
Abstract
Intraoperative sentinel lymph node mapping (SLNM) with methylene blue dye (MBD) tracer has been the recommended method to detect SLN in early-stage breast cancer patients in low-resource settings. However, the use of MBD alone is hampered by the high false-negative rate; thus, it requires coupling with other mapping methods if the appropriate infrastructure and services are available. In this article, we present two prospective cases detailing our initial experience using the gold-standard dual tracer technique (DTT: MBD and 99mTc-nanocolloid radioisotope) in combination with hybrid single-photon emission computed-tomography/computed-tomography (SPECT/CT) preoperative mapping for image-guided SLN biopsy (SLNB). Overall, both studies were successful in identifying the SLNs, which aided in mapping the possible anatomical spread of the disease.
Keywords
Introduction
Sentinel lymph node biopsy (SLNB) has gained importance as the standard-of-care for early-stage breast cancer patients with negative axillary lymph nodes (ALNs). 1 A successful SLNB is determined by the mapping (SLNM) approach as it influences the identification (IR) and false-negative rate (FNR). However, current SLNM standards require specialized instruments and other resources that are typically unavailable or limited in low-resource settings.2,3
According to the Breast Health Global Initiative, the intraoperative blue dye tracer is the recommended SLNM technique in low-resource settings. 2 Radioisotope tracer mapping via preoperative lymphoscintigraphy and intraoperative gamma-probe was also recommended for institutions with enhanced resource levels.2,3 Combining blue dye with radioisotope was found to yield a superior IR and FNR compared to using either tracer alone.1,4,5 Although no standard methodology exists, the dual tracer technique (DTT) is considered as the gold-standard in many guidelines. Recently, single-photon emission computed-tomography/computed-tomography (SPECT/CT) was also incorporated in the preoperative SLNM workflow.6,7 This hybrid scanner provides functional and anatomical information from the SPECT and low-dose CT components, respectively. A detailed three-dimensional view of the SLN’s location is generated by SPECT/CT image co-registration, which helps to observe the surrounding structures essential for optimal image-guided surgery. 6
In Malaysia, the radioisotope technique is not widely practiced and, even more so, the use of SPECT/CT. 8 It is evident by the limited nuclear medicine services and is mainly concentrated in major cities. 9 As of 2021, there is only one nuclear medicine facility (Hospital USM, Kota Bharu, Kelantan) that serves the entire east-coast region of Peninsular Malaysia—which constitutes three states (Pahang, Terengganu, and Kelantan) with an area of roughly 64,057 km2 and ∼5 million inhabitants. Furthermore, this region, particularly Kelantan, is primarily rural and known as one of the country’s least urbanized areas. 10
We are in the early stages of establishing an institutional protocol for early-stage breast cancer management. With the recent installation of a SPECT/CT unit at Hospital USM, we sought to develop a comprehensive SLNM program using a multimodal approach despite having only modest experience, and we report the procedural outcomes including the treatment planning for two of our earliest cases.
Case Report
Case 1
A 61-year-old Chinese lady with known diabetes mellitus, hypertension, dyslipidemia, and ischemic heart disease was admitted and presented with a one-month history of right breast swelling associated with brownish nipple discharge. Physical examination showed a small firm lump at the inner lower quadrant of the right breast, and there was no palpable ALN. Mammogram followed by ultrasound-guided biopsy revealed a breast lesion measuring 0.6 cm × 1.0 cm × 1.5 cm (AP × W × CC) (BI-RADS 4), with the histopathological examination (HPE) showing papillary ductal carcinoma in situ (DCIS) of low grade. Subsequent CT staging was negative for distant metastasis. At this point, the staging was TisN0M0 (Stage IA).
Before surgery, a lymphoscintigraphy was ordered, with four injections of 99mTc-nanocolloid radioisotope (37 MBq) in 0.2 mL were administered at the periphery of the right breast tumor. Three foci of enhanced tracer uptake were observed on immediate dynamic imaging in the upper outer quadrant of the right breast, which correlated to sub-centimeter lymph nodes in the right level 1 axillary area on SPECT/CT (Figure 1(a)). Localizations of additional two foci of second echelon sub-centimeter nodes were also seen at the right level 1 axillary region. Skin marking was then made on the SLN based on real-time scanning and gamma-probe tracing. (a) SPECT/CT axial (above) and coronal (below) view showed increased tracer uptake at right level I axillary region which corresponds to sub-centimeter lymph nodes on CT. (b) Histopathological examination of one of the sentinel lymph nodes received during the frozen section. It shows a well-encapsulated lymphoid tissue contains lymphoid follicles and fibrofatty tissue. This lymph node is negative for breast cancer metastases (H&E stain, 40×).
