
Abstract
Objectives:
To investigate the prevalence of skeletal Classes I, II and III in a Chinese orthodontic population, and determine its association with the prevalence of dental anomalies.
Methods:
This retrospective cross-sectional study was conducted on 2508 ethnic Chinese orthodontic patients aged 14 to 25 years who attended the Department of Orthodontics at the National Dental Centre Singapore. Radiographs, photographs and clinical records of the study sample were examined for the prevalence of dental anomalies in the permanent dentition, excluding third molars. The anteroposterior skeletal relationship was determined based on the A point–Nasion–B point angle measured from the lateral cephalogram, whereby Class I: A point–Nasion–B point = 3.6° ± 2.5° (1 standard deviation) that is 1.1° to 6.1°; Class II: A point–Nasion–B point greater than 6.1°; Class III: A point–Nasion–B point less than 1.1°. Logistic regression was used to determine the association between the anteroposterior skeletal relationship and the occurrence of various dental anomalies.
Results:
The prevalence of the anteroposterior skeletal relationship was: 49.5% Class I; 23.1% Class II; and 27.4% Class III. Class III patients had significantly lower odds of impacted teeth compared to Class I patients (odds ratio 0.608, 95% confidence interval 0.463–0.798; P=0.00009). There was no significant difference in the occurrence of the anomalies among the various anteroposterior skeletal types.
Conclusions:
The occurrence of impacted teeth was lower in Class III than Class I, while no significant differences were noted for hyperdontia, hypodontia, peg-shaped upper lateral incisors, transposition and double teeth. The occurrence of all investigated dental anomalies had no significant difference between Class II and Class I.
Introduction
Given the multifactorial aetiology of malocclusion, 1 it is postulated that there could be an association between malocclusion types and dental anomalies such as hyperdontia, hypodontia, peg-shaped upper lateral incisors, impacted teeth, transposed teeth or double teeth. If any association exists, it aids the clinician in being more cognisant in identifying these anomalies in patients with the respective malocclusion classes and being able to render appropriate investigations and treatment plans. Also, it sheds light on possible aetiological associations between these anomalies and malocclusion classes.
The prevalence of supernumerary teeth was determined by several studies to have no statistically significant difference between malocclusion classes.2–4 However, one study noted the prevalence of hyperdontia was significantly higher in Angle’s Class III malocclusion. 5 Similarly for hypodontia, some studies2,6–8 showed no significant difference between its prevalence among various malocclusion classes, while others found it to be higher in Class III9–12 and Class I. 13 For peg-shaped upper lateral incisors, its prevalence was observed to be greater in Class II 14 and Class II Division 2 malocclusion.4,15 The prevalence of impacted teeth was significantly lower in Class II Division 1 malocclusion than Class I in one study, 2 and significantly lower in skeletal Class II compared to both Class I and Class III in another study. 3 The prevalence of dental transposition was more commonly seen in Class II Division 2 malocclusion.4, 15 There were no notable studies which investigated the relationship between the prevalence of double teeth and malocclusion type. Therefore, the current published literature does not seem to be in agreement with respect to the relationship between these dental anomalies and malocclusion classes.
The primary aims of this retrospective study were to investigate: (a) the prevalence of skeletal Classes I, II and III in an ethnic Chinese orthodontic population; and (b) the difference in the occurrence of hyperdontia, hypodontia, pegged upper lateral incisors, impacted permanent teeth, transposed teeth and double teeth (gemination/fusion), excluding third molars, in the three aforementioned skeletal classes in an ethnic Chinese orthodontic population.
Methods
The study design was a retrospective cross-sectional study which investigated the records of consecutive patients who were seen at the Orthodontics Department in the National Dental Centre Singapore (NDCS) from 2011 to 2015. The study was approved by the SingHealth Centralized Institutional Review Board (CIRB reference number 2016/3042).
Patients who had visited the orthodontic clinic and had their records taken were eligible for enrolment into this study, according to the inclusion and exclusion criteria. All existing digital clinical records, photographs and radiographs were assessed. The patients need not have started orthodontic treatment after initial record taking.
