
Abstract
Introduction
The Mediterranean diet is a well-known dietary pattern currently studied worldwide for its palatability, high acceptance from the general population, and its proven beneficial effects on human health. 1 Referred to the historical dietary habits of individuals living in the countries facing the Mediterranean sea, the Mediterranean diet is characterized by some key features, including (i) promoting frequent intake of plant-based foods, such as fruit, vegetables, whole grains, nuts, and legumes, (ii) daily use of olive oil as main dressing, (iii) moderate alternative consumption of animal protein sources, namely dairy products, poultry, fish, eggs, and unprocessed red meat, and (iv) limitation concerning processed animal foods and elaborated sweets. 2 Specific underrated characteristics of the Mediterranean diet are also the common use of herbs and spices, preference for locally-produced, minimally processed products, slow and easy cooking procedures, as well as frugality and conviviality as integrated parts of an overall lifestyle. 3 The combination of such features is associated with certain dietary nutritional quality, including an adequate daily allowance of antioxidant vitamins and phytochemicals (such as polyphenols), an adequate amount of daily fiber, a good ratio of healthy/unhealthy fats, and supposedly limited amount of simple sugars. 4 Such main features of this dietary pattern lead to higher diet quality from a nutritional point of view.5–9 Overall, higher adherence to the Mediterranean diet has been associated with substantial benefits toward cardio-metabolic health and decreased risk of certain cancers, neurodegenerative diseases, and overall general prolonged lifespan. 10 Concerning the potential effects of the Mediterranean diet in younger generations, several reports have shown a relation with better mood, lower distress, and improved quality of life.11–14 Importantly, adoption of a healthy Mediterranean diet since early childhood would also lead to important long-term benefits, including improvement in metabolic parameters and improved development of the immune system.15–17 Potential mechanisms involved in such effects may involve a modulatory effect on inflammatory biomarkers also in children and adolescents, suggesting anti-inflammatory benefits. 18
Current evidence suggests that adherence to the Mediterranean diet has gradually decreased over time.19,20 On one side, industrialization as well as social and economic development has led to richer food options, 21 including higher availability of nutrient-rich, animal-based products leading to an improvement in diet quality globally. 22 On the other side, the large input from the industry and the rise in nutrient-poor, calorie-rich foods has increased globally, leading to an overall abandonment of this traditional dietary pattern and preference of unhealthier, yet often more palatable alternatives. 23 Recent evidence showed a substantial decrease in nutritional diet quality associated with increasing energy shares of highly processed foods in nationally representative samples globally. 24 Such trends have been reported to have an even greater impact among the younger generations, notoriously more sensitive to industrialized, heavily marketed products, in spite of their nutritional quality.25–27 Curiously, recent reports emphasized how the phenomenon of “nutrition transition” and the shift toward more “Westernized” dietary patterns is particularly interesting to those populations living in the Mediterranean area.28–30 The abandonment of traditional dietary patterns is considered a potential threat for the future health of younger individuals, since the establishment of unhealthy dietary behaviors at younger age are correlated with negative outcomes during adulthood, including higher risk of obesity, type-2 diabetes, and hypertension to begin with. 31
Over the last decade, several projects have been developed to investigate eating habits in children and adolescents and eventually promote healthy dietary behaviors and adoption of traditional dietary patterns.32,33 In this context, the aim of this study was to describe current eating habits and the level of adherence to the Mediterranean diet in children and adolescents living in 5 Mediterranean countries participating to the DELICIOUS (UnDErstanding consumer food choices & promotion of healthy and sustainable Mediterranean Diet and LIfestyle in Children and adolescents through behavIOUral change actionS) project.
Methods
Study design and population
The present study is based on the cross-sectional analysis in the context of the European-funded DELICIOUS project. The details of the study protocol have been described elsewhere. 34 For the purposes of this study, a consumer survey was conducted among parents of children and adolescents aged between 6 and 17 years old from five Mediterranean countries (Italy, Spain, Portugal, Egypt, and Lebanon). Participants were recruited based on their voluntary agreement in being included in a country-specific consumer database within the network of the Technological Institute for children's products & leisure (AIJU). A target of at least 400 individuals per each Mediterranean country balanced by age and sex of children and adolescents (assessed at the recruitment). Potential participants were provided with the following content: (i) the objective of the study, (ii) the link to the questionnaire, (iii) the link to communicate that the participant does not want to answer the questionnaire, and (iv) the link to unsubscribe in the event that the participant does not want to receive further notifications to participate in the surveys. If accepted to participate, all information concerning the aim of the project, estimated duration of the questionnaire, how the information will be transferred to third parties, as well as potential benefits, possible risks, security, privacy and confidentiality issues were provided. The data collection was assessed via an electronic survey and a total number of 2011 individuals was included in this study. All the procedures were carried out in accordance with the Declaration of Helsinki (1989) of the World Medical Association and all participants signed an informed consent form before the participants to the study. The study protocol was approved by the ethics committee of Mondragon University (no. IEB-20230704).