Intraoperatively, methylene-blue dye (MBD) mapping was used to facilitate the SLNB. Three lymph nodes that were “hot” (increased radioactivity/acoustic signals on gamma-probe) and visually stained blue were removed. Frozen sections of all three lymph nodes were negative for breast cancer metastasis (Figure 1(b)); hence, ALN dissection was averted. Wide local excision of right breast lesion then ensued. HPE showed papillary ductal carcinoma in situ with a background of fibrocystic change. The immunohistochemical (IHC) study for estrogen receptor (ER) and progesterone receptor (PR) showed 95% positivity. The tumor was located 1 mm, close to the superior surgical margin. Therefore, the patient was then scheduled for external beam radiotherapy (EBRT) to the right breast instead of wider excision and started hormonal therapy with an aromatase inhibitor.
Case 2
A 46-year-old Malay female with no known medical illness presented to the hospital with a right breast lump for 1 month. There were no palpable ALN upon physical examination. Mammographic findings revealed a heterogeneously dense fibrograndular breast and subcentimeter ALN with preserved fatty hilum, whereas right breast ultrasound showed a lobulated hypoechoic lesion at 7 o’clock position 2 cm from the nipple, measuring at 1.0 cm × 1.4 cm × 1.5 cm (AP × W × CC) (BI-RADS 4). However, no significant ALN was seen. HPE from the ultrasound-guided biopsy showed an invasive carcinoma of no special type (NST) with high-grade ductal carcinoma-in-situ. Staging CT was negative for metastasis. Here, the staging was cT1N0M0 (Stage IA).
Lymphoscintigraphy was performed following four peritumoral injections of 99mTc-nanocolloid. Immediate dynamic imaging showed an increased tracer uptake at the upper outer quadrant of the right breast, which corresponds to the sub-centimeter right level 1 axillary node on SPECT/CT (Figure 2). The patient’s skin was marked over the imaged SLN and traced using a gamma-probe. SPECT/CT axial (above) and coronal (below) view showed increased tracer uptake at one right level I sub-centimeter axillary node.
