
Abstract
Study design
Case report series using a using a mixed-methods design.
Introduction
There is a lack of high-quality evidence regarding the efficacy of orthotic intervention compared to standard care to resolve elbow contractures in the early stages after trauma.
Purpose
To present the results of four post-traumatic elbow patients with extension deficits in the subacute rehabilitation phase.
Methods
Four patients met the eligibility criteria and were randomly allocated to a 6-week extension orthotic (Orthotic1-2) or standard care (Control3-4). All participants received 6 weekly therapy sessions which included a standardized home exercise program. Orthotic1-2 received additional extension orthoses which were remoulded each week according to progress. Outcome measures were collected at baseline and final assessment by a blinded assessor including extension AROM and PROM, pain Numeric Rating Scale (NRS), Patient Rated Elbow Evaluation (PREE), Oxford Elbow Scale (OES) and Global Rating of Change (GRC). All participants had their weekly ROM recorded by their treating therapists. Short qualitative interviews were conducted with Orthotic1-2 at the final review.
Results
Plots of extension measures demonstrate participants’ response to the weekly treatments. All participants demonstrated clinically important improvements in extension AROM, extension PROM, OES-Function and GRC scores. Qualitative data on patient factors affecting orthotic use are described.
Discussion
The four cases provide descriptive data on early orthotic intervention and standard care in post-traumatic elbow patients with extension deficits over a 6-week period. While orthotic intervention was well-received, further research with a larger sample size is warranted to explore the role of extension orthoses in traumatic contractures.
Introduction
After elbow trauma, it is common for patients to develop joint stiffness and a loss in elbow range-of-motion (ROM), also known as contracture.1–3 The prevalence of contracture in surgically-managed elbows is 15%, with 57% requiring subsequent release. 3
Elbow contractures can arise from intra-articular or extra-articular structural causes or a combination of both. A heightened pain experience and poor psychological status are associated with the chronicity of contractures.4,5 Increased levels of substance P, mast cells and myofibroblasts in the elbow suggests that a heightened neural drive contributes to a prolonged inflammatory process, resulting in a proliferation of fibrotic tissue particularly in the anterior capsule and surrounding connective tissues.5,6 The likelihood of developing an elbow contracture is dependent on several factors, such as the severity of the injury,3,7 the presence of concomitant fractures and heterotopic ossification. 3 Although elbow contractures can take up to a year to resolve, delayed mobilization and a limited arc of motion as early as 6 weeks post-surgery are associated with permanent contractures.2,3 A limited movement arc is also associated with poorer perceived functional status, 1 impacting work capacity, 8 and sports engagement, 9 thus warranting further treatment to maximize ROM. Extension deficits are more common due to the anterior capsular involvement, hence a suggested goal of rehabilitation is to regain extension mobility within the shortest possible time.10,11 There is likely a greater need for terminal extension in younger patients with for reaching and driving tasks. 12
An elbow rehabilitation program prescribed by specialized hand therapists to restore movement and function can include early active ROM (AROM) exercises,13,14 passive ROM (PROM) exercises,10,13,15 soft tissue releases, 14 passive joint mobilization techniques13,16 strengthening,13,14,17 and orthotic intervention.10,14 A survey on clinical practice in Australia and a modified-Delphi survey in the USA demonstrated that 85%–90% of therapists support orthotic interventions to improve PROM in post-traumatic elbows.10,14 Broadly classified as serial static, static progressive or dynamic, mobilizing orthoses are designed to place the elbow on slight tension to promote growth of soft tissue.18,19 Caution should be exercised as excessive tension can trigger tissue failure, resulting in inflammation, muscle co-contraction, worsening pain and fibrosis. 