
Abstract
Introduction
In view of the opioid epidemic and increasing caution surrounding prescription of opioids, addressing the competence of opioid management is important. There is minimal structured opioid education in Singapore. Online opioid education modules are available but lack real-time input, concise objectives, and program evaluation. This pilot online, modular, blended program aimed to efficiently instruct novice doctors on safe and appropriate practical opioid prescribing, optimizing its role in multimodal pain management while minimizing risks to patients and public health.
Methods
The Analysis, Design, Development, Implementation, and Evaluation (ADDIE) model was used. A multidisciplinary team developed the interactive blended program, “Comprehensive Opioid Management in Pain (COMP)”, consisting of three online modules, one case-based discussion (CBD) session, pre- and post-program evaluations. The program was designed to be concise, clinically relevant and engaging to maximize application of knowledge in clinically deficient areas. All junior anesthetists across Singhealth were invited to participate. We analyzed all self-reported and objective scores, as well as program feedback.
Results
33 participants completed the online modules. Despite the moderate to high level of baseline self-reported confidence and competency scores, median scores for all variables increased post-program from pre-program. There was unanimous agreement on the relevance and utility of the training program.
Conclusion
This pilot achieved the aims of improving the knowledge and confidence levels of opioid management in novice doctors. Participants particularly enjoyed the succinct and interactive features of COMP. Further extension with modules focusing on opioid diversion and its use in high-risk populations would benefit intermediate learners.
Introduction
Pain causes suffering and timely intervention is crucial and humanitarian. Opioid epidemics worldwide have resulted in physicians being reluctant to prescribe opioids, which may result in under-treatment of pain.1,2
Increasing recognition of this problem has led to recent introductions of online opioid education modules. While many integrate interactive online features to engage participants in active learning, there are three main areas which are lacking in current available modules. Firstly, many modules lack clear curriculum,3,4 perhaps due to the complexity of opioid management. Secondly, real-time input which has been recommended for effective online learning 5 is mostly unavailable. Thirdly, many modules evaluate their impact on clinical knowledge and confidence in opioid management, but none evaluates the user interface to assess user-friendliness.
The authors believe an interactive online modular blended learning program with real-time input that is structured, concise, clinically relevant and engaging can improve clinical application of knowledge. The primary aim was to consistently equip novice doctors with safe and appropriate opioid prescribing skills, optimizing opioids in multimodal pain management while preventing abuse and diversion. The secondary aim was to determine the program’s effectiveness and potential for expansion to all opioid prescribers. The ultimate goal was to develop a standard of accreditation for safe opioid prescription.
Methods
We used the Analysis, Design, Development, Implementation, and Evaluation (ADDIE) model, which is an instructional design framework established for course development. 6 As opioid management domains are varied and complex, it provides a structured approach to distill our program objectives, target deficient areas and evaluate our program to see if these objectives were met.
Needs analysis
Needs analysis was performed by gathering targeted feedback regarding opioid management problems from interviewing doctors, nurses, and pharmacists. Amongst feedback and anonymous Risk Management System opioid-related cases, deficiencies in opioid prescribing and administration practical skills were highlighted (e.g., wrong opioid route, inappropriate use of concurrent opioids). Subsequently, 58 junior and 65 senior anesthetists surveyed 7 revealed only 57.8% felt confident in prescribing opioids and only 35% advocated a multidisciplinary team approach for complex pain patients. The majority (96.7%) believed they would benefit from pain management education.
Design and development of the program
A multidisciplinary team encompassing pain physicians, anesthetists, nurses, and pharmacists involved in pain management was gathered. Targeting issues identified through the needs analysis, the authors developed a program emphasizing key components of: (1) skills to address pain early and safely, (2) appropriate opioids use and when to escalate to a specialist pain physician, and (3) preventing unsafe opioid prescribing practices which can result in harm, opioid abuse, and diversion.