Inclusion criteria:
Chinese ethnicity
14 to 25 years old at the time records were taken
Pre-treatment records of adequate quality and completeness (electronic clinical notes, medical history, intraoral clinical photographs, digital radiographs of at least one lateral cephalogram, one dental panoramic tomogram and one anterior maxillary occlusal).
Exclusion criteria:
Syndromic or oro-facial cleft patients
Prior craniofacial fractures or surgery
Undergone prior growth modification therapy
Extenuating medical conditions
Pre-treatment records that are incomplete or of inadequate quality.
The records of patients who met the criteria were classified into anteroposterior (AP) skeletal types of Class I, Class II and Class III based on the A point–Nasion–B point (ANB) angle 16 measured from the lateral cephalogram. The ANB norms were of the Southern Chinese population, 17 whereby Class I: ANB = 3.6° ± 2.5° (1 standard deviation; SD) that is 1.1° to 6.1°; Class II: ANB greater than 6.1°; Class III: ANB less than 1.1°. The lateral cephalogram was examined on the institution’s medical imaging and viewing software, Medicor Imaging (MiPACS), and the ANB angle was measured electronically with the MiPACS angular measurement tool.
The dental anomalies were identified according to the definitions as specified in a previous study by the same author: 18
Hyperdontia: The presence of one or more teeth or odontomes in addition to the regular number of permanent teeth; 5 diagnosed radiographically, or with evidence that a supernumerary tooth had been removed before, with sufficient details of the supernumerary tooth.
Hypodontia: Developmental absence of one or more permanent teeth (excluding third molars);9,19 diagnosed radiographically with no recognised mineralisation of the tooth crown, and no evidence that it had been removed before.
Peg-shaped upper lateral incisor: Undersized, tapered maxillary permanent lateral incisor which may be conical, have reduction in diameter from cervix to incisal edge, or with marked asymmetry in volume between right and left sides; 20 diagnosed with clinical photographs and radiographs.
Impacted tooth: The tooth is obstructed on its path of eruption by an adjacent tooth, bone, or soft tissue,21, 22 and does not appear to be able to continue to erupt into good functional occlusion without intervention. It may be unerupted or partially erupted; excludes third molars and supernumeraries; diagnosed with clinical photographs and confirmed radiographically.
Transposition: Positional interchange of two adjacent permanent teeth, especially of their roots, or the development or eruption of a permanent tooth in a position occupied normally by a non-adjacent tooth; 23 diagnosed radiographically.
Double teeth: Incomplete division of a single tooth germ (gemination), or the union between dentine and/or enamel of two or more separate developing teeth (fusion);24, 25 diagnosed with clinical photographs and radiographs.
The prevalence of each dental anomaly was determined for each AP skeletal class. All records were examined by a single investigator. One month after initial examination of records, the classification of each subject into the respective AP skeletal type and the assessment of dental anomalies were repeated on 30 randomly chosen subjects, to verify intra-examiner reproducibility.
Statistical analyses were performed using SAS 9.4 (SAS Institute Inc., North Carolina, USA). Intra-examiner reproducibility for the measurement of the ANB angle was tested using the Bland–Altman method, while intra-examiner reproducibility of assessment of dental anomalies was determined with Kappa coefficients. The association between AP skeletal class and occurrence of the various dental anomalies, if any, was determined with logistic regression. The Class I group was used as the control group. A significance level of 5% was set.
Results
Orthodontic records of 2508 consecutive patients were identified, of which 1418 were female (56.5%) and 1090 were male (43.5%). The patients’ records were classified according to AP skeletal type: Class I (n=1241, 49.5%); Class II (n=580, 23.1%); Class III (n=687, 27.4%). Figure 1 shows the distribution of the sample according to the AP skeletal type.