Data collection
Data regarding demographic (i.e., sex, age, educational and occupational level of the parents and sex, age, and anthropometric measurements of children/adolescents) and lifestyle characteristics (i.e., level of physical activity, screen time, and sleep time of children/adolescents) were collected. Parents’ educational level was categorized as: (i) low (primary), (ii) medium (secondary), (iii) and high (tertiary), while occupational level was categorized as: (i) unemployed and (ii) currently working. Physical activity level was assessed using the International Physical Activity Questionnaire (IPAQ) short form, which reports the level of physical activity, referred to the last 7 days before compilation, about three specific types of activities (walking, moderate-intensity activities, and vigorous intensity activities); frequency (measured in days per week) and duration (time per day) are collected separately for each specific type of activity. 35 Finally, participants were asked how many hours on average their children are sleeping per day, and according to the National Sleep Foundation recommendations for school-age children and teenagers, sleep duration (in hours) was categorized considering: (i) <8 h, (ii) 8–10 h, and (iii) >10 h, 36 while screen time (in hours) was categorized as: (i) <2 h/day, (ii) 2–4 h/day, and (iii) >4 h/day.
Dietary assessment and Mediterranean diet adherence
Using a semi-structured 24-h recall, dietary information was collected. Participants were asked the type of foods and drinks for each meal (including snacks) their offspring had consumed in the previous 24 h among 20 main food groups provided in the electronic form and an open-ended space for additional free entries. Moreover, additional questions concerning the frequency of consumption from never to weekly and daily intake were asked for 13 main food groups included in the Mediterranean Diet Quality Index (KIDMED), 37 a tool used to assess the level of adherence to the Mediterranean diet which includes 16 yes/no questions on dietary and eating habits, with answers to questions that had a negative connotation towards the Mediterranean Diet (i.e., frequent consumption of meat or skipping breakfast) receiving a score of −1, while those that indicated a Mediterranean habit (i.e, consumption of plant-based foods) received a score of +1. The overall KIDMED score varied from 0 to 12 points, with higher points reflecting higher adherence to the Mediterranean diet. The KIDMED score was also divided into three categories of Mediterranean Diet adherence: high adherence (score ≥8), medium adherence (score 4–7), and low adherence (score ≤3).