Module title, objectives, contents, and assessments.

*Modules 4 and 5 were planned to be potential extensions to the pilot program.

Interactive interface with clinical decision making (Example 1: choose yes/no according to question).

Interactive interface to assimilate clinical knowledge and management (Example 2: matching exercise of opioid side effects/overdose to management steps. Matched example “respiratory” and “cardiovascular” done).
Implementation
This program was tested by the project team and selected juniors, then further refined prior to implementation. All juniors in the departments of anesthesiology across Singhealth cluster were invited to participate. An ethical approval waiver was obtained from the Singhealth Institutional Review Board.
Evaluations
The program evaluation consisted of three components including (1) pre- and post-program MCQs on theoretical opioid knowledge and its clinical application, (2) self-reported pre- and post-program confidence and competency in handling opioids, and (3) program evaluation on its content, structure, delivery, and relevance. Likert scales were used. To allow fair comparison, the team ranked the MCQs in terms of difficulty and categorized them based on the concept tested; these were then evenly distributed between the pre- and post-evaluations.
Evaluation data was extracted by the project team’s administrator and anonymized before sending it to the team for analysis. Descriptive statistical analysis and Wilcoxon Signed-Rank Test was conducted. To account for Type I error inflation due to multiple comparisons, Bonferroni correction (17) was applied with a new statistical significance threshold p-value of 0.002 instead of the conventional 0.05.
