
Abstract
Ewing sarcoma (ES) of the extraskeletal form is a rare occurrence and even rarer to manifest in the sinonasal tract. We describe a case of an advanced sinonasal ES with orbital and intracranial extension that was managed with chemotherapy and endoscopic surgery. Despite completing chemotherapy and surgical resection, the tumor progressed rapidly even before postoperative radiotherapy, and subsequently, she succumbed to death due to sepsis. We would like to discuss the management challenges, pitfalls, and surgical approach which may improve the outcome of this complicated disease.
Introduction
Ewing sarcoma (ES) is a malignant tumor that can manifest itself in skeletal and extraskeletal forms. The extraskeletal type is uncommon in the head and neck area and even more uncommon in the sinonasal tract. Prevalence is higher in males especially in early adulthood. 1 Diagnosing ES is challenging owing to the few differentials of a small blue round cell tumor. A diagnosis is made based on immunohistological (IHC) staining and molecular analysis for confirmation in ambiguous cases. 1 Multimodality treatment with chemoradiotherapy combined with endoscopic surgery has been recommended as strategies to control this poor prognostic disease. Five-year survival rates are low especially in patients with distant metastasis.
Case report
A 45-year-old woman presented with right nasal blockage which was progressively worsening associated with hyposmia, intermittent epistaxis, and blurring of vision of the right eye over 3 months duration. She denied facial pain, foul-smelling nasal discharge, neck swelling, and constitutional symptoms. Rigid nasal endoscopy showed a vascular reddish mass with a smooth surface occupying the whole right nasal cavity until the floor and right posterior choana (Figure 1). A vascular reddish mass that bleeds on probing and occupying the whole right nasal cavity till the floor (arrow).
Contrast-enhanced computed tomography (CECT) of the paranasal sinus revealed an enhancing soft tissue mass measuring 2.7 × 3.8 × 4.6 cm (AP × W × CC) occupying the entire right nasal cavity and extends posteriorly to the right posterior choana. The findings were suggestive of aggressive right sinonasal mass with bony erosions, intracranial extension, and right intraorbital extension. Urgent biopsy of the right nasal mass revealed small round cell tumor and immunohistochemistry staining was positive to CD99, synaptophysin, and FLI1. Findings were in favor of ES or primitive neuroectodermal tumor (PNET). Staging bone marrow trephine biopsy was negative for tumor infiltration; hence, the TNM staging was T1 N0 M1. She was further investigated with magnetic resonance imaging (MRI) of the brain and CECT of the thorax, abdomen, and pelvis for staging which confirmed the extension of mass into the right nasal cavity, ethmoidal air cells, sphenoid sinus, right orbit, and extradural involvement with multiple lung nodules suggestive of lung metastasis (Figure 2). Sagittal view of contrasted MRI T2-weighted image showing the mass originated from the right nasal cavity and extending into right ethmoidal air cells, sphenoid sinus, right orbit, and extradural.
The management strategies were discussed during a multidisciplinary board meeting. She was planned for neoadjuvant chemotherapy followed by endoscopic surgical resection and postoperative radiotherapy to the primary lesion and bilateral lungs. She was started on intensive induction chemotherapy of vincristine, ifosfamide, doxorubicin, and etoposide (VIDE) for six cycles. However, she defaulted for 6 months after the first cycle due to logistic issues and had multiple admissions in between for neutropenic septicemic shock. She eventually completed six cycles of VIDE after 11 months. Repeat CT TAP revealed a significant 78% reduction of the lesion and stable lung nodule. Subsequently, she had endoscopic surgical resection of the tumor under image guidance. Intraoperatively, the tumor originated from the lateral wall of the right posterior ethmoid and eroded the right lamina papyracea exposing the periorbital fascia. We performed resection of the tumor with a microdebrider with an intent of clear margins. Postoperatively, the tumor margins were positive at the right periorbital and right medial orbital region.
