
Abstract
Acrodermatitis enteropathica is an uncommon nutritional disorder caused by zinc deficiency, characterised by the triad of periorificial dermatitis, alopecia and diarrhoea. We report an elderly man who presented with periorificial erosive dermatitis, alopecia and systemic manifestations including diarrhea and derangement of liver function.
Introduction
Primary acrodermatitis enteropathica is an autosomal recessively inherited disorder resulting in zinc deficiency. It is caused by a defect of zinc absorption in the gastrointestinal tract. Zinc is an essential co-enzyme involved in various physiological processes, therefore, zinc deficiency may lead to growth retardation, impaired immune function, multiple skin and gastrointestinal manifestations. 1
Case history
A 63-year-old Chinese male nursing home resident was admitted with 10-days history of non-painful rashes over the buttocks, which subsequently progressed to involve the face, upper limbs, lower limbs, and trunk. This was associated with a 3-days history of watery diarrhoea. He also suffers from mild to moderate oropharyngeal dysphagia complicated by poor oral intake. The patient suffered from a previous history of liver cirrhosis, childhood mental disability and frontal lobe epilepsy on long-term carbamazepine, lamotrigine and levetiracetam.
On examination, there were periorbitall crusted erosive plaques affecting the eyes, paranasal and perioral regions (Figure 1). In addition, there were scaly erosive plaques on the anterior neck, distal forearms, distal shins, buttocks, scrotum and groin folds. Nikolsky’s sign was negative throughout all lesions. There was no ocular, oral or genital mucosal involvement. There was non-scarring alopecia affecting the frontal and temporal areas of his scalp. (a & b) Scaly erosive crusted plaques present over the buttocks, perianal, peri-flexural and peri-orifical regions, associated with angular cheilitis and scalp alopecia.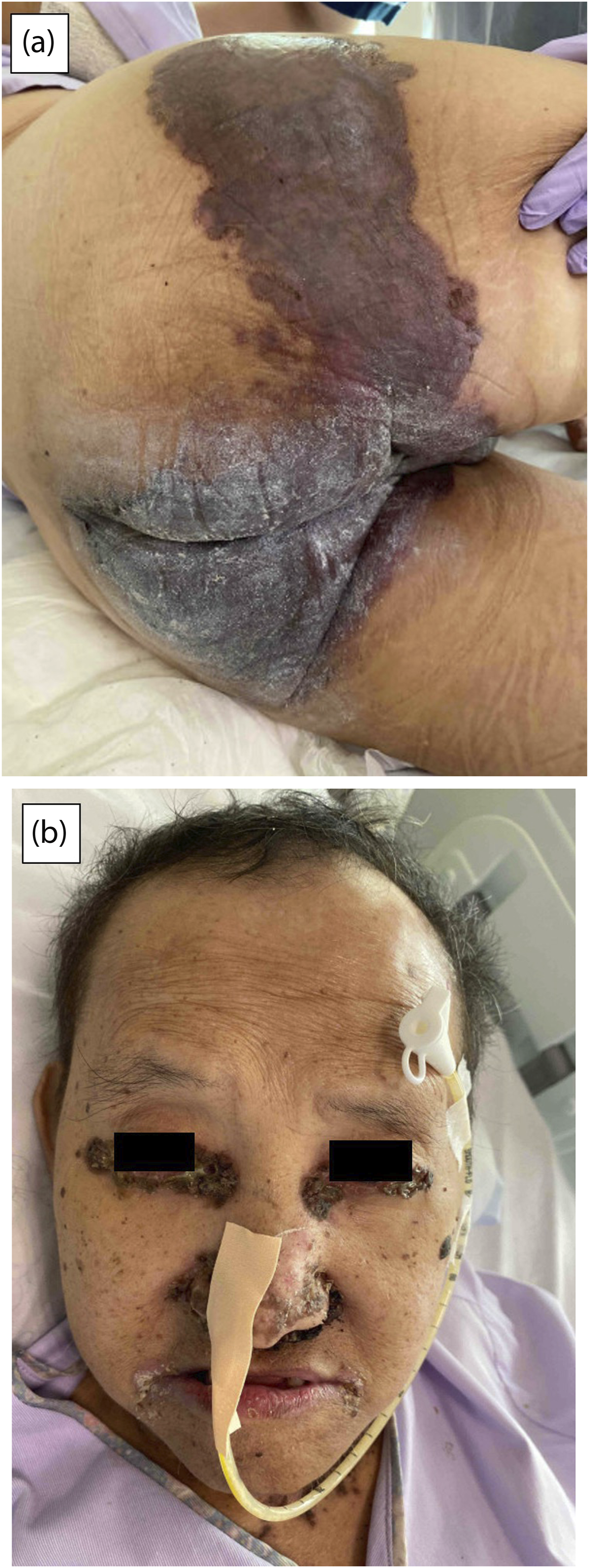
The presence of peri-orifical and peri-flexural erosive dermatosis, alopecia, diarrhoea, accompanied with a history of poor oral intake is suggestive of an underlying nutritional deficiency. However, important differential diagnoses to consider would include Steven’s Johnson Syndrome, staphylococcal scalded skin syndrome, necrolytic migratory erythema, herpes vegetans, langerhans cell histiocytosis and autoimmune blistering diseases such as pemphigus vegetans.
