
Abstract
Introduction:
Continuous epidural analgesia has proven to be a good tool in the anaesthetist’s quest to provide excellent pain relief for an extended perioperative period. Pharmaceutical advances provide us with a larger array of both local anaesthetic (LA) drugs and additives that can prolong the duration or enhance the quality of analgesia, or both. The avoidance of LA toxicity is of paramount importance for safe prescription, especially in the high-risk neonatal and infant cohort, and all patients stand to benefit from ‘safer’ LA agents and adjuvants that promote the use of a lowered concentration of epidural LA infusions. We present a descriptive review of trends in epidural prescription and technique in our hospital.
Methods:
Our observational study was conducted over a period of 19 years in a tertiary paediatric teaching hospital. Prospectively collected data that included patient demographics, level of epidural catheter insertion, LA drugs and adjuvants used, as well as postoperative infusion rates, were then analysed retrospectively.
Results:
There was a decline in the use of paediatric epidural analgesia. Over the study period, we also observed a shift in preference of LAs and adjuvant drugs toward safer alternatives.
Conclusion:
Paediatric epidural analgesia is gradually being superseded by other analgesic modalities with superior safety profiles (e.g. peripheral neural blockade). However, indications remain for its continued use, and anaesthetists should be familiar with its technical aspects and pitfalls.
Introduction
Epidural analgesia is a well-established method of intraoperative and postoperative pain relief in the paediatric population. In the last two decades, a rise in the popularity and use of other analgesic modalities have displaced it as the preferred regional analgesic technique of choice in the postoperative period.
This study aims to examine the practice and trends in the use of epidural analgesia in a Singaporean paediatric population over the last 19 years. We illustrate the changes in epidural drugs and practices over time, and discuss their benefits and risks. Finally, we discuss the possible factors leading to the decline of paediatric epidural anaesthesia, as well as highlight new fields of development of alternative modalities of paediatric analgesia in our Pain Service.
Methods
Since 1997, prospectively collected data on all epidural catheters inserted have been recorded on our Acute Pain Service (APS) audit forms. These data encompassed patient demographics, surgery performed, level of epidural catheter insertion, local anaesthetic (LA) drugs and adjuvants used, epidural infusion rates as well as any other analgesic prescriptions, together with daily pain scores and documentation of any adverse effects encountered.
Approval for this observational study was obtained from the institutional review board. A retrospective review of the above data was conducted to examine the trends and changes in practice over the last 19 years. All children who received epidural catheters from 1 June 1997 to 31 May 2016 were included in the study. These included thoracic, lumbar, trans-sacral and caudal epidural catheters. Single-shot caudal epidurals were not included. Patients were divided into the following age groups: neonates <28 days old; infants <1 year old, toddlers 1–2 years of age, preschoolers 3–6 years of age, children 7–12 years of age and adolescents >12 years of age.
Results
A total of 829 epidural catheters were inserted from 1 June 1997 to 31 May 2016, accounting for 0.6% of all anaesthetics (Table 1). Figures 1 and 2 illustrate an overall declining trend in the use of epidural analgesia over the last 19 years; in particular, a steep drop is seen after 2001. The incidence of epidural analgesia has remained largely unchanged in the last 10 years.
Trends in level of epidurals with time.
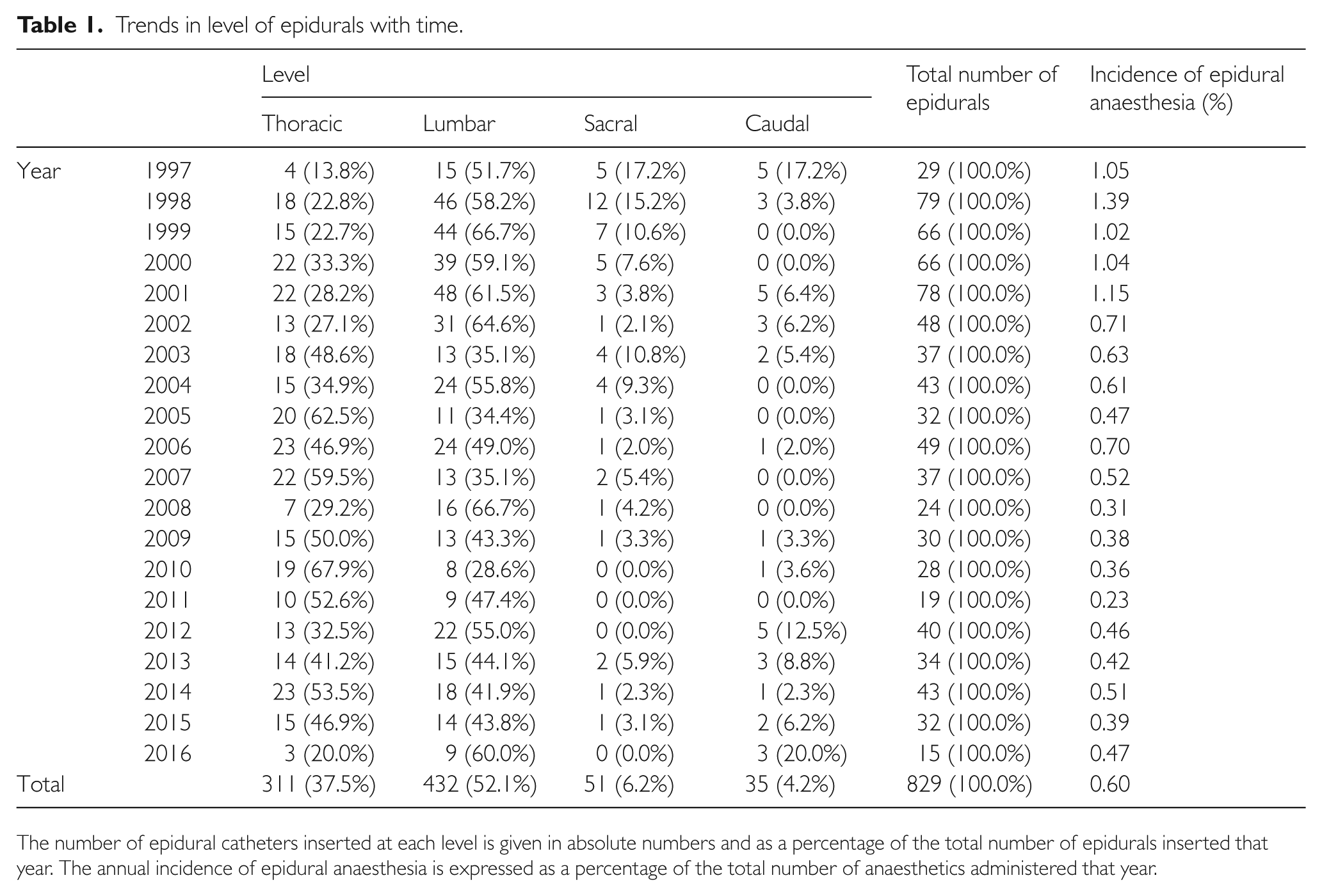
The number of epidural catheters inserted at each level is given in absolute numbers and as a percentage of the total number of epidurals inserted that year. The annual incidence of epidural anaesthesia is expressed as a percentage of the total number of anaesthetics administered that year.

