
Abstract
Background:
Optimal hand function recovery is the key to the successful management of hand burns. It starts with a timely burns coverage in the acute setting. A new hand burns protocol has been introduced to cover hand burn wounds within 24 hours after admission. BiobraneTM and split skin graft (SSG) are the coverage methods for partial-thickness burns. A three-year prospective study is being carried out to evaluate the short- and long-term clinical and functional outcomes of the two treatment modalities. This paper reports the preliminary short-term results of the first 34 hand burns of the study.
Methodology:
This report includes consecutive hand burns patients admitted between September 2014 and May 2015. The recruited hand burns patients underwent clinical and functional assessments seven days after the coverage with either SSG or BiobraneTM. Statistical analysis was performed to evaluate the outcomes.
Results and discussion:
Eleven burnt hands were treated with SSG and 23 with BiobraneTM. The clinical and functional outcomes, including range of motion, power and sensitivity, were similar in both treatment groups. Further study to recruit more patients is necessary to ascertain the significance of the above findings. More importantly, long-term functional outcomes have to be assessed to conclude the treatment efficacy of early hand burns coverage with BiobraneTM or SSG.
Introduction
As the primary interface between us and the environment, hands burns account for 50–80% of burns cases, despite contributing to only 3% of the total body surface area (TBSA). 1 Optimal hand function recovery after burns is essential for re-integration back into the society and occupation. 2 Burn wound coverage, early mobilization and aggressive physiotherapy are the cornerstones in hand burns management to achieve good functional recovery. 3
Recent studies have shown that early debridement and split skin graft (SSG) coverage of hand burns result in significantly better outcomes than delayed coverage.4,5 Early coverage has been observed to have several important advantages – it prevents the worsening of burn injury by stopping tissue conversion from the zone of stasis into the zone of coagulation, it decreases wound infection by the removal necrotic tissues, and it minimizes soft tissue desiccation, allowing early mobilization. In view of the benefit of early coverage, a new hand burns protocol was implemented in our department in September 2014. 6
There is an armamentarium of rapid burn wound coverage options, both biological and synthetic, with their own distinct advantages and disadvantages. 7 In our practice, SSG and BiobraneTM are used for coverage of partial-thickness hand burns.
SSG is a time-proven modality for the coverage of hand burns. Combined with tangential excision of the burn wound, excellent functional recovery has routinely been achieved. 8 SSGs have the distinct advantages of being readily available in most burns patients and provide a definitive skin coverage as an autologous tissue.
However, the availability of SSG is often limited for severely burned patients. The harvesting of the SSGs is often associated with significant donor-site morbidity. The preparation of recipient sites by tangential excision inevitably removes some healthy tissue, especially in mixed-depth burns, contributing to poor wound healing. Finally, SSG-covered hands will require immobilization for 5–7 days to allow for graft take, which worsens joint stiffness.
BiobraneTM was developed in 1979 by Woodroof to serve as a definitive partial-thickness wound dressing. 9 It is a biosynthetic wound dressing made of porcine dermal collagen-bonded nylon membrane on a silicon scaffolding. It possesses many of the characteristics of an ideal dressing. It is readily available without any donor-site morbidity. Minimal debridement is required to prepare the burns wound bed to apply the dressing. Furthermore, it is easy to apply, and range of motion (ROM) exercises can begin as early as post-operative day (POD) 3. The development of the BiobraneTM glove further simplifies the process of application of the dressing to hand burns. 10
However, the high cost of BiobraneTM limits its role as a general dressing. Its efficacy is very dependent on the wound condition; contaminated or infected wounds, deep burns and exudative wounds often lead to the failure of the dressing.
Few literature has compared the functional outcome of BiobraneTM with SSG in managing partial-thickness hand burns. A study by an Australian centre comparing the functional outcome of BiobraneTM and SSG found that the group treated with BiobraneTM showed better functional recovery. 11 However, the small number of participants – 24 in the BiobraneTM group and four in the SSG group – limits the significance of these findings. Moreover, this study was conducted with a Caucasian population and the findings may differ from that of an Asian population.
Our centre has embarked on a three-year-long prospective study to evaluate the short- and long-term functional outcomes of partial-thickness hand burns managed by BiobraneTM and SSG. This paper serves as a preliminary report of the early functional recovery (POD 7) of these two groups of patients.