Results
Participant characteristics
Participant profile (N = 33).
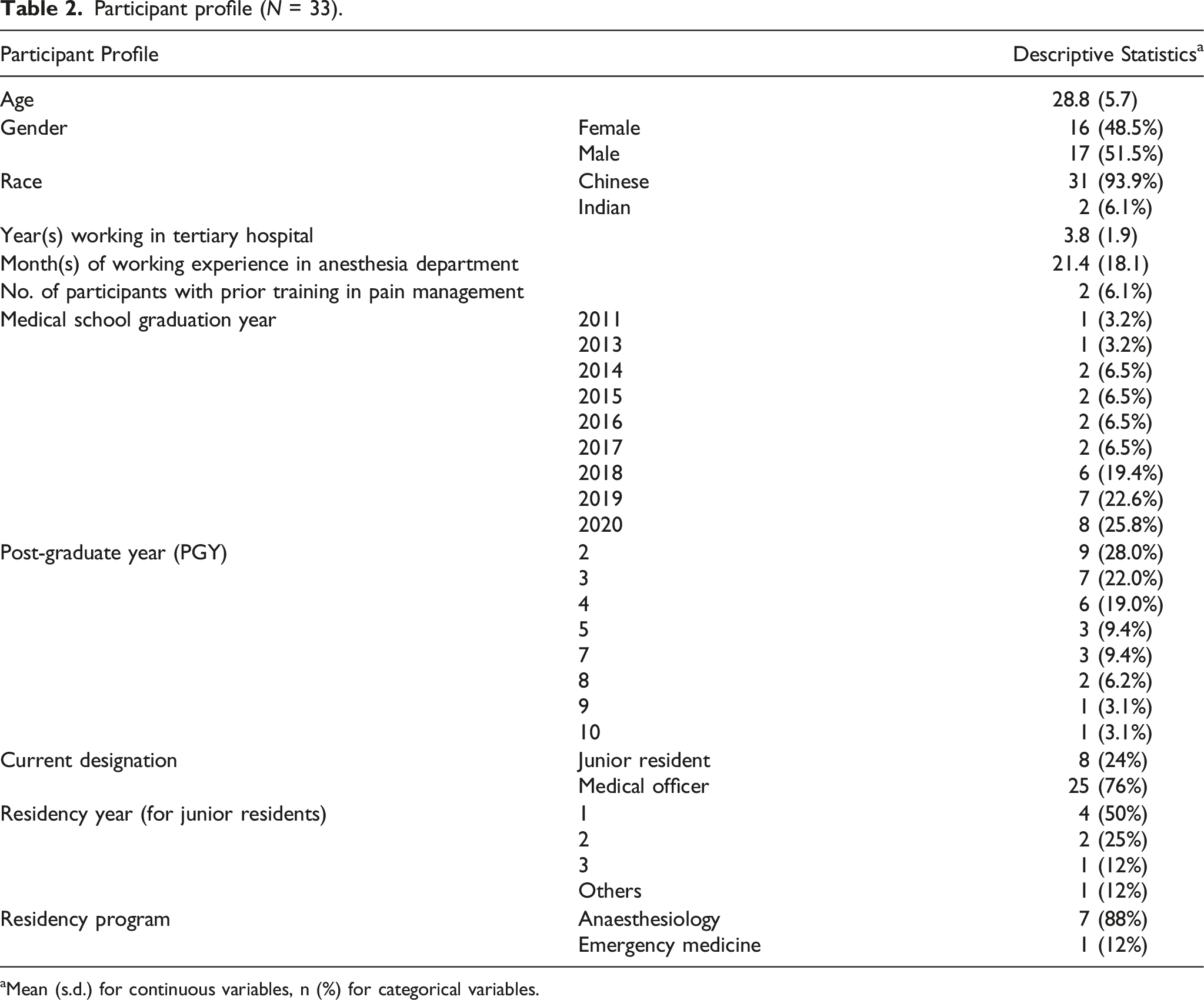
aMean (s.d.) for continuous variables, n (%) for categorical variables.
Self-reported confidence and competency in opioid pain management
Descriptive statistics of self-reported and confidence and competency and objectively assessed competency levels in pain management before and after the training program.

aNumber of valid responses, list-wise deletion applied.
bMedian (Range).
Wilcoxon signed-rank test of self-reported confidence and competency and objectively assessed competency levels in pain management before and after training.
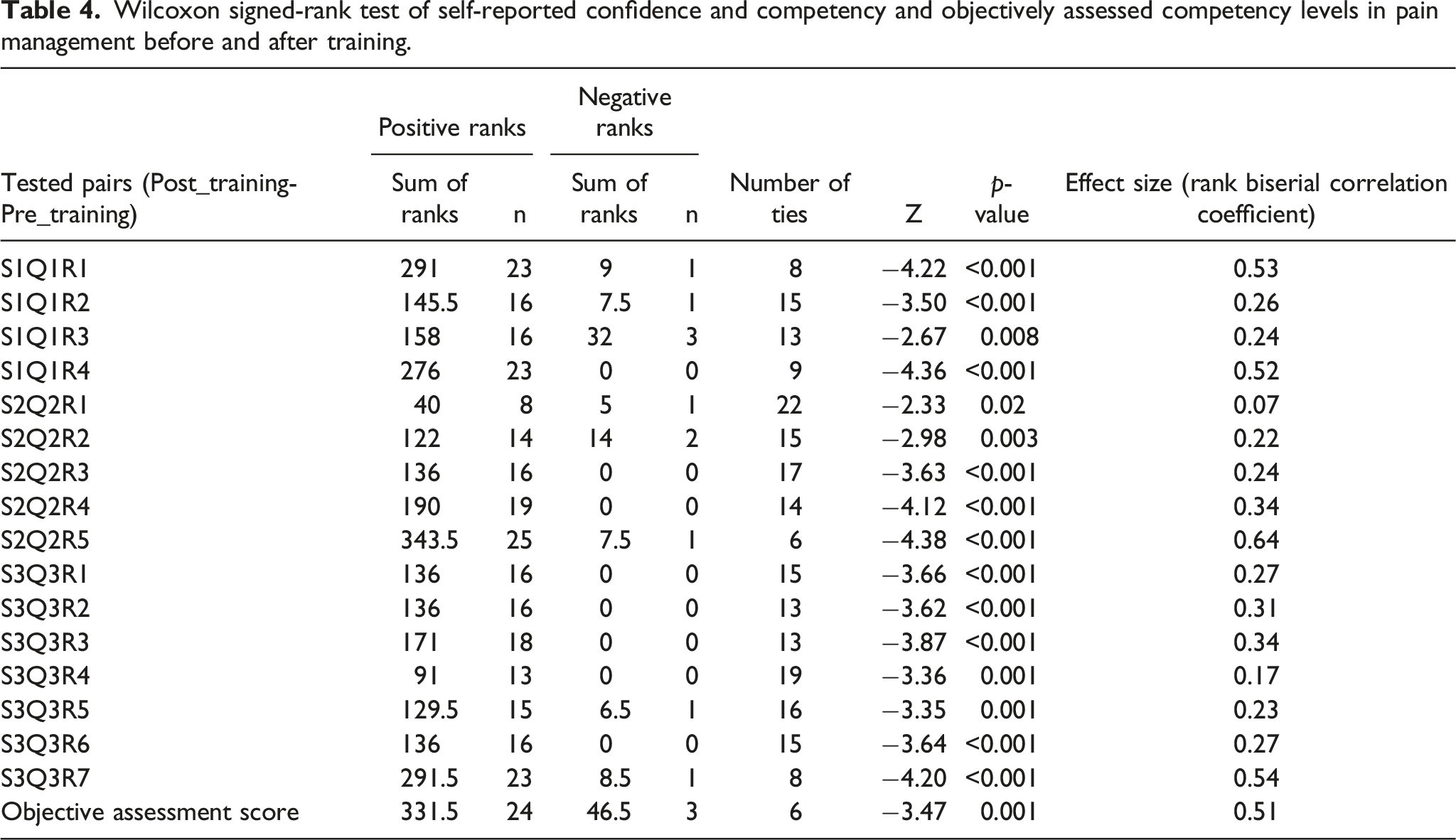
Based on the effect size statistics, the difference was most pronounced for “confidence in assessing patients using a biopsychosocial approach (S1Q1R1)”, “choosing appropriate opioid for various patient groups (S1Q1R4)”, “ability to formulate a management plan for the opioid-dependent patient coming for surgery (S2Q2R5)”, and “to identify withdrawal symptoms in opioid dependent patients when opioids are withheld from them (S3Q3R7)”.
Objectively assessed competency in opioid pain management
The median objectively assessed pre-program competency score was high at six out of 8. Post-program, this rose to seven and had a smaller range. The difference was statistically significant.
Program feedback
