
Abstract
We present an unfortunate case of severe acute aortic regurgitation (AR) following a motor vehicle accident (MVA) linked to isolated aortic valve prolapse, with no evidence of aortic root disruption or other valvular pathology missed on initial presentation. A 55-year-old gentleman, with known hypertension, was brought into the emergency department following a MVA, where he sustained severe intra-thoracic injuries. A bedside transthoracic echocardiogram (TTE) revealed a trileaflet aortic valve with evidence of mal-coaptation and severe AR. A computed tomography angiography of the thorax, however, failed to demonstrate evidence of dissection along the aortic root or ascending aorta. Following successful weaning off ventilatory support, the patient was discharged, but he presented back within a week with worsening dyspnoea and palpitations. Examination and investigation supported a diagnosis of acute heart failure with evident severe AR on repeat TTE. Transoesophageal echocardiography was performed, revealing prolapsed right and non-coronary cusps which were not seen in previous studies but absent evidence of the aortic root, ascending and descending aorta dilatation or dissection. Valvular complications rarely occur following blunt chest wall trauma, often involving right-sided valves due to their proximity to the sternum. Although aortic valve disruption can occur following MVAs, it is often associated with trauma to the aorta. Based on our literature search, there have been only a handful of reported cases of severe acute AR due to isolated prolapse or ruptured aortic valves in the absence of aortic valve perforation, aortic root disruption or dissection and other valvular abnormalities following trauma.
Introduction
Acute aortic regurgitation (AR) commonly occurs in the setting of infective endocarditis, following disruption of the aortic valve coaptation via traumatic and non-traumatic means or following deformation or destruction of the aortic cusps, the aortic root and/or ascending aorta. 1 We present an unfortunate case of severe acute AR following a motor vehicle accident (MVA) linked to isolated aortic valve prolapse, with no evidence of aortic root disruption or other valvular pathology missed on initial presentation which led to dire consequences.
Case presentation
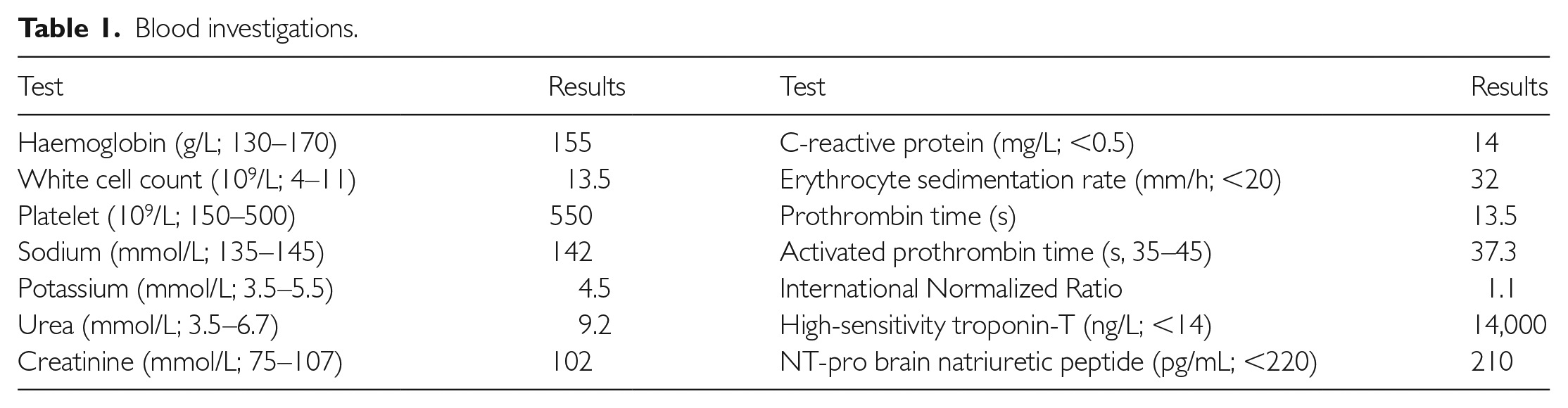
A 55-year-old gentleman, with known hypertension, was brought into the emergency department of a neighbouring trauma centre following a MVA where he sustained severe intra-thoracic injuries. Alongside multiple skeletal injuries, including rib fractures, he suffered bilateral lung contusions (evident from a trauma sequence computed tomography (CT) imaging on arrival) and cardiac contusion (evident from raised high-sensitivity troponin T of 14,000 ng/L). He was intubated and mechanically ventilated during his 21 days in the intensive care unit. A bedside transthoracic echocardiogram (TTE) was performed during his inpatient stay, which reported a normal left ventricular ejection fraction of 57%, normal left ventricular end-diastolic dimension of 30 mm/m2, a trileaflet aortic valve with evidence of mal-coaptation, severe AR on Doppler studies associated with holo-diastolic flow reversal on suprasternal view and no evidence of pericardial effusion (Figure 1). However, the referring team had failed to recognise prolapse of