Statistical analysis
Categorical variables were presented as absolute numbers and relative frequencies (%), and continuous variables were reported as means (standard deviations, SDs). Differences between mean KIDMED and E-KINDEX scores between countries and groups based on variables of background were tested with Student's t test and ANOVA if variables were normally distributed or Mann-Withney u test and Kruskall–Wallis test if not normally distributed. Differences for categorical variables were tested by the chi-squared test. All p-values were reported as two-sided and compared to a significance level of 5%. SPSS 27 (SPSS Inc., Chicago, IL, USA) software was used for all the statistical calculations.
Results
The mean KIDMED score for the whole sample was 6.1 (SD 2.0), with some negligible differences across countries (Figure 1). Specifically, Lebanon and Portugal had slightly higher mean KIDMED scores than the other countries [Lebanon (mean 6.5, SD 1.8), Portugal (mean 6.4, SD 2.0), Italy (mean 6.2, SD 2.1), Egypt (mean 5.8, SD 2.1), and Spain (mean 5.7, SD 2.0)] (Figure 1). Although with small, yet not significant differences, adolescents in Italy and Portugal had lower adherence to the Mediterranean diet assessed through the KIDMED than children. When looking at the level of adherence to the Mediterranean diet, there was a lower proportion of individuals in the low adherence group in Lebanon, and a relatively higher proportion of high adherent in Lebanon, Italy, and Portugal (Figure 2). These differences were due to a much lower share of children less adherent to the Mediterranean diet in these countries counterbalanced by a higher proportion of higher adherent compared to adolescents, although this trend was not observed in Lebanon (Figure 2).
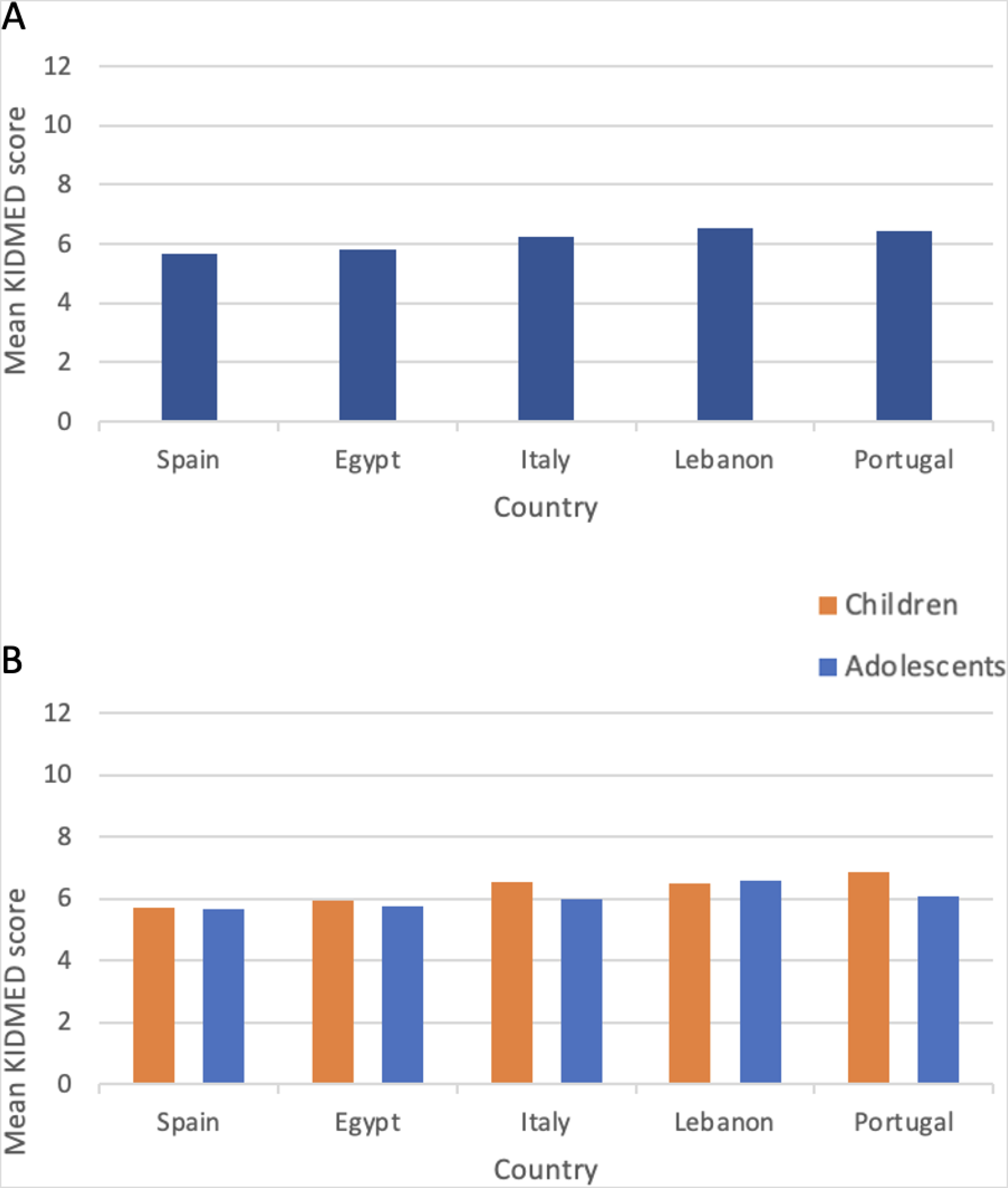
Country-specific mean KIDMED scores for the total sample (A) and stratified by age groups (children vs. adolescents) (B).
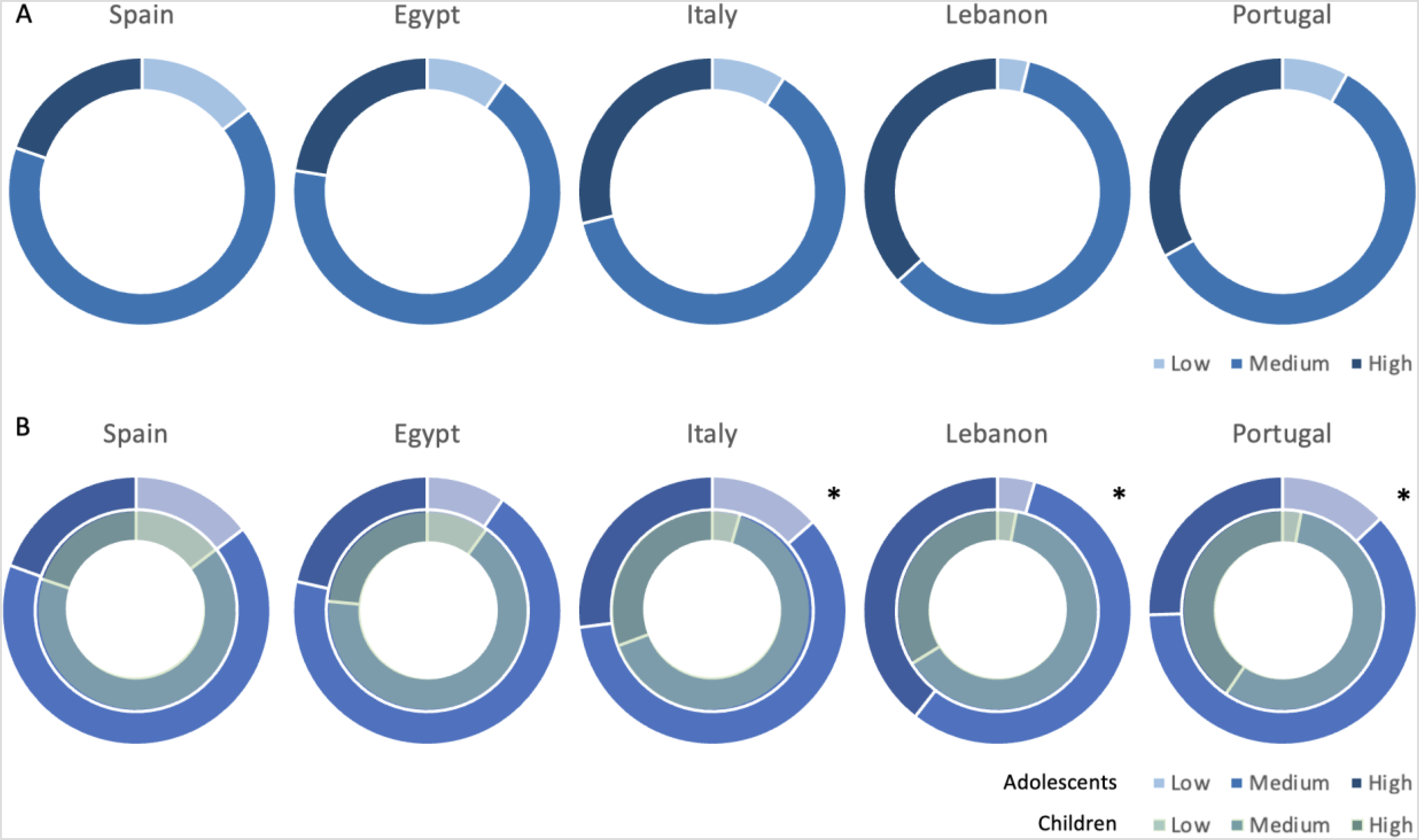
Country-specific percentage of individuals falling into low, medium, and high adherence to the Mediterranean diet categories in the total sample (A) and stratified by age groups (children vs. adolescents) (B).