SLNB with intraoperative MBD injection was performed the following day. Three SLNs were identified—the first node was “hot” and stained blue upon inspection, while the remaining nodes were “cold” (low radioactivity/acoustic signals) but visually stained blue. Levels from the frozen sections of the lymph nodes were found to be negative for malignancy. However, levels from the parafinnised tissue block displayed a micrometastasis (1 mm × 1 mm) within the subcapsular region from the first node (Figure 3 (a)), while levels of the second and third nodes were negative for malignancy. This tumor cluster was confirmed when it showed positivity for CKAE1 and AE3 (Figure 3 (b)). Histopathological examination of sentinel lymph node and right breast: (a) Section from a sentinel lymph node of the frozen section shows a cluster of malignant tumor cells (as indicated by red arrows) measuring 1 mm × 1 mm within the sub-capsular region (H&E stain, 100×). (b) The tumor cells are positive for CK AE1 & AE3 immuno-histochemical stain (IHC stain, 100×). (c) Section from wide local excision of the right breast shows invasive breast carcinoma (at lower part) with desmoplastic stromal reaction and high-grade ductal carcinoma in-situ (at upper part) (H&E stain, 100×). (d) Invasive breast carcinoma of grade 2 with moderate pleomorphism, moderate tubular formation, and mitosis (H&E stain, 200×).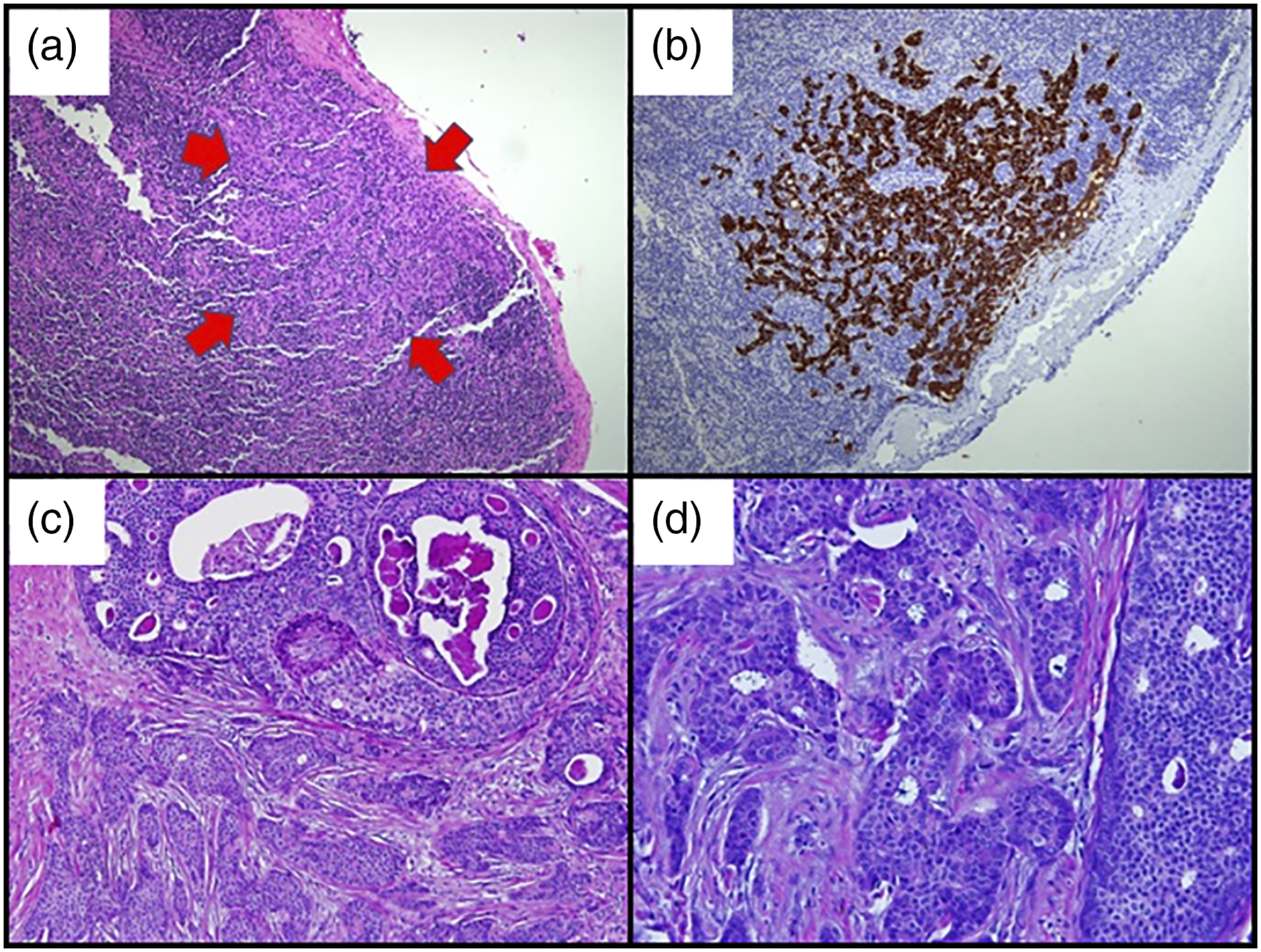
Wide local excision at the area revealed an ill-defined irregular tumor measuring 30 mm × 20 mm × 12 mm macroscopically. HPE findings showed an invasive carcinoma of NST with high-grade DCIS grade 2 and confirmed the size of 30 mm × 20 mm by histology (Figures 3(c) and (d)). ER and PR were positive 90 and 80%, respectively, while HER2 was negative (1+). The tumor was 1 mm away from the deep and superior surgical margins. The patient was upstaged to T2N1Mic (Stage IIB) following surgery. Bone scintigraphy a month later was negative for bone metastasis. The patient later planned to undergo adjuvant chemotherapy EBRT to the breast, and hormonal therapy.
Discussion
At present, blue dye is the most basic and cost-effective SLNM method, with common dye types being isosulfan-blue dye and patent-blue dye.2,3,11 MBD is an alternative blue dye more frequently used in low-resource settings due to its significantly cheaper price and easier access. According to a meta-analysis by Li et al. 11 MBD alone was found to have an acceptable IR of 91% but carried an excessive pooled FNR of 13%. Contrary to other blue dyes, MBD has yet to be associated with adverse reactions in breast cancer patients, for example, anaphylactic shock.1,6,11 Other non–life-threatening risks, for example, skin necrosis and blue tattooing have also been reported, however, none of these complications were observed in our cases.