the aortic cusps at the time. Furthermore, due to the nature of his presentation, a CT angiography of the thorax was performed but failed to demonstrate any evidence of dissection along the aortic root or ascending aorta, although the morphology of the aortic cusps could not be best appreciated on this imaging modality. The patient’s history, examination findings and laboratory investigations were not suggestive of infective endocarditis (Table 1). Following successful weaning from mechanical ventilation and oxygen supplementation, the patient was discharged with an outpatient cardiology referral, as he was haemodynamically stable. At the time, his AR was felt to be chronic and likely due to his long-standing hypertension, and he was referred to cardiology services as an outpatient without any inpatient cardiology consult.

Transthoracic echocardiography on apical three-chamber view during (a) systole and (b) and (c) diastole, apical five-chamber view during (d) systole and (e) diastole, demonstrating aortic regurgitation jet on colour flow Doppler, with (f) continuous wave Doppler assessment through the aortic valve revealing a high jet density with measured pressure half time of 180 ms. This is further supported by holo-diastolic flow reversal seen on pulsed wave Doppler imaging down the descending thoracic aorta at the (g) suprasternal view. A parasternal short-axis view, zoomed into the aortic valve during (h) systole and (i) diastole showed malcoaptation between the right and non-coronary cusps. Left ventricular ejection fraction using the Biplane Simpson’s (j)–(k) method demonstrate preserved ejection fraction.
Blood investigations.
Unfortunately, the patient presented within a week to our emergency department with worsening dyspnoea and palpitations. His vitals on arrival include a blood pressure of 102/86 mmHg, pulse rate between 160 and 180 bpm, respiratory rate of 32 breaths per minute and oxygen saturations of 88% on room air requiring oxygen supplementation. On general inspection, there were no dysmorphic features overtly visible. Clinical examination revealed an apex beat in the fifth intercostal space at the midclavicular line and a soft first heart sound with audible third heart sound. There was a low-pitch early diastolic murmur loudest on inspiration (grade 3/6) and pansystolic murmur loudest on expiration (grade 4/6). There were also bilateral crepitations up to the midzone. Chest radiography confirmed both cardiomegaly and pulmonary oedema, and an electrocardiogram on arrival revealed supraventricular tachycardia (Figure 2). Bedside TTE revealed global pericardial effusion and previously reported severe AR on colour Doppler (Figure 3). Following stabilisation, an urgent transoesophageal echocardiography (TOE) was performed, revealing a trileaflet aortic valve with prolapsed right coronary cusp (RCC) and non-coronary cusps (NCC), which were not seen in previous studies, associated with severe AR (Figure 4). There was a 0.5 cm2 area of mal-coaptation noted, but assessment of the aortic root and ascending and descending aorta did not reveal any evidence of dilatation or dissection. Additionally, all other valves were morphologically normal. Subsequently, a cardiothoracic consult was sought, and the patient underwent aortic valve replacement, which confirmed isolated aortic valve prolapse, and he remains well postoperatively.