The responses to the KIDMED questionnaire are presented in Figure 3. In general, some positive components of the KIDMED score were commonly adopted by children and adolescents (i.e., olive oil consumption and daily fruit or fruit juice consumption) while others only in a minority of participants (i.e., daily consumption of pasta, cereals, and nuts). Among negative components, daily sweet and candy consumption and skipping breakfast are relatively poorly adopted (Figure 3). When the analyses were stratified by age groups, the responses to most questions did not differ substantially in most cases; however, there was a higher proportion of adolescents reporting having cereals and dairy for breakfast compared to children (Figure 3).
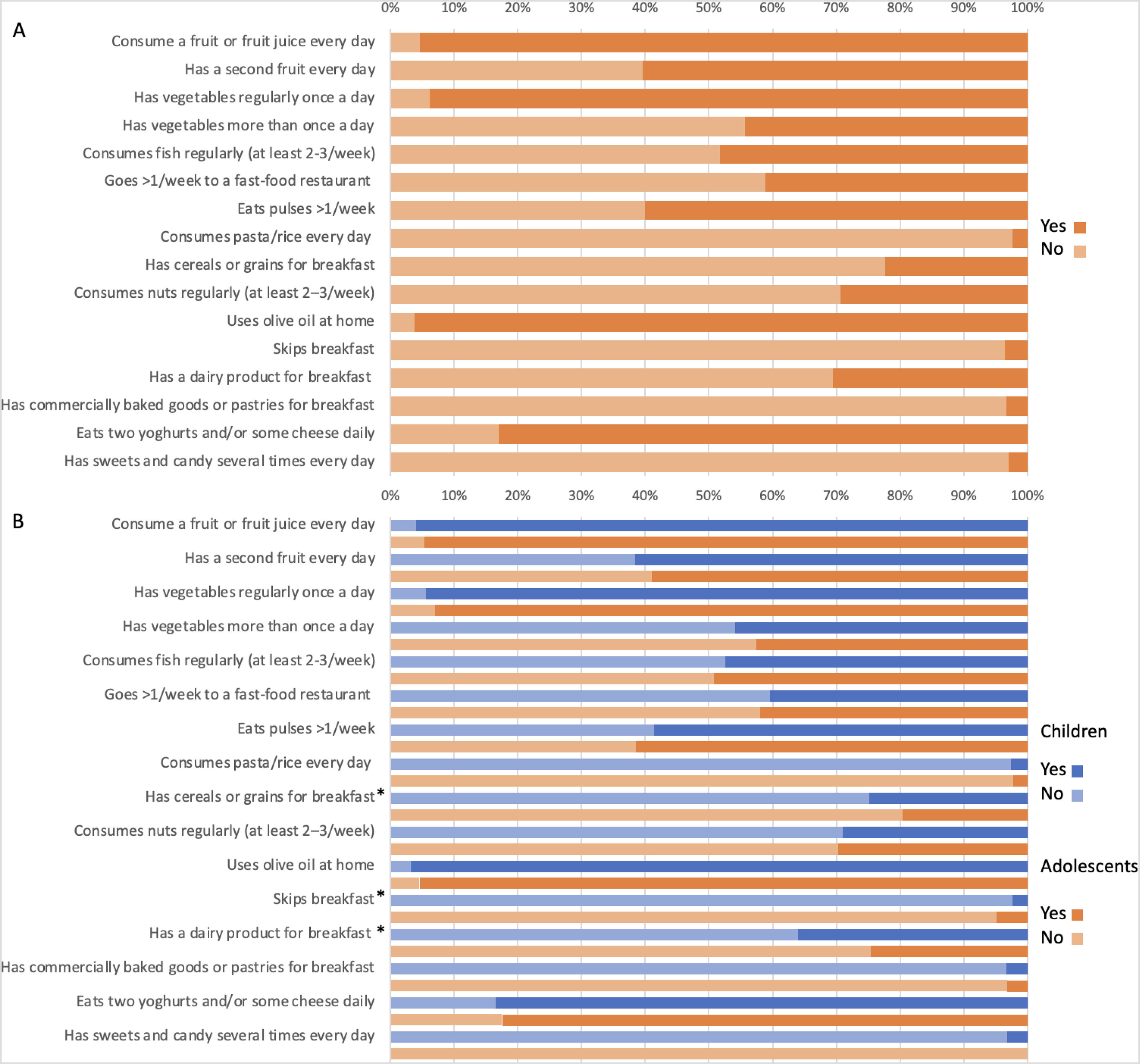
Responses to the KIDMED questionnaire in the total sample (A) and stratified by age groups (children vs. adolescents) (B).