Incidence of epidural anaesthesia from 1997 to 2016 at a paediatric teaching hospital in Singapore (expressed as a percentage of total anaesthetics performed).

Trends and approaches in paediatric epidurals from 1 June 1997 to 31 May 2016 in a paediatric teaching hospital in Singapore.
The majority of epidural catheters are inserted at thoraco-lumbar levels (Figure 2). The first seven years saw a gradual rise in the incidence of thoracic epidurals and a decline in lumbar epidurals (Figure 3). Caudal catheters have also been on the decline. Children younger than 3 years of age saw the largest decline in trans-sacral epidurals.

Trends in levels of epidurals over time.
Figure 4 illustrates an overall rise in the use of epidural analgesia in infants and adolescents, and a corresponding fall in preschoolers as well as children in the school-going age group.

Trends in age group over time.
The proportion of caudal catheters used was higher in neonates compared to the older age groups (Table 2). Conversely, the use of thoracic epidurals was less common in neonates.
Level of epidurals performed in each age group.

Figures 5 and 6 illustrate trends in the drugs given via continuous epidural infusion. Levo-bupivacaine was introduced in our institution in 2012, and since then there has been a steady rise in the use of levo-bupivacaine instead of racemic bupivacaine. The use of adjuvants has also changed over the years – there has been a shift away from using additives at all. Opioids are used less frequently, with a fall in the use of fentanyl by almost half in the last decade and the complete avoidance of morphine since 2012. Clonidine has also been used more frequently in the last 10 years.

Trends in local anaesthetic drugs used in epidural infusions.

