ.
Leptin has been shown to cause sympathetic overdrive in obese individuals through its sympatho-excitatory effect on the hypothalamus and its levels are directly proportional to BMI and heart rate.8,9 The increase in leptin along with other endogenous factors such as insulin and cytokines contribute to the development of hypertension, diabetes mellitus and atherosclerosis in obese subjects.9,10 As leptin levels decrease with weight loss, vagal tone is augmented and sympathetic overtone on the sinus node is withdrawn, thus causing bradycardia. 8 The direct relationship between leptin and BMI also explains the reversal of metabolic diseases without treatment following weight loss, such as in this case.
Thorough clinical assessment and resting electrocardiogram are requisites in investigating bradycardia. To date, no study has evaluated the benefits of elaborate laboratory testing in working up bradycardia. Nonetheless, basic laboratory tests, such as serum electrolytes, pH and thyroid-stimulating hormone, are useful in aiding diagnosis of conditions commonly associated with bradycardia. 7 Specific laboratory and radioimaging tests should be catered to specific conditions such as intrinsic heart disease, infections, infiltrative diseases and rheumatological conditions based on clinical suspicion and pre-test probability.7,11 In this case, good exercise tolerance, absence of clinical features and an identifiable event preceding the onset of bradycardia resulted in low clinical suspicion of said conditions. Furthermore, ECG features such as prolonged PR-interval, poor R-wave progression, low QRS voltage and ventricular hypertrophy, as well as extra-cardiac manifestations that would suggest infiltrative cardiomyopathy, were absent. 12 The transient nature of bradycardia, established on follow-up, further negated the need for additional investigations.
Treatment is not typically required in post-bariatric surgery SB except in symptomatic cases where administration of anticholinergics has been reported to be helpful. 3 Focus should be directed towards managing compounding comorbidities such as obstructive sleep apnea (OSA) as arrhythmias resolve with treatment of the comorbidity alone. 5 Furthermore, post-bariatric surgery SBs are usually asymptomatic and 80% of cases resolve without treatment. 6 In a retrospective study by Clapp et al., 13 only 0.8% of post-bariatric surgery patients required pacemaker insertion, the main indication of which was sick sinus syndrome. However, subjects with OSA were not excluded in the study and determining obesity or weight loss as the cause of arrhythmia could not be ascertained.
Conclusion
With the increasing number of bariatric surgeries performed in tandem with obesity rates, physicians should be aware of the physiological responses to significant weight loss such as sinus bradycardia. This awareness not only reduces patient anxiety but also reduces unnecessary investigations and treatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.