Methodology
New burns protocol
The new Singapore General Hospital (SGH) Burns Protocol was introduced in our centre on 1 September 2014 to streamline the communication process between the Emergency Department, the Department of Anaesthesia and the Department of Plastic, Reconstructive and Aesthetic Surgery for the management of burns. The aim was to provide aggressive early wound debridement and coverage within 24 hours of admission. Early data has shown improvement in mortality and morbidity in patients managed with this protocol. There was also an associated cost reduction and shortened hospitalization. 6
Hand burns patient
This prospective study was conducted on consecutive patients with superficial partial-thickness hand burns admitted to the Department of Plastic, Reconstructive and Aesthetic Surgery, Singapore General Hospital from 1 September 2014 to 31 May 2015. The inclusion criterion was patients with superficial dermal partial-thickness hand burns admitted for surgery. Patients with deep-dermal partial- to full-thickness burns were excluded from this study. In addition, patients with burns involving >40% TBSA were also excluded.
Patients in the study underwent debridement and coverage of their hand burns with either BiobraneTM or SSG, depending on time of presentation after burn injury. BiobraneTM was applied for patients who presented within 48 hours after sustaining the burn injury. SSG was the choice of treatment for patients presented with hand burns beyond 48 hours after injury. SSG was also used for patients who refused BiobraneTM due to personal belief.
In the application of BiobraneTM, burn wounds were debrided minimally under general anaesthesia to remove non-viable epidermis and hair. Thereafter, the BiobraneTM glove was applied and secured with Hypafix. The hand was then immobilized in an Intrinsic Plus position and inspected on POD 2 and POD 5. If wounds were healing well, the patient would be reviewed by a physiotherapist to begin gentle ROM exercises.
In SSG coverage, burn wounds were tangentially excised with a Goulian knife until viable bleeding tissue was visualized. SSG was harvested with the Dermatome in 10/1000-inch thickness from the inner thigh. It was then fenestrated with the blade and applied to the hand wounds with Vicryl 5/0 sutures. The hand was immobilized for 7 days to allow for graft take. The SSGs were reviewed on both POD 2 and POD 7. If grafts were well taken, patients were allowed gentle ROM exercise on POD 7.
Clinical and functional assessment
Hand functional assessment consisting of grip strength, ROM, two-point discrimination, pressure sensitivity and pain was performed on POD 7. Measurements of the parameters were performed by two experienced occupational therapists. Grip strength was measured using the dynamometer. A two-point discriminator was used to determine two-point discrimination. Pressure sensitivity was measured with Semmes–Weinstein monofilament. Joint ROM was measured with a goniometer. A pain rating scale (0–10) was used to assess the pain experienced by patients. Photos were taken both before and after the operation, at POD 2 and POD 7.
Pressure sensitivity was tested at three different points over the area of burn, the average taken and recorded. A 2.83 monofilament corresponding to normal pressure sensitivity was given a score of 1; 3.61 corresponding to diminished light touch was given a score of 2; 4.31 corresponding to diminished protective touch was given a score of 3; 4.56 corresponding to loss of protective touch was given a score of 4. If no sensation was felt at 6.65, the patient was deemed untestable and given a score of 5.
Total active motion (TAM) for the individual digit was calculated by adding up all joints’ ROM of the digit (distal interphalangeal joint, proximal interphalangeal joint and metacarpal phalangeal joint for finger; interphalangeal joint and metacarpal phalangeal joint for thumb). Normal TAM for the finger is 260 degrees, and 140 degrees for the thumb. The TAMs of the involved digits were divided by the normal TAM value to calculate the functional ROM percentages of the digits. The average of the functional ROM percentage of all burnt fingers on one hand would be considered as the functional ROM percentage of the hand.
Data analysis
A two-tailed Student’s t-test was carried out to analyse the functional outcomes of the two groups using SPSS version 13 software.
Results
Patient demographics
A total of 23 patients with 34 superficial partial-thickness hand burns were included in this study. All 23 hand burns patients were managed with either BiobraneTM or SSG. All burns were thermal burns from being in contact with hot water or flames.
Fifteen patients with 23 hand burns were managed with BiobraneTM. The mean age was 34 and mean TBSA was 10.7%. The mean duration from burns injury to operation was 0.7 days. Patients managed with SSGs had a mean age of 40, a mean TBSA of 12.6% and were operated on at 3.2 days from burn injury on average (Table 1). All patients showed excellent response to treatment and were discharged when their hand burns were epithelialized. There was an SSG patient whose recovery was complicated by donor-site infection, although this was treated medically and resolved prior to discharge.