Trends in adjuvant drugs used in epidural infusions.
Over the years, the midline approach has been favoured over the paramedian approach, consistently accounting for over 80% of all epidurals. Epidural catheters were left in situ for a mean of 2.3 days (95% confidence interval 2.2–2.4 days), with an initial rise in mean duration (from 1.7 to 2.8 days) in the first decade and a plateau thereafter at about 2.4 days.
Discussion
The overall incidence of epidural analgesia is 0.6%, which is low compared to an incidence of 5.1% in the French-Language Society of Paediatric Anaesthesiologists (ADARPEF) study. 1 Parental fears of potential neurological complications are not uncommonly encountered and preclude more frequent use of epidural analgesia. Concerns of intraoperative coagulopathy, particularly where massive blood transfusion is anticipated or potential derangements in coagulation (e.g. with significant hepato-biliary disease) may sway the anaesthetist and/or surgeon to view it as a riskier rather than a beneficial option. Further study on the perception of Asian parents as well as anaesthetists about the safety of epidurals may shed light on this issue. Because of our stringent and cautious patient selection, we have encountered only one case of postoperatively deranged coagulation requiring further labs and delay in removal of the catheter.
The use of epidural analgesia has fallen steadily over the last 19 years, from 1.05% in 1997 to 0.47% of all anaesthetics performed in 2016. This is consistent with international data,1–3 which also showed a decline in the use of epidural analgesia. It is also in keeping with the rise in popularity of use of other modalities of analgesia including patient-controlled analgesia, caudal additives and peripheral regional anaesthesia. 1 At the same time, the development of laparoscopic surgery has reduced analgesic requirement in many surgeries.3,4
A fall in the absolute number of lumbar and trans-sacral epidurals was seen after 2008, when anaesthetists began using additives in single-shot caudal injections. Clonidine and S-ketamine were frequently used, and the prolonged duration of effect provided good analgesia of sufficient duration such that an indwelling epidural catheter would not be required.5–7
Over the last decade, there has been increasing global interest in paediatric regional anaesthesia.1–3 The ADARPEF study in 20101 showed that peripheral nerve blocks represented 66% of all regional anaesthesia, compared to only 38% in 1996. 2 With the increase in popularity of regional anaesthesia since 2008, an increasing number of lower limb peripheral nerve blocks such as femoral nerve blocks have also allowed anaesthetists to avoid the use of lumbar epidural catheters and their inherent risks. This is especially so with the increasing skill in the use of ultrasound techniques in regional anaesthesia, 8 which may allow the use of a lower volume of LA and prolong the analgesic effect compared to conventional peripheral nerve block techniques. 9 Peripheral catheter techniques also allow continued postoperative analgesia 10 and have a superior safety profile compared to central neuraxial blocks. 1
In recent years, truncal blocks such as paravertebral blocks, transverses abdominis plane blocks and rectus sheath blocks have also increased in number. These have the potential to decrease postoperative pain and therefore reduce the need for thoracic epidural infusions. 11
Patient-controlled analgesia has been established as a safe and reliable method of postoperative analgesia in children who are able to understand its use. Nurse-controlled analgesia, in the presence of reliable protocols, are also safe and provide an effective analgesia, 12 sparing the patient an invasive epidural catheter insertion. In our institution, the use of patient-controlled analgesia has tripled in the last decade (from 0.6% in 2006 to 1.8% in 2016), and may have accounted for the decline in the use of epidural catheters in school-going children and preschoolers, respectively.
Trends in prescription
(i) LA agents
Bupivacaine has traditionally been the local anaesthetic of choice in continuous epidural infusions. However, the last five years have seen the introduction and rise in use of levo-bupivacaine at our hospital. Levo-bupivacaine has similar analgesic efficacy but a lower risk of toxicity (viz. neurotoxicity and cardiotoxicity) when compared to racemic bupivacaine. This attested superior safety profile makes it more ideal for paediatric use. 13 Epidural ropivacaine remains less popular than bupivacaine or levo-bupivacaine, a trend mirroring that of caudal analgesia, where the latter two were used 85% of the time, 14 largely due to prevalent paediatric anaesthetists’ preference.
(ii) Epidural opiates
In our institution, the standard epidural opiate additive of choice is fentanyl at concentration of 2 mcg per ml in the epidural infusate. It is entirely omitted in neonates and younger infants. Epidural morphine has been used as a substitute for hydromorphone, which is the more commonly used epidural opiate in the United States of America. The hydrophilic nature of morphine produces more extensive spread which results in an improvement in the quality of analgesia. 15 It is particularly useful in cases with inadequate dermatomal coverage or where its more pronounced sedative effects may be useful in postoperative care of the fractious child. However, it is mandatory to document with absolute confidence that the epidural is in fact in the correct place (i.e. the epidural space) before utilising this prescription. It also presents a relative contraindication to the addition of a second parenteral opioid, especially as a continuous infusion that is commonly utilised in younger children, in view of the unpredictable nature of delayed respiratory depression (up to 17 hours after administration) associated with epidural morphine. 15
(iii) Epidural clonidine
Clonidine is known to prolong the duration of epidural analgesia without significantly increasing the risk of adverse effects, 16 and its popularity has superseded that of morphine. There has been an overall decline in the use of opioid adjuvants, in keeping with international practices on caudal additives. The addition of caudal fentanyl in particular has not been shown to enhance analgesia compared to ropivacaine alone. 17 Unlike hydrophilic morphine, its lipophilic nature may not be as useful in augmenting the analgesic effects of incomplete blocks.