20 The guiding principle of stress application during therapy is derived from Brand and colleagues who described living tissues’ response to applied stress as occurring in the successive stages of “unfolding , alignment , stiffening and failure”. 18 Mobilizing orthoses are generally favoured over other passive techniques for treating hand and knee contractures as they can be controlled at a low tension more effectively,21–25 and comfortably used overnight to achieve optimal results.26,27 However, there is a lack of published evidence on the effectiveness of mobilizing orthoses for the treatment of elbow contractures, particularly in the subacute phase of recovery. The 2012 randomised controlled trial (RCT) by Lindenhovius and colleagues included post-traumatic elbow participants without movement progression from as early as 4-weeks post-injury to chronic contractures. 28 Both groups received orthotic intervention, using either commercial dynamic or static progressive orthoses. No significant differences in ROM or function were identified between groups. Other studies on elbow orthotic intervention were either on chronic conditions or lacked a comparison group.29–31
This case report series will present the results of four patients with post-traumatic elbow extension deficits in the subacute phase of rehabilitation, with random allocation to a 6-week extension orthotic (OG) or control group (CG). Extension was chosen in this study as the treatment direction of choice as extension deficits are more prevalent in elbow contractures.6,11,17 The custom-made serial static extension orthosis (EO) was chosen as it is considered appropriate for patients in the early stages of healing, 20 comfortable for prolonged use overnight and is the most commonly prescribed design. 10
Methods
This study consists of four single case studies using a mixed-methods design. The participants were recruited to a randomized controlled trial between July 2020 and August 2021 which was discontinued due to implications arising from the Covid-19 pandemic. 32
The four participants with post-traumatic elbow contractures were referred by their orthopaedic specialists for upper limb rehabilitation in a multicentre private practice in southeast Queensland, Australia. Eligibility criteria for the study included: 6–8 weeks post-injury or surgery, an active extension deficit of at least 20°, adequate stability for EO, at least 18 years old and able to provide written informed consent. Exclusion criteria were heterotopic ossification, inflammatory disease, active infection or wound-healing issues, neurological or burns-related contracture, total elbow replacement, complex regional pain syndrome, neck and shoulder/widespread pain syndrome, cognitive impairments, or inability to comply to weekly review and structured rehabilitation. Prior to the study, each participant attended hand therapy once or twice weekly according to their individual needs for wound and scar management, oedema control and ROM exercises. Participants were initially provided with either a resting thermoplastic elbow orthosis or sling which they weaned off by the time of enrolment. None of the participants had received extension orthoses prior to the study commencement. Participants were randomly allocated into OG as Orthotic1 and Orthotic2, or CG as Control3 and Control4.
Outcome measures
Outcomes measures.

pASES-e = Self-report section of the American Shoulder and Elbow Surgeons elbow questionnaire; DASH = Disabilities of the Arm, Shoulder and Hand questionnaire; ES = effect size; SRM = standardised response mean; ICC = intraclass correlation coefficient; SEM = standard error measurement; SDD = smallest detectable difference; PCC = Pearson Correlation Coefficient; MCID = Minimal Clinical Important Difference.
Procedures and intervention
Timeline of participant.
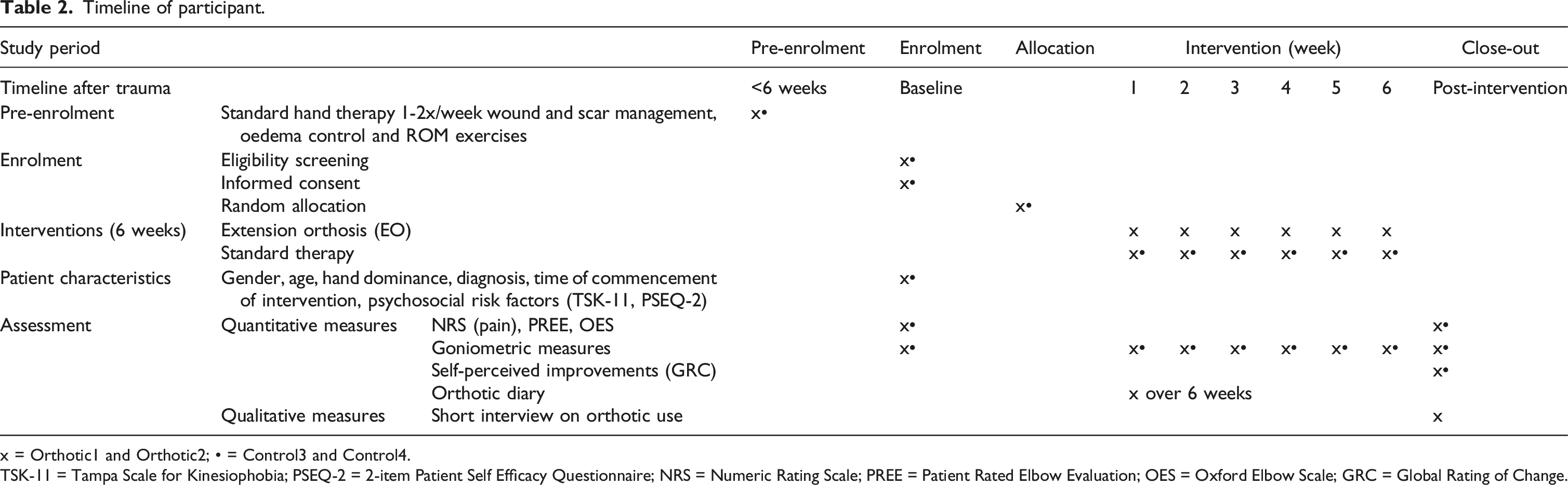
x = Orthotic1 and Orthotic2; • = Control3 and Control4.