With radioisotope, the cost of SLNM rises significantly as it requires special infrastructure, skilled operators, and extensive legislative-administrative work. Regardless, radioisotope has the inherent edge of allowing preoperative and intraoperative SLN assessment. 6 Lymphoscintigraphy, for example, can guide surgeons to trace the lymphatic drainage preoperatively, especially for patients with a history of breast/axillary surgery and EBRT; while intraoperative gamma-probe helps to specify “hot” nodes. The DTT was found to improve the SLN IR and FNR significantly—although it is slowly evolving into a unimodal approach that relies almost entirely on radioisotope due to the low contribution of blue dye in non-radioactive nodes. 6 Since troubleshooting SLNM is critical for a successful SLNB, DTT is highly recommended for cases with a high risk of false-negative, and surgeons with limited technical proficiency.1,4
Radioisotope SLNM is performed by injecting metastable technetium-99 (99mTc) isotope labeled with sulfur colloid or nanocolloid, followed by a gentle massage at the injection site to dilate the lymphatics. 4 The literature has described various injection methods (superficial vs. deep routes) but the ideal method is still contested to this day. In our protocol, we chose peritumoral injection as it is the most studied method. Although periareolar injections were shown to have more benefits, for example, easier to perform and less painful, both methods were effective and demonstrated comparable SLN identification, either via lymphoscintigraphy or gamma-probe. 12
Case schedule also serves as a challenge because the gap between injection and surgery determines the amount of radioisotope required to maintain appropriate radioactivity levels throughout the intraoperative procedures. Here, Case 1 and Case 2 were performed as a 1-day and 2-day protocol, respectively. Both methodologies were reported to produce similar IR regardless of injection method and radiotracer type. 13 Therefore, the decision is based on preferences and logistic considerations—a one-day protocol allows SLNB to be done on the same day with minimal radiation exposure, whereas a two-day protocol is advantageous in scheduling multiple patients and easing the department’s load.
Furthermore, SPECT/CT is increasingly adopted for SLNM in breast cancer and other malignancies with complex drainage pathway.6,14 Compared to conventional planar lymphoscintigraphy, SPECT/CT augments the IR by detecting more “hot” nodes affected by scattered radiation from the injection site. It is also beneficial for overweight/obese patients. 7 The additional low-dose CT helps to provide anatomical correlation for nodal localization obscured in planar imaging due to artifacts transpiring from poor activity signal and photon scattering by greater soft-tissue attenuation.7,15 SPECT/CT, however, may not be advised for all breast cancer patients due to additional cost and irradiation—although it is deemed safe for pregnant surgeons and patients. 5 Nonetheless, current evidence suggests that it is indicated whenever planar imaging is difficult to interpret, equivocal, or negative. 7
Newer tracers such as indocyanine green (ICG) have also been successfully developed for SLNM. It is a low molecular weight compound that fluoresces in the near-infrared region (∼800 nm) of the light spectrum and possessed a favorable safety profile with no documented life-threatening side effects. 1 The use of ICG to identify SLNs has become an appealing option due to the absence of radiation and cheaper operating cost than radioisotope.1,8 Nonetheless, ICG mapping is associated with unnecessarily excessive dissection and removal of SLNs. 1 Lack of methodological standardization was also found between studies, thus making it difficult to draw firm conclusions. 1 A focus on the technical aspects and conducting trials with different DTT combinations involving ICG would be substantial to validate the technique and provide arguments for change in practice.
Conclusion
This case presentation of DTT and SPECT/CT for SLNM is the first-ever performed at the east-coast region of Peninsular Malaysia and contains excerpts from our institution’s protocol. The coupling of MBD, 99mTc-nanocolloid, and SPECT/CT improves the management by enhancing SLN detection, increasing surgeons’ interpretative confidence, and minimizing the unnecessary risk associated with radical ALN dissection. We look forward to the collection of more patient data for future SLNM studies.
Footnotes
Acknowledgments
This report was presented as an e-poster at the 31st Annual Scientific Congress of Malaysian Oncological Society (ASCOMOS), 1–3 November 2019, Perak, Malaysia. NT is the recipient of the 2020–2021 USM Graduate Student Financial Assistance (GRA-Assist) sponsorship and the 2020 Fundamental Research Grant Scheme (FRGS) Graduate Assistant Scheme. Finally, the authors would like to acknowledge the contribution of the multidisciplinary team (Dr. Wan Fatihah Wan Sohaimi, Dr. Mohd. Fazrin Mohd. Rohani, Dr. Mohd. Adib Abdul Onny) during the management of the patients and their input throughout the standard-operating-procedure development for Hospital USM.
Author Contributions
All authors managed the patient, and prepared the manuscript, edited, and approved the final draft.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Short-term Research Grant (304/PPSP/6315121) of Universiti Sains Malaysia. The funders had no role in the interpretation or writing of this report.
Ethical approval
The study was approved by the Human Research Ethics Committee of Universiti Sains Malaysia (Reference: USM/JEPeM/17030167), following the Declaration of Helsinki.
Informed consent
The patients were informed that their data would be submitted for publication and gave their written informed consent.