Patient demographics.
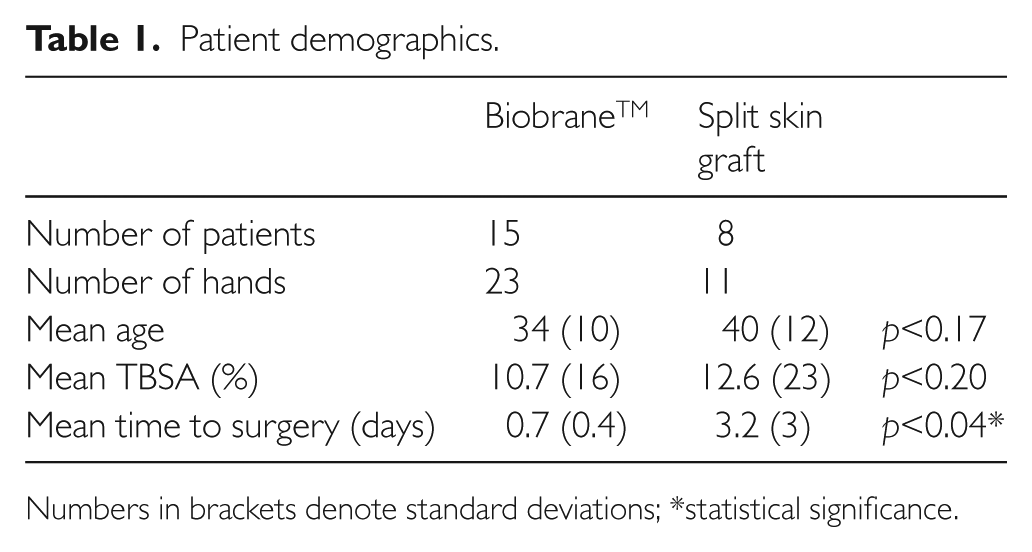
Numbers in brackets denote standard deviations; *statistical significance.
Case 1: BiobraneTM glove
Patient A was a 46-year-old Chinese male working as a chef. He was of right dominance and had no significant past medical history. The patient sustained a 2.5% TBSA burn involving his left hand and forearm after being scalded by hot water while cooking. He presented to A&E on the same day and BiobraneTM coverage of his hand burns was performed within 24 hours. Mobilization was started on POD 5 and full epithelialization was noted on POD 7 (Figure 1). The patient was discharged with outpatient occupational therapy treatment and clinical follow-up.

Patient A. A–C: Pre-op photo of superficial partial-thickness burns of the left hand involving the dorsum and thenar eminence; D–F: POD 2 after being treated with BiobraneTM glove; G–I: Full epithelialization on POD 7.
Case 2: split skin graft
Patient B was a 33-year-old Indian male working as a software engineer. He was of right dominance and had no significant past medical history. The patient sustained a 5% TBSA burn on his right hand after being burned by a firecracker. He was initially treated conservatively with antibiotics and dressings in India for two days, and presented at SGH with right-hand burns. Wound debridement and Vacuum assisted closure (VAC) dressing was carried out at the SGH Burns Unit before SSG coverage five days later. The SSG was noted to be fully taken at POD 7 and mobilization was initiated on POD 7 (Figure 2).

Patient B. A–C: Pre-op photo of mid- to deep-dermal partial-thickness burns of the right hand involving the dorsum and thenar eminence; D–F: POD 2 after being treated with SSG; G–I: SSG fully taken at POD 7.
Short-term functional outcomes
For participants whose burn injuries were managed with BiobraneTM, their mean two-point discrimination was fair (9.1 mm) at seven days, post-treatment, their mean active ROM was 76% of baseline and grip power was 12.6 N on average. Mean pressure sensitivity was 2.1 when measured using a Semmes–Weinstein monofilament, and mean pain score was 0.1 out of 10. In the group of patients managed with SSG, the mean two-point discrimination was fair (10.1 mm), mean ROM was 60% of baseline and mean grip power was 8.6 N. Patients in the SSG group had 2.5 mean pressure sensitivity and a mean pain score of 0.1 out of 10.