(iv) Epidural ketamine
Ketamine has been reported to decrease analgesic requirements 18 and prolong the duration of caudal epidural analgesia to over six hours. 19 As a single-shot caudal additive at the recommended dose of 0.5 mg/kg, it has provided prolonged analgesia for up to 22 hours with minimum behavioural anomalies and agitation. 20 Although epidural morphine has been demonstrated by several authors to provide more potent analgesic and sedating effects than epidural ketamine, Xie et al. managed to show that the addition of epidural ketamine provided superior analgesic effects. 21 Adverse neurological effects have been documented after neuraxially administered, non-preservative-free ketamine and in our institution, only preservative-free S+ ketamine can be administered in neuraxial blocks. In the recent light of neurotoxicity of anaesthetic agents, we have chosen to be more conservative with its use, limiting its prescription to single-shot caudals for its prolonged analgesic effect in older children, rather than as an additive in a continuously administered epidural infusion in our younger subset.
(v) Other epidural adjuvants
Neostigmine and midazolam have not been employed as epidural additives in our hospital. Reports of their successful utilisation in the caudal/epidural space have been documented in other countries.19,22 We collectively chose not to try out these drugs because they are inherently not analgesics per se and more importantly because we have not been able to procure a pharmaceutical preparation safe for use in the epidural space. It is possible that their analgesic advantage is largely due to sedation and musculoskeletal relaxation, rather than manipulation of innate opioid receptors or other established analgesic pathways.
(vi) Patient-controlled epidural analgesia (PCEA)
In our practice, continuously administered epidural LA with or without additives has provided good analgesia (with pain score less than 2/10) in the majority of cases so we had little impetus to explore PCEA. An additional concern is that PCEA boluses may lead to a block level that is potentially higher than desired. This mandates more intensive assessments and monitoring, particularly when already faced with difficulties in the accurate measurement of pain in young children. With continued development and increased sophistication of epidural programming via the pump and cartridges used, we can currently explore this modality, which is already a useful tool for paediatric spinal surgery. 23
Future directions
The future of paediatric epidural analgesia remains uncertain for now. The development of liposomal local anaesthetic deposits which can be administered aseptically by surgeons may herald a further decline in the number of elective epidurals. The potential for future additives or long-acting local anaesthetic agents to extend the duration of a single shot regional to the point that the need for a postoperative infusion is obviated, may do away with the need for an indwelling catheter and its consequent associated risks. Although the use of epidural analgesia is on the decline, it still remains an effective technique for management of acute postoperative pain. Currently, there remain indications for the use of epidural analgesia in specific instances such as open thoracic surgery, 4 major intra-abdominal surgery 24 or spinal surgery 25 where the analgesia effected is virtually sine qua non for those either unfamiliar with newer regional techniques or without the availability of ultrasound machines to guide them in, for example, paravertebral or transversus abdominus plane (TAP) blocks. Anaesthetists should maintain competency in the insertion of paediatric epidural catheters, but as the overall incidence decreases, there will be fewer opportunities for training and refinement of skills, sauf in vitro simulators. In our practice, due to the small numbers of infant epidural catheters performed, we preferentially reserve their execution in this higher-risk group for paediatric specialist consultants only. Clearly, it is imprudent to allow a trainee who has not performed enough epidurals in older children to attempt this challenging and delicate task. Similarly, clinical nursing skills and expertise in managing the paediatric epidural may deteriorate with infrequent epidural patients to manage, giving rise to concerns regarding postoperative management of continuous epidural infusions and subsequent identification and management of any adverse effects. Our institution has guidelines in place for the initiation and care of epidurals, encompassing protocols on paper and electronic order templates to guide junior staff who may be unfamiliar with its use. This is in addition to core training, didactic lectures and supervision. We also mandate ongoing accreditation for nurses in their competency skill sets in handling paediatric epidurals, which embraces lectures, practical as well as test/assessment aspects.
Strengths and limitations
This is the first such study which has examined trends from a single database over a period of almost two decades. It mirrors a global trend in paediatric anaesthetic practice and highlights potential areas for development in paediatric analgesia. We acknowledge our main limitations as that of modest numbers and that this study examines only patients from a single institution.
Conclusion
Over the last 19 years, the use of epidural analgesia has been on the decline as it is gradually replaced by alternative modalities of analgesia with superior safety profiles. In keeping with global trends, we expect further growth in the area of paediatric regional anaesthesia in the near future, specifically in the fields of peripheral nerve and truncal nerve blocks. However, there remain clear indications for the use of epidural analgesia in children, and for this reason paediatric anaesthetists must retain competency and confidence in its use.
Footnotes
Acknowledgements
The work for this original article was conducted at KK Women’s and Children’s Hospital, Singapore. Both authors were involved in study design, data collection, statistical analysis and preparation of the manuscript.
Declaration of Conflicting Interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.