TSK-11 = Tampa Scale for Kinesiophobia; PSEQ-2 = 2-item Patient Self Efficacy Questionnaire; NRS = Numeric Rating Scale; PREE = Patient Rated Elbow Evaluation; OES = Oxford Elbow Scale; GRC = Global Rating of Change.
Prior to goniometric assessments, a “preconditioning procedure” involving the application of a heat pack and weighted stretch was used to reduce the effect of confounding variables such as temperature differences or activity levels on joint stiffness.
40
In this study, the blind assessor positioned the participants’ elbows in maximal extension on an elevated platform and applied a heat pack over the volar surface of the elbow for 15 min. After the first 5 min, the participant was asked to hold an additional 500g dumbbell for the remaining duration of heat treatment. The weight was gradually added to reduce muscle guarding and pain (Figure 1). After preconditioning, a universal goniometer was used in a standardized testing position (Figure 2). Preconditioning performed before the goniometric assessment with the patient loosely holding a 500g weight. Standardized testing procedure for elbow goniometric measurements for (a) extension and (b) flexion. Prior to the goniometric assessment, the elbow underwent a 15-min preconditioning procedure. The participant to sit with the back supported against the chair, the upper arm stabilised at 90° shoulder flexion and the forearm in neutral rotation. AROM was recorded with the participant straightening the elbow maximally with their own strength, followed by extension PROM where an extension force was exerted by the assessor, as guided by the participant without eliciting pain.

All participants underwent 6 weekly therapy sessions and seen by their usual treating hand therapist for heat pack application, weighted stretch, effleurage and scar massage. Orthotic1 and Orthotic2 (allocated to OG) were provided with an additional serial static EO (Figure 3) which were custom-made and remoulded by their treating therapists on a weekly basis into greater extension according to progress. The orthotic dosage was a minimum of 6 hours daily, preferably overnight. Both OG and CG participants were instructed in a standardized home exercise program (Table 3). Therapists individualized the protocol, such as adjusting weights used for strengthening and monitored for adverse reactions beyond normal discomfort while wearing the EO or transient pain while performing exercises. To improve participant adherence, all participants were given daily mobile text reminders. Orthotic reports were recorded by participants using a physical diary or virtual diary through TrackActive Pro, an exercise prescription software. Serial Static Extension Orthosis (EO) implemented for Orthotic1 and Orthotic2. Summary of semi-structured home exercise program. AAROM – Active-Assisted Range Of Motion.

Post-intervention, the semi-structured interviews were conducted with OG participants to understand their experiences regarding the use of the extension orthosis such as the motivators and inhibitors to orthotic use, self-perception of orthotic adherence and satisfaction with the intervention. The principal investigator conducted the interviews, which were audio-recorded and took notes of any non-verbal cues.
Data management and analysis
The data were managed in a secure university database (University of Queensland Research Data Manager), according to recommendations made in The Australian Code for the Responsible Conduct of Research and applicable legislation. The data were de-identified for data analysis. Interview recordings were transcribed and de-identified by the principal investigator. Outcome measures were scored by the principal investigator and verified by the co-investigators.
Absolute and percentage gains in goniometric measurements between baseline and final assessment were calculated. The extension AROM is recorded by the treating therapist at the end of each therapy session. The data was plotted graphically to track the participants’ response to the intervention, noting variations in orthotic wear-time. Baseline scores on TSK-11 and PSEQ-2 were calculated for each participant. The 2 items from NRS were averaged and used to calculate the mean difference between the assessments. The OES was scored and analysed using absolute gains. NRS, OES and GRC scores were compared against the minimal clinically important difference (MCID) for meaningful difference post-intervention. PREE data was scored and analysed using absolute gains and percentage differences. Weekly and overall orthotic wear-time was aggregated and averaged over the number of days to generate a patient report detailing the daily orthotic wear-time. Transcriptions of the interviews were analysed by the principal investigator to summarize key experiences associated with orthotic use.
Results
Baseline characteristics of participants.