The individual components of the KIDMED questionnaire by country are presented in Figure 4: some differences were evident concerning pasta and rice consumption (less consumed in Spain and Portugal), sweets and candies (less consumed in Italy), but also nuts (less consumed in Egypt) and having baked goods and sweets (less consumed in Italy and Portugal). In contrast, balanced responses about olive oil use at home, fruit and vegetable consumption, and having pulses weekly were detected.
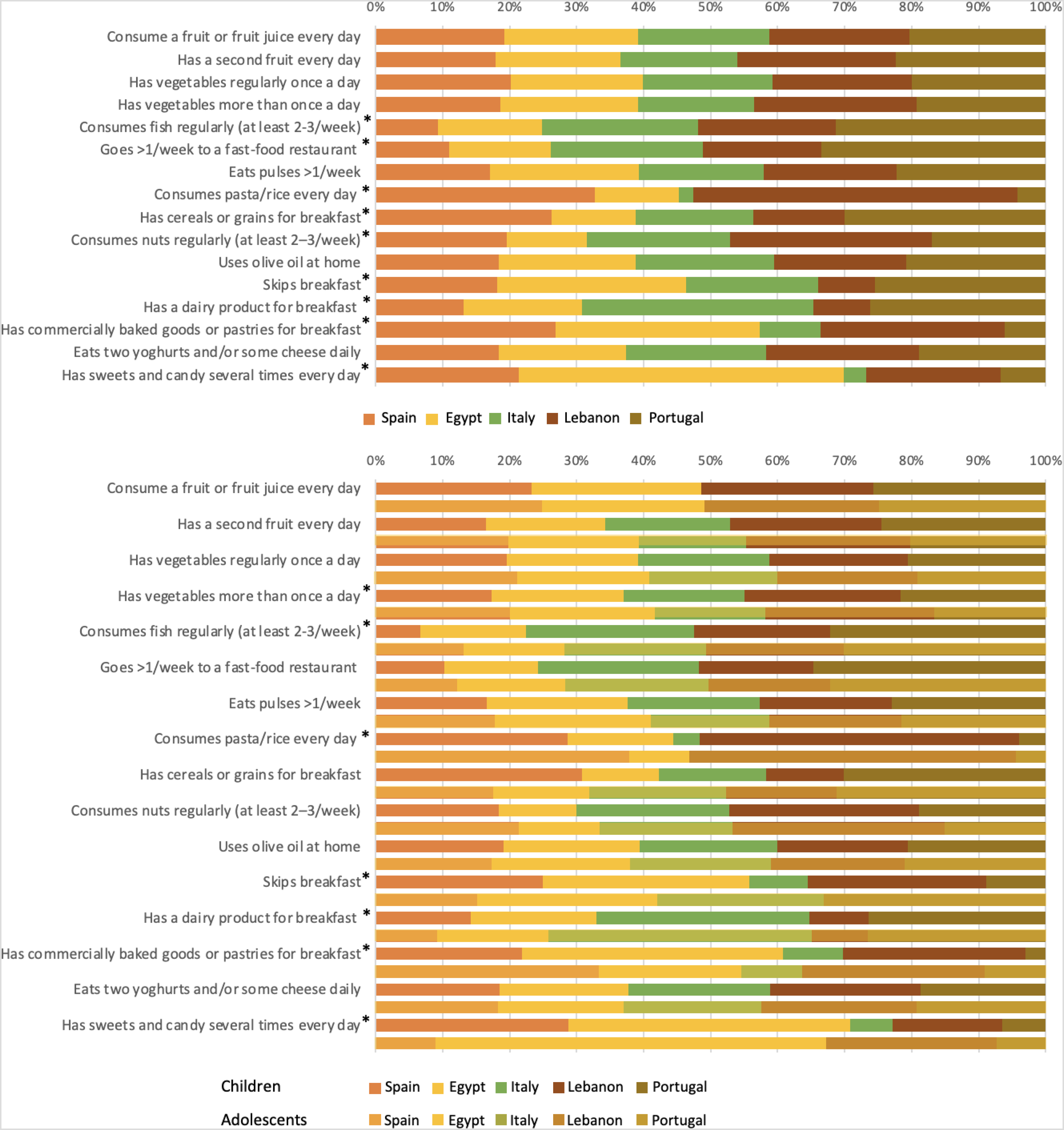
Positive responses to the KIDMED questionnaire in individual participating countries in the total sample (A) and stratified by age groups (children vs. adolescents) (B).