Overall, all aspects of the program were highly positively rated (Figure 3). There was unanimous agreement on the relevance, utility, content, and duration of the training program. 84% of participants found the CBD session’s interactivity helpful. Besides two participants who felt some interactive components could be simplified, there was no negative feedback. Likert Chart of post-program feedback.
Discussion
There is a lack of formal pain management and opioid education internationally, with various educational studies recognizing a need in this area.8–10
With pain management being an anesthesiology sub-specialty in Singapore, structured pain education mostly comprises trainee lectures on pain management. Pain management education is largely obtained “on-the-job” and highly variable. Singapore recently released opioid guidelines in 2021, 11 but guidelines alone are inadequate to translate knowledge into clinically appropriate and confident opioid management.12,13 Establishing a structured pain management program with focus on clinical practice and opioids can improve patient safety and care.
Besides an interactive online platform which is widely accessible, the authors wanted to create a program that was time-efficient and yet had maximal impact. This would require streamlined and clear objectives aimed at the most deficient areas in the current practice. This was achieved via the needs analysis survey and rigorous discussion amongst the multidisciplinary team. The content needed to be highly concise, and presentation had to be clear and clinically relevant for knowledge assimilation. We aimed to have participants spend less than 30min per module to ensure continued engagement and retention of knowledge. Pre- and post-module quizzes with immediate feedback aimed to consolidate the learning objectives for participants.