TSK-11 = Tampa Scale for Kinesiophobia, PSEQ-2 = 2-item Patient Self Efficacy Questionnaire, ORIFs = Open Reduction Internal Fixations, NRS: Numeric Rating Scale; PREE: Patient Rated Elbow Evaluation, with 0–100 for a composite pain and functional score, with 100 for maximum disability; OES: Oxford Elbow Score, were scored 0–100 for each pain, function and psychosocial subcategories, with 0 signifying maximum disability.
aNote. Due to COVID-10 pandemic restrictions, the study enrolment was delayed beyond the 6–8 week timeframe.
bROM measurements were taken with a modified preconditioning procedure.
Elbow Extension ROM as measured in degrees and percentage of gains.

aMeasured under a modified preconditioning condition.
bExtension improvements are beyond the smallest detectable difference (AROM = 6°, PROM = 5°).
Subjective outcome measures.

aMinimal clinical important difference for pain (MCID = 2.17) demonstrated in NRS after 6 weeks.
bMinimal clinical important difference (MCID = 10) demonstrated in OES-Function scores after the 6 weeks.
cMinimal clinical important difference in OES-Pain and OES-Psychosocial scores (MCID = 18) after 6 weeks.
dMeaningful difference in GRC (≥5) after the 6-week intervention.

Therapist plot for weeks 1–6 elbow active extension range of motion.
Patient report of daily orthotic wear-time.

Qualitative data showed that Orthotic1 and Orthotic2 were satisfied with the orthotic intervention and its ongoing use. Both participants reported meeting the minimum requirement for 6 hours daily. Participants described similar motivators of orthotic uptake including perceived effectiveness in improving extension ROM, an achievable orthotic dosage, and an orthotic regime that did not interfere with their normal routine or function. Other motivators included: protection from harm and pain during sleep, reduced disability, personal preference for nighttime orthotic application over intermittent exercises due to the ease of the orthotic routine, muscle soreness from increased orthotic tension was transient and tolerable, recommendations from their expert therapists, and personal goals to return to sports. Individual barriers to orthotic use include reduced patient comfort due to its orthotic design, and the impracticality of the orthosis for daytime use due to it impeding function.
Discussion
The efficacy of orthotic intervention in post-traumatic elbow pathology is not conclusive due to the lack of high-level evidence. To date, there are no known studies that compare the outcomes of orthotic intervention with non-orthotic elbow care. The purpose of this case report series is to present on contracture outcomes of four patients with subacute post-traumatic elbows, who were randomly assigned to receive EO or usual care as part of a 6-week rehabilitation program. We will discuss observations during the elbow-related treatment, and the strengths and limitations of this case series.
As discussed in the introduction, post-traumatic elbow ROM can take up to 1 year to improve. Given that there is anecdotal evidence to support orthotic interventions to improve extension ROM in post-traumatic elbows,10,14 there is a surprising lack of experimental studies with a true control arm without orthoses. There are also no studies to date that document the lived experience of elbow orthotic users. Our case series contributes a detailed description of multiple outcomes from elbow interventions with and without EO, and qualitative feedback to understand the patient factors that can guide orthotic prescription for managing post-traumatic elbow extension deficits.
The present case series has incorporated a control group allocation. Improvements were observed in all patients in the current case series that suggest a true difference occurring as it accounted for goniometric measurement errors (smallest detectable difference for AROM = 6°, PROM = 5°), and achieved meaningful improvements in patient-reported functional outcomes (MCID for OES-Function = 18). 41 However, further research is warranted in larger sample sizes to explore for statistical differences between the orthotic and control groups.
While unable to draw conclusions based on the current data, there are some interesting observations. There may be an effect of orthotic wear time on extension gains. According to the weekly extension records, Orthotic1 reported a rapid improvement in extension upon commencing the extension orthosis, achieving an extension improvement of 5° by week 2 and another 10° by week 3. The daily orthotic wear-time was above 6 hours in the first 2 week but dropped to 4.93 hours daily during the third week. Coinciding with this lapse in adherence to the prescribed regime, extension ROM regressed by 4°. Orthotic2 reported more consistent wear-time and demonstrated improvements in weekly extension ROM that were less variable. The qualitative interviews of Orthotic1 and Orthotic2 showed that the orthotic intervention was well-received and reported acceptable orthotic application times. Participants agreed on the perceived effectiveness of extension orthoses in regaining ROM, coping positively with the recommended dosage of at least 6 hours accumulatively in a day, and satisfaction with the night-time regime. There was minimal negative feedback to orthotic use.