Initial investigations revealed a low alkaline phosphatase (ALP) level (14 U/L), hypoalbuminaemia, hypokalaemia, hypernatremia and hypophosphatemia, related to poor oral intake. A skin punch biopsy performed showed ulceration with thick inflammatory scaly crust containing neutrophils. The adjacent epidermis showed focal basal vacuolaralteration associated with apoptotic cells. There was a dense underlying infiltrate of lymphocytes, histiocytes and neutrophils. There was no frank epidermal necrosis. Direct immunofluorescence was negative. Herpes simplex virus (HSV) PCR swab of his buttock erosions was negative. Anti-desmogleins 1 and 3 were both negative. Subsequent testing confirmed a low plasma zinc level (199.28 ug/L).
Given the clinical findings and investigations, a diagnosis of acrodermatitis enteropathica (AE) was made. Treatment with oral zinc supplementation was commenced at 2 mg/kg per day. Thiamine and vitamin D supplementation were also commenced and a nasogastric tube was inserted to supplement oral intake. Clinical improvement of facial and truncal rashes was noticed as early as 1 week after commencement of zinc replacement (Figure 2) and nutritional supplementation. During his admission, the patient also developed a fever spike, and his urine dipstick test showed pyuria. He was treated for urinary tract infection with oral antibiotics and discharged back to his nursing home on day 15 of admission. A repeat zinc level performed 1 month after commencement of oral supplementation showed serum zinc level was replete (1008 ug/L). Significant clinical improvement was noticeable as early as 1 week after commencement of zinc and nutritional supplementation.
Discussion
Acrodermatitis enteropathica (AE) is a rare nutritional disorder which results from zinc deficiency. Inherited AE is a rare inborn error of metabolism that is seen in infants weaning from breastmilk, caused by SLC39A4 mutation. Acquired AE is cause by inadequate or defective absorption of zinc in the gastrointestinal tract, which can be related to insufficient dietary intake or malabsorption syndromes. In Singapore, inadequate dietary zinc intake is not uncommon and estimated at approximately 14%. 2
The characteristic skin findings in AE includes scaly erythematous plaques, with a predilection for peri-flexural, peri-orificial and acral sites. These plaques can also be eczematous, pustular, vesiculobullous or erosive with crusted border in the periphery. In advanced cases, angular cheilitis, diffuse alopecia, nail changes may be seen. Systemic features include irritability, lethargy, anorexia and neuropsychiatric problems. 3
Zinc is an essential element which plays an important role in immune regulation, growth and development, wound healing, keratinocyte proliferation and differentiation. 4 Zinc deficiency can lead to an impairment of the innate immune system from reduction in NK cell activity, impaired chemotaxis and phagocytosis of neutrophils. Development and function of T cells can also be affected, leading to a defective adaptive immune system. 5
In this case, the presence of an erosive ‘diaper rash’ not responding to topical therapies prompted the consideration of alternative diagnoses. The triad of periorificial, peri-flexural and acral rashes, together with alopecia and diarrhoea, raised the clinical suspicion of acrodermatitis enteropathica. Measurement of plasma zinc level confirms the diagnosis of AE. ALP is a zinc-containing metalloenzyme that is reduced in low plasma zinc level, which serves as a useful surrogate marker of zinc deficiency. Therefore, a low ALP level in this context is helpful in establishing a provisional diagnosis of AE, even before the patient’s plasma zinc level is known.
Stevens Johnson syndrome was considered less likely given the lack of mucosal involvement and the lack of frank epidermal necrosis. The morphology and unique distribution of skin lesions, clinical context, absence of bacteraemia, histology and direct immunofluorescence were not supportive of the diagnoses of staphylococcal scalded skin syndrome, necrolytic migratory erythema nor autoimmune blistering disease respectively.
Impaired immunity in zinc deficiency has been associated with an increased risk of infections, 6 and this may have been a predisposing factor to urinary tract infection in our patient. The presence of liver cirrhosis and hypoalbuminaemia may have contributed to increased alpha-2 macroglobulin production which increases urinary zinc excretion. 7 Zinc absorption from the small intestine is also impaired in patients with liver cirrhosis, 7 possibly leading to zinc deficiency in our patient.
Conclusion
In conclusion, zinc deficiency can present with a myriad of clinical manifestations. It is important for the attending clinician to be cognisant of this under-recognised disorder, in order to establish an early diagnosis and minimise possible systemic complications.
Footnotes
Acknowledgments
The authors would like to thank all clinical staff involved in the care of this patient.
Author contributions
Chee Hoou Loh: Writing-original draft, review & editing, providing clinical care. Adeline Lam Ee Ling: Providing clinical care, review & editing. Yee Kiat Heng: Supervision, writing-review & editing, providing clinical care.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Data availability statement
Relevant de-identified clinical information is available from the corresponding author upon reasonable request.