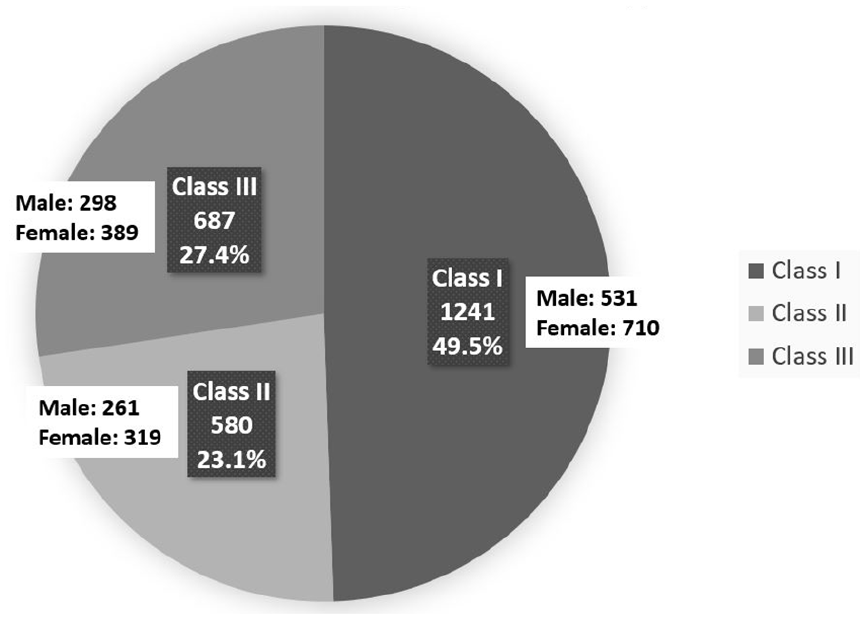
Distribution of anteroposterior (AP) skeletal type.
About 97% of the difference in ANB measurements fell within –0.3504 and 0.3678 (mean 0.0087 ± 1.96 SD). According to the Bland–Altman method, agreement has been achieved for the ANB measurement. There was 100% reproducibility for the classification of patients into skeletal Classes I, II and III within the sample of 30 repeats. There was also 100% reproducibility for the assessment of anomalies within the sample of 30 repeats. There was perfect agreement between the first and second assessments of hyperdontia, impacted teeth, and peg-shaped upper lateral incisors (kappa = 1, P<0.001). The agreement for missing, transposed and double teeth could not be evaluated in the sample of 30 repeats because all of them had no missing teeth, no transposed teeth and no double teeth.
More than a third (36.8%) of the sample had at least one anomaly of the permanent dentition. There was no statistically significant difference between males and females (odds ratio (OR) 1.101, 95% confidence interval (CI) 0.935–1.297; P=0.247). The prevalence of patients with at least one dental anomaly in Classes I, II and III was 39.2%, 35.9% and 33.3%, respectively. There was no statistically significant difference between Classes II and I (OR 0.869, 95% CI 0.689–1.096; P=0.312). There was a statistically significant difference between Classes III and I (OR 0.777, 95% CI 0.622–0.970; P=0.022). Patients of Class III skeletal type had significantly lower odds of having at least one dental anomaly compared to patients of Class I skeletal type.
The prevalence of dental anomalies in various skeletal types is summarised in Table 1. There was no statistically significant difference in the prevalence of dental anomalies (hyperdontia, hypodontia, peg-shaped upper lateral incisors, transposed teeth and double teeth) between the various skeletal types. Patients of Class III skeletal type had lower odds of having impacted teeth compared with patients of Class I skeletal type (OR 0.608, 95% CI 0.463–0.798; P=0.00009).
Summary of results.

Class III patients were found to have significantly lower odds of having impacted teeth compared with Class I patients (OR 0.608, 95% CI 0.463–0.798; P=0.00009).