The resected tumor has the same histopathology features as was observed in the initial biopsy. The tumor cells were arranged in diffuse pattern, and some has vague rosette-like pattern surrounding the blood vessels. The tumor cells were small to medium in size and have round to oval nuclei, and fine chromatin and inconspicuous nucleoli. The cytoplasm was scanty (Figure 3). Repeat IHCs were done, to exclude other differential diagnoses due to poor respond to the treatment. NK/T-cell lymphoma was excluded with negative staining of CD3 (T-cell marker) and focal scanty staining of CD56. It was observed that the CD56 positive cells were also expressing synaptophysin and chromogranin A. All of these 3 markers are known to be focally positive in cases of ES. Other differential diagnosis, such as myeloid sarcoma was also excluded, with negative myeloperoxidase expression despite CD117 was positive for tumor cells. The tumor cells are arranged in diffuse pattern, and some has vague rosette-like pattern surrounding the blood vessels. The tumor cells are small to medium in size and have round to oval nuclei, and fine chromatin and inconspicuous nucleoli.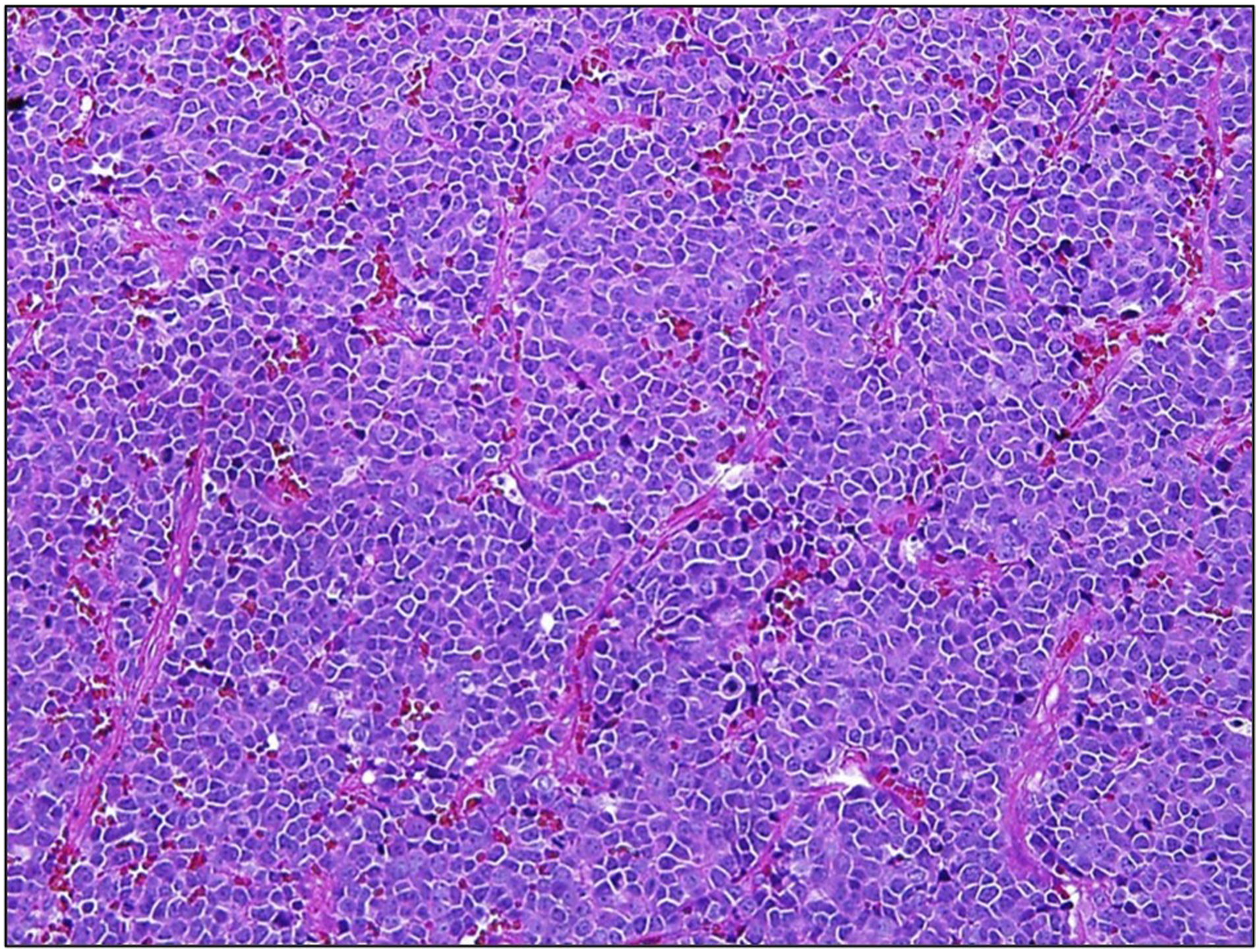
CT simulation for radiotherapy planning, which was done 1 month after surgery, however, showed huge tumor progression with worsening intraorbital and intracranial extension. Hence, ifosfamide, carboplatin, and etoposide (ICE) regime as second-line chemotherapy was started instead of radiotherapy. However, 1 week after the first cycle of ICE, the patient succumbed to death due to neutropenic sepsis with severe metabolic acidosis and multiorgan failure.