The two-tailed Student’s t-test was performed to analyse the short-term functional outcomes of the two groups (Table 2). The difference in active ROM and pressure sensitivity were found to be statistically significant, while differences in the other parameters of grip power, two-point discrimination and pain were not statistically significant.
Patient outcomes at POD 7 according to the method of burn management.
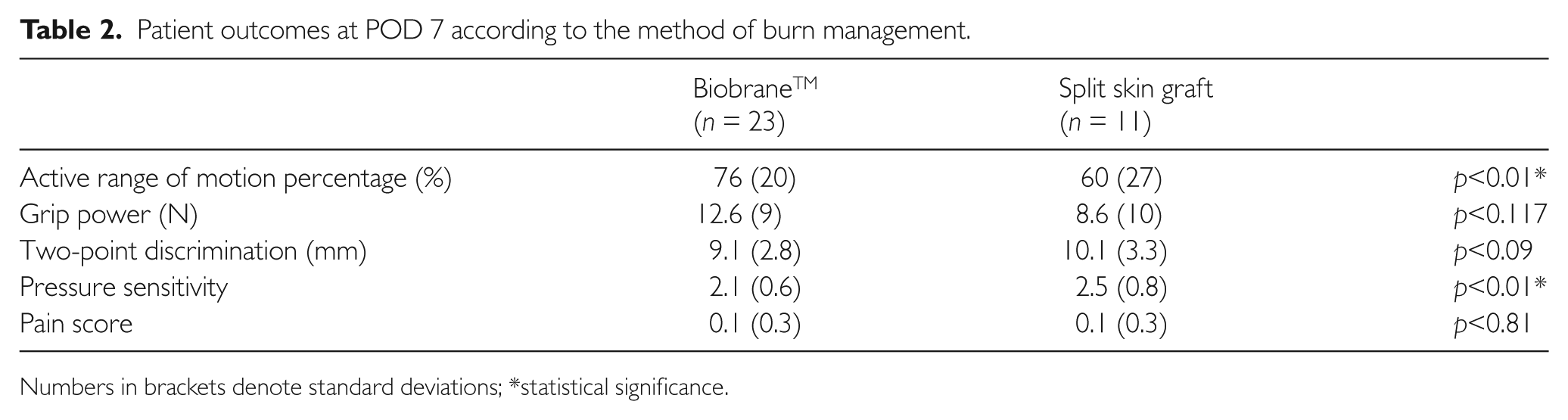
Numbers in brackets denote standard deviations; *statistical significance.
Discussion and conclusion
Both BiobraneTM and SSG have proved to be effective in treating superficial partial-thickness hand burns. Early coverage and aggressive physiotherapy have resulted in good functional recovery in the early post-operative period for both treatment modalities.
Our early results suggested that patients treated with BiobraneTM had better short-term functional recovery as compared to those with SSG coverage. Significant differences were noted in active ROM and pressure sensitivity of the hands.
The observations of better active ROM may be contributed by two factors. Firstly, earlier hand mobilization in the BiobraneTM group on POD 5 meant shorter periods of joint immobilization and earlier physiotherapy exercises, resulting in better recovery of joint ROM. Secondly, the time interval from sustaining the burn injury to receiving treatment was shorter in the BiobraneTM group. This time interval was 0.7 days for the BiobraneTM group but 3.2 days for patients in the SSG group. The shorter time interval reduced voluntary self-immobilization of the hand due to the raw wound, resulting in less joint stiffness
A tangential excision had to be done to prepare the wound bed for SSG coverage. However, only minimal wound debridement was required before BiobraneTM application, which could have resulted in better preservation of delicate nerve endings in the BiobraneTM group. The preserved nerve endings likely contributed to the better pressure sensitivity in BiobraneTM group.
The mean grip power and two-point discrimination were better in the BiobraneTM group, but this was not of statistical significance and was probably due to chance.
Significant morbidity was experienced by a patient in the SSG group from donor-site infection, which was treated with a course of antibiotics, bed rest and one month of dressing before resolution. In addition, the hyperpigmentation and scarring would require many more months to resolve.
BiobraneTM has shown to be an effective treatment for superficial partial-thickness hand burn patients who present within 48 hours of burn injury. Our preliminary data have shown that patients managed with this modality had excellent early functional recovery without donor-site morbidity compared to those treated with SSG. More patients are to be recruited in future studies to increase the power of this study. Further follow-ups of these hand burns patients are necessary to assess the long-term functional outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.