The differences in mean KIDMED scores by main study characteristics of children are reported in Table 1. Adolescents had significantly lower KIDMED scores, with significant differences denoted in Italy and Portugal. Among lifestyle variables, lower KIDMED scores were also detected among children and adolescents reported having inadequate sleep duration, longer screen time, and low physical activity levels, but only the latter was significant in all countries (Table 1).
Mean KIDMED scores across categories of children's and adolescents’ background variables, total and by country.
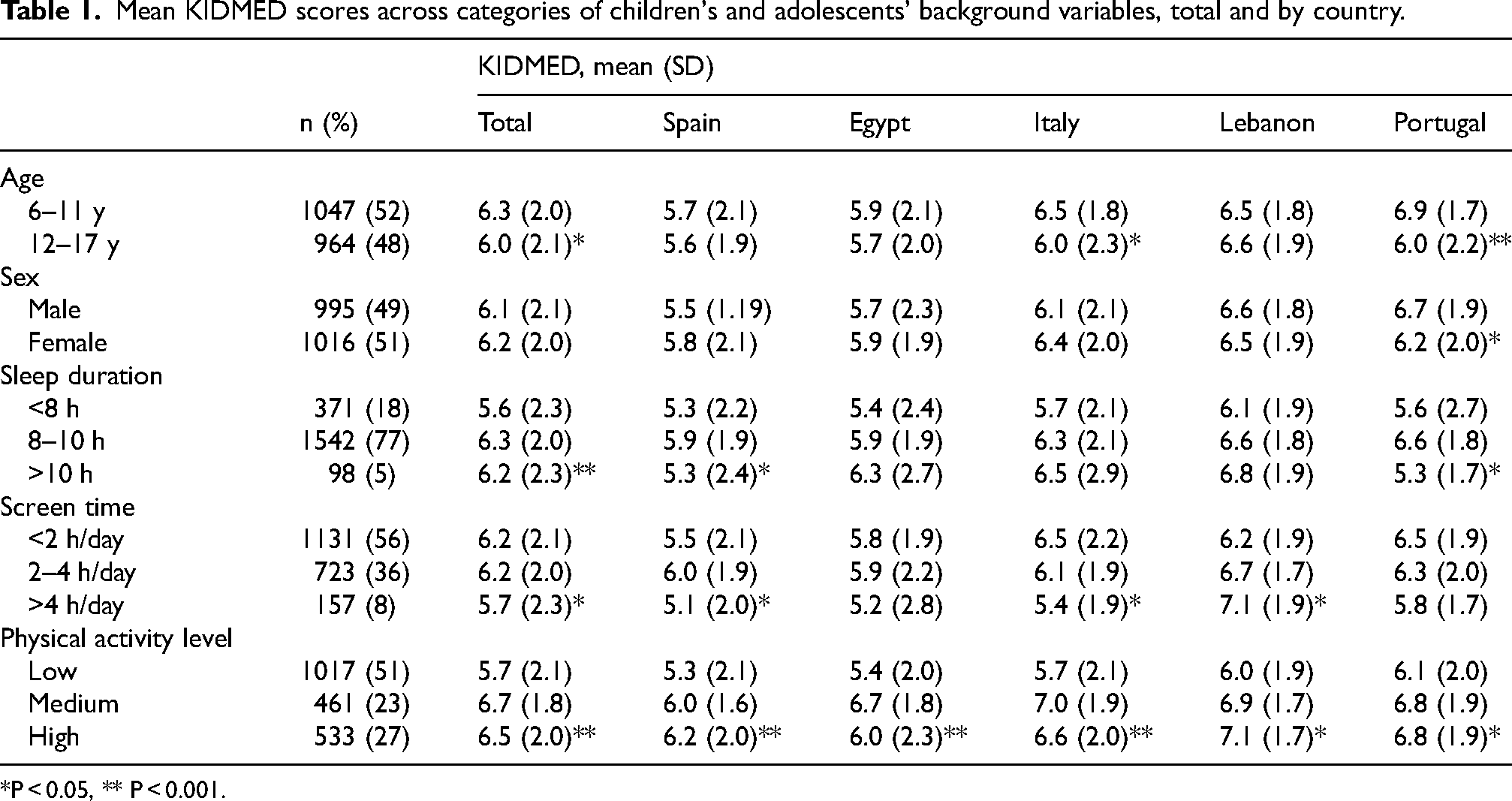
*P < 0.05, ** P < 0.001.
Among parents’ characteristics, significantly lower KIDMED scores of children and adolescents were detected in participants with lower educational levels consistently found in all countries but Lebanon (Table 2). Also low family income and rural area of living related with lower KIDMED scores, although significantly only in Spain (Table 2).
Mean KIDMED scores across categories of parents’ background variables, total and by country.