Discussion
Ewing’s sarcoma of the head and neck is extremely rare accounting for 4% of all Ewing’s sarcoma cases. The maxilla is the commonest affected site and the nasal cavity being the least common. 2 ES belongs to a group of tumors with neuroectodermal differentiation and is categorized as a peripheral PNET. 3
Diagnosing ES is challenging due to broad differential diagnoses for small round cell tumors in the sinonasal tract such as olfactory neuroblastoma, sinonasal undifferentiated carcinoma, rhabdomyosarcoma, NK T-cell and myeloid sarcoma. Simons et al. published a systematic approach to guide pathologists in diagnosing ES. Positive IHCs for CD99 and synaptophysin greatly suggest PNET/ES. 3 In uncertain cases, molecular analysis by identification of t(11;22)(q24;q12) translocation is the hallmark for diagnostic confirmation. 3 In this case, the diagnosis was made based on the morphology supported by the IHCs, CD99 (strong membranous), FLI1 (strong), chromogranin A/synaptophysin (focal), and CD56 (focal). CD117 (c-kit) was also positive in our case. A study showed that CD117 is expressed in 75.8% of ES and it did not have significant prognostic value. 4 Establishing a diagnosis will implicate on correct management of this difficult disease.
Ewing sarcoma is a systemic disease, and the mainstay of treatment is neoadjuvant chemotherapy followed by definitive surgery and or radiotherapy. The current practice according to European EURO EWING 99 recommended combination of vincristine, doxorubicin, ifosfamide, and etoposide for 42 weeks for both localized and metastatic disease. In good responders, this is followed by surgery and or radiotherapy to primary and metastatic sites. 5 Consolidation chemotherapy is then continued with the same agents for another 30–48 weeks in metastatic disease. 5 Tumor response to chemotherapy significantly affects the overall survival rate of Ewing’s sarcoma patients. 6 Shrinking the tumor volume by chemotherapy will help in achieving local control and negative margins by surgery either open or endoscopically. The pitfall in this case was the delay in completing full cycles of chemotherapy. Our case responded well after the first cycle; however, the delay in the second cycle may contribute to the aggressive and rapid progression of the tumor. It is proven that lower compliance to chemotherapy will lead to a lower 5-year overall survival rate and disease-free survival of 53% and 35%, respectively. 6 Apart from that, it is imperative to promptly diagnose and treat neutropenic sepsis as one of the life-threatening complications of chemotherapy with empirical antibiotics. 7
Adjuvant radiotherapy is still controversial in the management of sinonasal ES. To date, there is no study of increased survival rate with radiotherapy. Furthermore, it may lead to blindness, pituitary dysfunction, and significant morbidity owing to close vicinity to orbit and brain. Nevertheless, radiotherapy was still intended after surgery in our case considering the positive margins as proposed by Thariat et al. 8 Postoperative radiotherapy was also included in the protocol by Lepera et al. 9 Unfortunately, due to the rapid disease progression postoperatively, second line of chemotherapy was used instead.
Surgical management of ES can be approached by either craniofacial or endoscopic resection. Endoscopic transnasal surgery of sinonasal carcinoma has been shown to sustain the quality of life while achieving oncological outcomes comparable to those obtained with external methods. 10 This technique is in favor of pediatric patients and those with metastatic disease by avoiding mutilating surgery and craniofacial growth disruption. 10 However, not all cases are suitable for the endoscopic approach especially when there is involvement of the skin, infratemporal fossa, orbit, and dura. A combined endoscopic-craniofacial approach is recommended for the latter. 10
Factors affecting outcome of 5-year survival rate.

OS: overall survival; DFS: disease-free survival.
Conclusion
Ewing sarcoma of the head and neck is a rare entity with high mortality. Each patient must be managed by a multidisciplinary team to customize the treatment approach based on the tumor extension, patient’s status, and expectations. A multimodality treatment consisting of neoadjuvant chemotherapy, radiotherapy, and surgery appears to be linked to better outcomes, although a well-established guideline is yet to exist. We hope that our case in this pool of sporadic cases in the literature will help to reach a consensus in the management of sinonasal ES.
Footnotes
Acknowledgments
We would like to thank all co-authors for their assistance and guidance in this research.
Author contributions
AAAAAK wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
USM does not require ethical approval for reporting individual cases or case series because patient’s confidentiality, rights, and dignity are not disclosed in this manuscript.
Informed consent
Written informed consent was obtained from a legally authorized representative for anonymized patient information to be published in this article.
Availability of data
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.