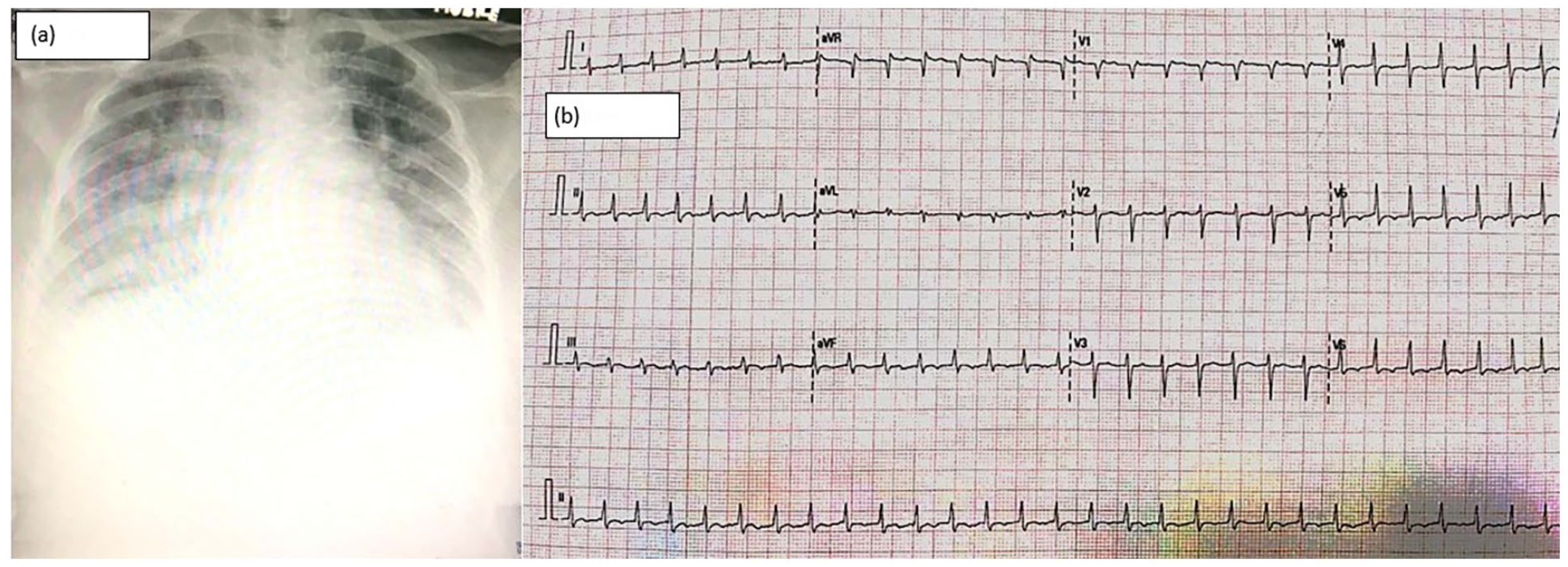
Investigations on arrival including (a) chest radiography demonstrating pulmonary oedema and cardiomegaly, and (b) electrocardiogram showing supraventricular tachycardia with a rapid ventricular rate of approximately 200 bpm.

Bedside transthoracic echocardiography on (a) parasternal short-axis, (b) parasternal long-axis, (c) apical four-chamber and (d) apical five-chamber view demonstrating global pericardial effusion. A large regurgitation jet across the aortic valve in the (d) apical five-chamber view was also seen, likely representing severe aortic regurgitation.