All participants had a GRC sore of +5 and above, signifying a significant improvement in elbow symptoms compared to pre-intervention. A maximal GRC score of +7 was noted in Control4 who had a partial ligamentous injury. This was considered stable and did not require surgery. Conservatively managed elbows often demonstrate greater response to therapy due to reduced risk of soft tissue damage, less swelling and scar adhesions from surgical wounds. Consequently, Control4 achieved a clinically meaningful difference in pain experience as assessed with NRS and OES-Pain, OES-Function and OES-Psychosocial subcategories. Her final extension ROM had improved by 20° actively and 18° passively, indicating that a true change has occurred compared to baseline, resulting in early contracture resolution.
Other studies have reported that the elbow functional outcomes did not correlate with elbow ROM, citing that pain was a stronger indicator of patients’ perceived disability.42–44 At the final review, Orthotic1 reported both self-rated functional scores to be almost negligible (PREE-function 1/50; OES-Function 93.8/100) despite demonstrating a modest gain in active flexion arc of 27°. The overall pain experience was low, with low baseline levels of pain and no significant changes at the final review. Control4 had reported ongoing pain and disability (PREE 21/100; OES-Pain 62.5/100, OES-Function 62.5/100). Her perceived disability could not be attributed to ROM restrictions as a substantial active flexion arc of 48° had been regained. Instead, her pain experience may have contributed to her residual disability. However, it is not known if the extension orthoses are able to modify the pain experience or disability in any phase of healing.
As pain alone accounts for more than a third of elbow disability, Doornberg et al. suggested that clinician-rated elbow evaluation tools should be modified to evaluate pain as a unique component from the objective measures. 44 In this case series, pain was evaluated using NRS, PREE-Pain and OES-Pain subcategories. A notable difference related to the duration of assessment, namely the average pain over 2 days using NRS, 1 week using the PREE-Pain questionnaire, and 4-weeks using the OES-Pain questionnaire. Differences in pain scores may be reflected in Control3, with significant improvements observed using OES-Pain (37.5), while reflecting a deterioration in both NRS (−2) and PREE-Pain (−2). However, changes in NRS did not reach MCID (2.17) and no MCID values are available for PREE interpretation. One of the limitations of this study is that patients were only followed up for a span of 6-weeks. It is not known if differences in pain assessments will be less significant if the study duration was prolonged beyond 12 weeks.
Caution must be exercised when interpreting these results. This series highlights certain limitations to allow for application in clinical practice. One of the limitations is the variability of patient characteristics in this case series. Orthotic1-2 had age differences (60–75 years old) and had late enrolments in the study (9-10.5 weeks), while Control3-4 were younger patients (30–40 years old) and were enrolled earlier (7–7.5 weeks). Even though all 4 cases had lateral elbow injuries and pain, Orthotic1-2 present with more extensive injuries, with surgical repair of a complex terrible triad injury in Orthotic1, while Orthotic2 presented with fracture fixations to the radial head and clavicle. Control4 was the only conservatively managed elbow. Another limitation is in relation to the preconditioning procedure. Control3 was unable to tolerate the full duration of the weighted stretch and may have altered the baseline ROM measurements. The observations from this study suggest consideration of a more appropriate preconditioning procedure to improve the reliability of the measurement, such as removing or reducing the weight applied, while maintaining the duration of heat in a lengthened position. The difficulty lies in finding a standardized tension that soft tissues will be responsive to without triggering pain and muscle guarding. 20 Nonetheless, the strength of this case series is the prospective selection of cases, random allocation, control arm and use of a blind assessor for the outcome measures.
Conclusion
The four case studies provide descriptive data on early orthotic intervention and standard care in post-traumatic elbow patients with extension deficits over a 6-week period. Observations from therapeutic applications, the achievement of minimal clinically important difference in outcome measures, strength and limitations are described. Whilst orthotic intervention was generally well-received, there is currently no clear benefits in improving outcomes in this case series. Further research with a large sample size is warranted to explore the role of extension orthoses in traumatic elbow contractures.
Footnotes
Author contributions
GS, JF and CG were involved in protocol development. GS gained ethical approval and funding. GS wrote the first draft of this article. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the Australian Research Council Scholarship and the Australian Hand Therapy Association. The content is solely the responsibility of the authors and does not necessarily represent the official views of funders. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results. This work had organisational support from EKCO Hand Therapy. Permission for licensed use of TrackActive Pro and Oxford Elbow Score was obtained from Carmel Bain and Oxford University Innovation Limited respectively.
Trial registration
This trial is registered on Australian New Zealand Clinical Trials Registry, (ACTRN12619001402134p).
Ethical statement
Data Availability Statement
The datasets generated and/or analysed during the current study are available from the corresponding author.