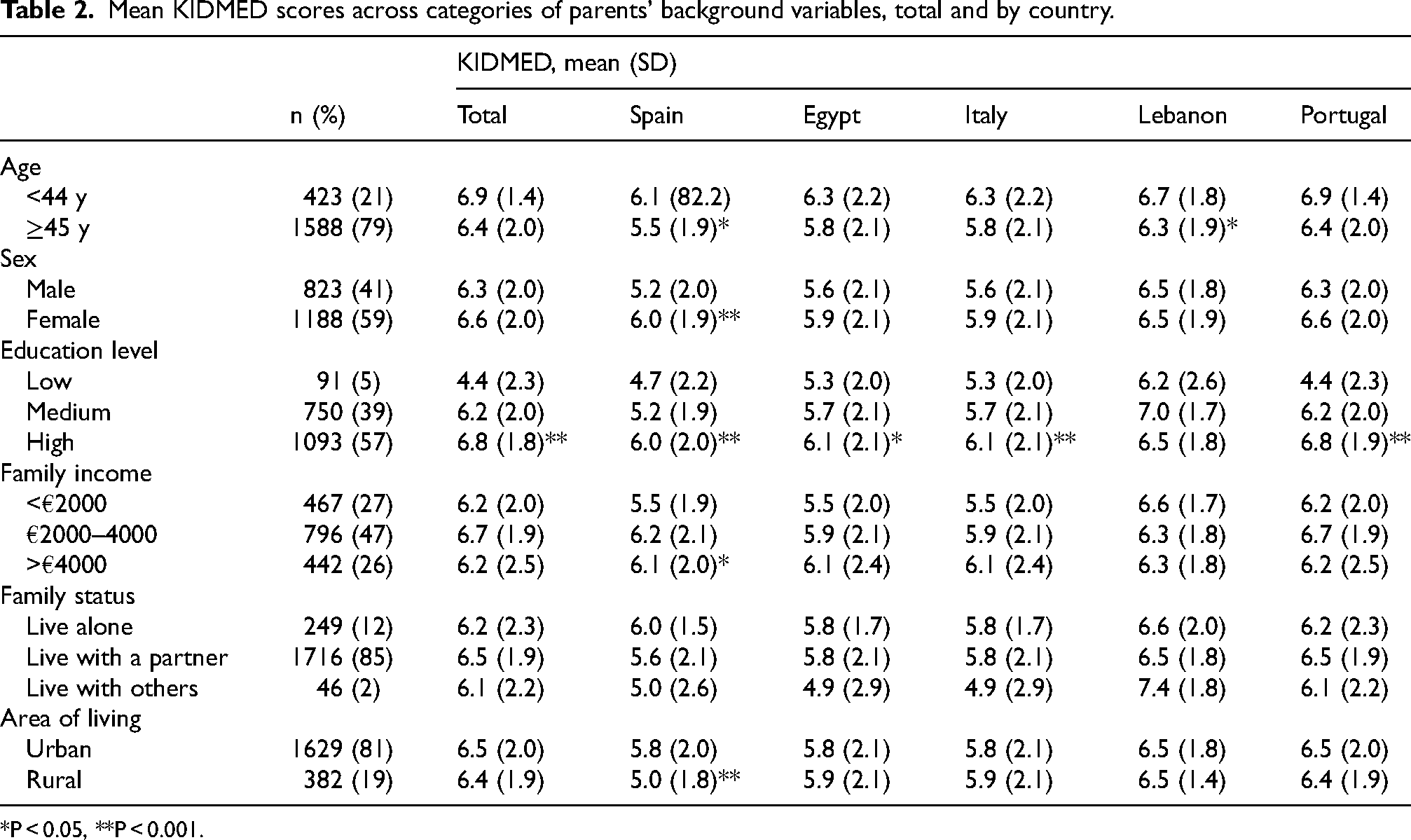
*P < 0.05, **P < 0.001.
Discussion
The present study described the status of Mediterranean diet adherence in children and adolescents living in 5 Mediterranean countries. The results from this study showed some differences in the level of adherence to the Mediterranean diet, with children and adolescents living in Lebanon and Portugal more adherent than their counterparts in other countries. Additional aspects related to Mediterranean diet adherence elucidated from this survey include the adoption of specific characteristics in line with traditional dietary habits in the Mediterranean area, such as olive oil consumption and daily fruit and vegetable intake, as well as lifestyle habits including having breakfast and limit sweets, while underscoring substantial abandonment of certain other Mediterranean diet features, including having a second portion of fruit and vegetable, adequate consumption of fish, nuts, and cereals (for breakfast), as well as frequent consumption of fast foods. Some background factors were also explored to potentially be related with higher Mediterranean diet adherence scores.
In a broad multi-national context, several studies showed a decrease in Mediterranean diet adherence in Mediterranean countries. 38 The overall decline in Mediterranean diet adherence over recent years has been noted, even in countries like Spain and Italy, where this diet is part of the cultural heritage. Age seems to be a factor strongly affecting such trends, being younger individuals more likely to have lower adherence to this traditional dietary pattern compared to older ones, as studies indicate that Mediterranean diet adherence is often moderate-to-low among children and adolescents living in the Mediterranean area. 39 The shift towards more Westernized eating patterns, characterized by higher consumption of processed foods and sugary beverages, has been hypothesized to have played a significant role in this decline.40–42 Moreover, recent reports have shown a worsening in Mediterranean diet adherence rates in light of the negative impacts from the COVID-19 pandemic. 43 The COVID-19 pandemic significantly affected dietary habits and lifestyle behaviors among children and adolescents. Lockdowns and school closures disrupted regular meal patterns and physical activities, contributing to increased screen time and sedentary behavior. 44 These changes adversely impacted dietary habits, as evidenced by several studies reporting decreased Mediterranean diet adherence during the pandemic period, although with some contrasting results depending on the setting and background characteristics.45–48 Several reports specifically conducted on children and adolescents during the COVID-19 pandemic found a notable decline in adherence to the Mediterranean diet among adolescents, attributed to increased consumption of snacks and sugary foods and reduced physical activity due to lockdown measures.49–53 These findings highlight the importance of stable routines and the role of structured environments like schools in maintaining healthy dietary habits.