Transoesophageal echocardiography in the (a)–(c) mid-oesophageal five-chamber, (d)–(f) midoesophageal short axis and (g)–(i) mid-oesophageal long axis demonstrating evidence of aortic valve prolapse, specifically of the right and non-coronary cusps, with evidence of severe aortic regurgitation on colour flow Doppler. Assessment at the (j) mid-oesophageal short axis, (g–i) and (k) mid-oesophageal long axis and (l) upper-oesophageal long axis demonstrate no evidence of dissection or dilatation in the ascending and descending thoracic aorta, as well as aortic arch.
Discussion
Valvular complications uncommonly occur following blunt chest wall trauma, where post-mortem reports showed an incidence of 5% for valve lesions after blunt cardiac injury. Aortic valve rupture is the most commonly reported valve injury, followed by the mitral, tricuspid and pulmonary valves.2,3 Although isolated aortic valve disruption can occur following MVAs, it is often associated with trauma to the aorta. Based on our literature search, there have been only a handful of reported cases of severe acute AR due to isolated prolapse or ruptured aortic valves in the absence of aortic valve perforation, aortic root disruption or dissection and other valvular abnormalities following trauma.4–7
During blunt chest trauma, the acute increase in intra-aortic pressure transmitted towards a closed aortic valve, especially during early diastole, can lead to detachment of the valve commissures, leading to prolapsing, tear or rupture of the aortic cusps. The NCC is most frequently affected, as opposed to the RCC and left coronary cusp, as coronary flow to the right and left coronary arteries occurs during diastole, and therefore haemodynamic stress over these cusps decreases. On the other hand, the RCC is the next likely cusp to be injured due to its anterior position, exposing it to higher pressure. 2 All these could potentially lead to acute AR which leads to rapid haemodynamic collapse due to failure of a normal-size left ventricle to adapt to a sudden increase in volume accumulated from both the regurgitation and left atrial flow. 8 The sudden rise in left ventricular end diastolic pressure beyond the left atrial pressure can initially lead to (a) premature closure of the mitral valve, followed by (b) diastolic mitral regurgitation and later (c) raised pulmonary venous pressures – all of which lead to acute pulmonary oedema. There is also an inability for the left ventricle to increase stroke volume in the acute setting, often relying on a compensatory, albeit temporary and inadequate, tachycardia such as the case in our patient. The development of pericardial effusion is also common in the setting of acute pulmonary oedema due to increased hydrostatic pressure, although ruling out the presence of dissection remains paramount. 9
Our case was an unfortunate one which led to dire consequences. Despite the absence of aortic trauma and as clearly illustrated in the existing literature, isolated acute aortic valve prolapse can occur and was indeed evident from the start. Furthermore, the lack of left ventricular morphological changes and normal clinical and laboratory parameters further support the possibility of an acute, non-infective aetiology in our patient. Ideally, three-dimensional TOE could be used to confirm the presence or absence of perforation, but ultimately an urgent cardiology and cardiothoracic surgery consult was already warranted following the trauma and TTE findings.
Conclusion
Although extremely rare, aortic valve prolapse is a potential cause of severe acute AR following trauma. Despite a preserved suspensory apparatus of the aortic valve and ascending aorta, the potential haemodynamic instability following severe AR warrants urgent cardiac assessment and intervention.
Footnotes
Acknowledgements
The authors would like to acknowledge Universiti Teknologi MARA Sungai Buloh for supporting the submission of this case report.
Authors’ contributions
R.E.F.R.S. was responsible for data collection and analysis and for drafting the manuscript. N.J.M., K.S.I., S.S. and M.A.A were responsible for drafting and revision of the manuscript.
Availability of data and materials
The data that support the findings of this study are available from UiTM Sungai Buloh, but restrictions apply to the availability of these data, which were used under license for the current study and so are not publicly available. Data are, however, available from the authors upon reasonable request and with permission of UiTM Sungai Buloh.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Ethical approval to report this case was obtained from Universiti Teknologi MARA (UiTM) Sungai Buloh Ethics Committee.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for his anonymised information to be published in this article.