Our participants were junior doctors with inpatient pain management experience and moderate to high level of pre-program self-reported confidence and competency scores. It was heartening to still see improvements in both objective and self-rated scores throughout, with the greatest effect size improvements corresponding to the areas of need highlighted from the needs analysis: biopsychosocial approach of managing pain, choosing appropriate opioids for patients, and identification of withdrawal symptoms (Table 3).
Given the lack of student-teacher interaction in available modules, the authors strove to increase learning effectiveness by creating a blended program with CBD facilitated by our multidisciplinary team. Although 84% of participants found the CBD session’s interactivity helpful, the authors encountered difficulties in obtaining a common protected time for participants and facilitators. It was also labor intensive involving at least four faculty members each session. Weighing the potential benefits and challenges, the authors will replace this with an online forum for future sessions.
The authors sought to assess the participants’ learning experience as it is shown to correlate with skills improvement. 14 COMP program was very well received with unanimous agreement on its utility and relevance. Interactivity, conciseness, and clinical relevance of the program was most appreciated, allowing retention, understanding and application of knowledge obtained as evidenced by increased scores in all areas assessed. Some interactive components could be more guided to be more user-friendly.
Our main limitations are the low participant numbers and varied clinical experience amongst our participants. Unfortunately, due to the COVID epidemic and reallocation of medical manpower resources, we had limited junior manpower allocated to the anesthesia departments. The increased workload due to fewer juniors also discouraged many from signing up voluntarily for an extra program and barred a few from attending the CBD sessions. Due to frequent department out-rotation of juniors and approximately 50% participation rate, it was not possible unable to assess direct clinical impact of COMP with reported RMS opioid incidents which was initially intended.
Conclusion
Based on the positive results and feedback, the authors believe the aims of the program have been achieved. The participants enjoyed the program and were more confident with safe and appropriate opioid prescribing. To improve COMP, CBD will be replaced with an interactive discussion forum. Two more modules focusing on opioid diversion and its use in a high-risk population will be launched. With the expansion, COMP may benefit intermediate practitioners instead of just novice doctors involved in pain management. Further analysis of feedback from the final program would allow us to determine the feasibility of using it as an accreditation tool, facilitating safe and timely opioid prescribing practices for all.
Footnotes
Acknowledgments
We would like to acknowledge Ms Hong Yu Wen (Pharmacist, Singapore General Hospital) for contributing to our online modules and CBD; Dr Denise Quah (Resident, Singhealth) for assisting with the needs-based analysis; Ms Daphne Chan and Mr Joseph Pu (eLearning Singhealth) for their invaluable help with IT and formulating the interactive online program; Ms Carol Tan and Ms Christine Neoh (Anaesthesiology Academic Clinical Program Administrators, Singhealth Duke-NUS) for coordinating all our administrative needs; Ms Xin Xiaohui and Ms Nur Nasyitah Binte Mohamed Salim (Health Services Research Unit, Singapore General Hospital) for performing and giving us advice on the data analysis for this project.
Author contributions
Leong XYA: conceptualization, design, IRB and grant application, study materials, recruitment, implementation, data collection, data analysis, manuscript writing and revision Lim ZW: IRB and grant application, study materials, recruitment, implementation, manuscript writing Li LW: study materials, recruitment, implementation George JM: conceptualization, design, implementation, mentoring; Goy RWL: conceptualization, design, mentoring Chan DXH: IRB and grant application, needs analysis, study materials Tan SYL: study materials Tan PY: needs analysis, study materials Yu XJ: design, IRB and grant application, study materials, recruitment, implantation, manuscript revision, mentoring.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the Singhealth Duke-NUS Anaesthesiology and Perioperative Sciences Academic Clinical Program Philanthropy Grant 2020.
Ethical statement
Data Availability Statement
Data and materials are available upon request to the authors.