With concern to specific elements characteristics of the Mediterranean diet, olive oil consumption and daily fruit and vegetable intake have been found to be rather common among children and adolescents in all countries. Although potentially reassuring, this finding probably reflects a higher availability of such foods and their common use in traditional diets in the countries involved in the survey, while the overall consumption of both fruit and vegetables may still result relatively low, since only half children and adolescents were reported consuming a second serving per day. These results are quite in line with previous studies reporting a substantially inadequate intake of fruit and vegetables among children and adolescents living in the Mediterranean region.54–56 On the other hand, some specific aspects related to the Mediterranean diet have been emphasized as of potential concern, including low frequency of children and adolescents having dairy and cereals for breakfast (especially in Egypt and Italy), having weekly fast-food and regular fish (especially Spain), and relatively scarce legume consumption (equally observed in all countries). These findings remark the general trends observed in the last years concerning the aforementioned food groups, confirming a consistent evidence of adoption of unhealthy dietary behaviors. 57 As previously mentioned, it may be hypothesized that industrially produced foods, not necessarily healthy and nutritious, may have a stronger appeal on younger generations as compared with older ones, 58 leading to their preference over more traditional, less processed foods characteristic of the Mediterranean diet. The concerns on the so-called “ultra-processed” foods and the resulting nutrition transition in Mediterranean countries with the “Westernization” of traditional diets are of public health domain: the discussion on this matter is currently ongoing and data in support of such evidence is needed to better understand the best targets for potential interventions.
In this study, also an attempt to test whether the mean KIDMED scores would be significantly different in groups based on background and lifestyle variables was conducted. Younger children with adequate sleep duration, shorter screen time, and higher physical activity were reported to have higher Mediterranean diet adherence scores. Similarly, children of younger female (respondent) parents with higher educational level, family income, and living in urban areas were also reported to have higher scores. Several studies explored factors potentially associated with higher adherence to the Mediterranean diet with healthy lifestyles reported to cluster with each other, possibly depending on factors related to parents and family.59–61 It may be hypothesized that all such variables may be related, hence not representing individual determinants of adherence to the Mediterranean diet, but rather an unique single construct. 62 Although hypothesized in previous studies, further in depth analyses are needed to further elucidate such potential framework.
Some limitations of the present study should be listed in order to fully consider the findings reported. First, the data presented has been reported by parents, hence potentially being affected by recall bias, social desirability bias, or simply lack of valid knowledge concerning their children's dietary habits (however rather limited to the older ones, eventually). Second, data relied on frequency of consumption, but no information concerning portion size was retrieved; thus, one cannot exclude that portions were substantially inadequate (in excess or defect) and did not effectively reflect a proper adherence to the Mediterranean Diet. However, the instrument such the KIDMED is not built to identify quantitative data in terms of portions, hence it is supposed to maintain its validity also in such types of studies. Third, survey respondents may not be truly representative of the target population; however, the study is methodologically in line with previously published reports, furthermore it includes harmonized information on five countries, and additionally provides information eventually poorly explored or not updated for some of them (i.e., Egypt). Concerning the tool used to assess the level of adherence to the Mediterranean diet, although the KIDMED is the most widely used, such instruments may not fully capture potential unmeasured key components of this dietary pattern and under or overestimate the adherence rate. Finally, the IPAQ short form has been validated for both young and adults, but its validity on children remains untested. However, the tool was not used to calculate complex and specific measures of physical activity (i.e., metabolic equivalents) but only to rank the level of activity in general groups.
In conclusion, the current status of adherence to the Mediterranean diet is not encouraging, showing a relatively average adherence rate that can be deemed as suboptimal considering the geographical area of interest. While some traditional elements are almost fully retained even nowadays (i.e., olive oil consumption), the growing impact of modern society, providing unhealthy yet more appealing or convenient food alternatives, is gradually leading to a change of preferences and an abandonment of the adoption of a Mediterranean diet. Notably, the food groups that seem to suffer more to be consumed are fruit and vegetables, whole grains, and legumes. Future efforts should be made to promote intervention studies aiming to increase the level of diet quality among younger generations and encourage adoption of healthy, traditional dietary patterns, such as the Mediterranean diet itself. Additionally, research exploring the impact of digital interventions, such as mobile apps and online education programs, on improving dietary habits can offer innovative solutions to reach wider audiences.
Footnotes
Author contributions
A.R., P.B., and G.G. designed the study, G.G. performed analyses. A.R., F.S., F.G. and G.G. interpreted the data. A.R. and F.S. wrote the article. All authors provided critical revision of the manuscript. All authors have read and agreed to the final version of the manuscript.
Funding
The DELICIOUS project is funded by the PRIMA programme supported by the European Union [Grant Agreement No. 2131].
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.