Discussion
In studies investigating the relationship between dental anomalies and malocclusion of Caucasian populations, the proportion of skeletal Class III in such populations were low, ranging between 1.6 and 5.5%.26–28 On the other hand, in Chinese populations, it had been reported to be between 13% and 22.9%.29–31 In this study, sampling was restricted to ethnic Chinese orthodontic patients, which allowed for a sizeable proportion of subjects with Class III skeletal jaw relationships in the sample, and for representative findings without the confounders of anatomical differences in multiracial groups.
This study showed that Class III patients were found to have significantly lower odds of having at least one dental anomaly and of having impacted teeth compared to Class I patients. Skeletal Class III can most commonly be attributed to maxillary hypoplasia, mandibular prognathism or a combination. However, the current study did not distinguish between the horizontal skeletal subtypes that resulted in the Class III presentation. In this study, the most commonly impacted tooth was identified to be the lower second molar (46.4% of all impactions). 18 Assuming the Class III skeletal pattern is attributed in part to a prognathic mandible, the odds of an impacted tooth could be lower given the larger arch length in a prognathic mandible.
However, this differs from the results of another study, 3 which demonstrated a statistically significant lower prevalence of impacted teeth in Class II compared to Classes I and III patients. The same study also revealed no difference in the prevalence of tooth impaction between Class I and Class III. In another study, 32 the prevalence of impacted lower permanent second molars was shown to be greater in Angle’s Class II compared to Class I patients. These may be due to the difference in the population, sample size, age range, inclusion and exclusion criteria, definitions of anomalies studied and tools of assessment.
The aetiology of both skeletal Class III and tooth impaction are multifactorial, each with respective genetic and environmental factors. The results of this study showed a statistically significantly lower occurrence of tooth impaction in the skeletal Class III group. Therefore, it can also be postulated that there could be some underlying common genetic aetiology linking this Class III presentation and the development of impacted teeth. However, this will require further investigation with better designed studies before it can be concluded accurately.
Clinical significance
To date, there has been no study which investigates the prevalence of the various AP skeletal relationships in the Singapore population. The information from this study is useful in counselling patients on the prevalence of AP skeletal types and dental anomalies. This is especially important because dental anomalies are commonly seen in orthodontic patients, regardless of skeletal type. A higher index of suspicion can also be employed by clinicians in locating impacted teeth in skeletal Classes I and II patients, as compared to Class III patients.
Future directions
This study investigated the AP dimension of the skeletal jaw relationship. Future similar studies can be conducted to investigate the relationship between the vertical dimension of the skeletal jaw relationship and the occurrence of dental anomalies in the average angle, low angle and high angle skeletal groups. Furthermore, it is worthwhile to consider the genetic, epigenetic and environmental factors related to the development of skeletal types and dental anomalies. Future epidemiological studies can compare data from this study with data obtained from first degree relatives of these patients to explore the factors which determine skeletal types and dental anomalies.
Conclusions
The prevalence of AP skeletal types in an ethnic Chinese orthodontic population is 49.5% Class I, 23.1% Class II and 27.4% Class III.
The Class III skeletal type had a lower odds of having impacted teeth compared with patients of Class I skeletal type.
There was no significant difference in the occurrence of hyperdontia, hypodontia, peg-shaped upper lateral incisors, transposition and double teeth among the AP (Classes I, II, III) skeletal types of ethnic Chinese orthodontic patients.
Footnotes
Acknowledgements
The author(s) would like to thank the National Dental Centre Singapore for providing the necessary records for this study.
Authors’ contributions
GXL Chan conceived the presented ideas and methodology, conducted literature search, carried out data acquisition, data analysis and prepared the manuscript. HC Wong performed the statistical analyses. ELY Tan and M Yow provided critical feedback, reviewed and edited the manuscript. MT Chew and KWC Foong reviewed the manuscript before submission.
Availability of data and materials
Data sharing is not applicable to this study and datasets are stored confidentially with the National Dental Centre Singapore.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval to report these cases was obtained from the SingHealth Centralized Institutional Review Board (CIRB reference no.: 2016/3042)
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent for individual patients was not sought due to the large number of patients involved and the non-invasive nature of this retrospective study.