
Abstract
Introduction
The Mediterranean Diet (MD) is widely recognized for its numerous health benefits, 1 including reduced risks of cardiovascular disease, 2 improved cognitive functioning, 3 lower prevalence of metabolic disorders, 4 decreased incidence of certain cancers, 5 and reduced overall mortality. 6 Consequently, it is actively promoted by health organizations worldwide. 7 Paradoxically, adherence to the MD is declining in countries where it originated, 8 raising concerns about both public health and the erosion of cultural and culinary heritage. 9 To preserve and revitalize MD adherence in Mediterranean countries, it is important to understand the multifaceted determinants that drive this behavior; however, such insight remains limited, especially in Middle Eastern Mediterranean contexts. 10
Existing evidence from European Mediterranean countries show that the complex interplay of factors influencing MD adherence can be systematically examined using the Socio-Ecological Model (SEM). 11 This framework emphasizes the dynamic interactions between individual, interpersonal, community, and societal-level determinants, 8 offering a comprehensive perspective on drivers of dietary behaviors.
At the individual level, determinants such as health literacy, nutrition-related knowledge, and personal beliefs shape dietary choices according to the SEM. 12 Cross-sectional studies from Spain and Italy consistently show that higher nutrition knowledge is associated with greater MD adherence, as individuals who understand its health benefits are more likely to follow its principles.13–15 In addition, dietary habits like regular breakfast consumption and mindful eating have been positively associated with MD adherence in Southern European populations.3,4 Socio-economic factors—including income, employment status, and financial security—have also emerged as key predictors, especially during times of economic hardship.13,16 However, socio-cognitive determinants of MD adherence such as attitudes, beliefs, emotional support, and social connections remain underexplored, particularly in Middle Eastern Mediterranean countries. 17 Qualitative studies in Greece highlight the critical role of family traditions, peer support, and shared meals in fostering MD adherence and preserving cultural food heritage. 18 In Italy and Spain, observational studies similarly show that strong family ties and culturally embedded food rituals act as protective factors against dietary westernization.19,20 Yet, there is limited empirical research examining how these socio-cognitive processes influence MD adherence in Middle Eastern Mediterranean settings.13,21
At the community and environmental level, factors such as food accessibility, affordability, and the local food environment are pivotal. 22 Systematic reviews indicate that access to food products that fit within the MD, proximity to traditional markets, and the preservation of rural agricultural systems are associated with higher MD adherence. 17 Conversely, urbanization and the shift towards modern food environments promote Western dietary patterns, characterized by increased consumption of ultra-processed foods and reduced intake of MD staple foods. 23 While these dynamics are well-documented for Southern Europe, they remain insufficiently studied in the Middle Eastern Mediterranean context. 13 Moreover, macro level factors such as globalization, dietary westernization, and economic crises have been found to critically influence MD adherence. 22 Longitudinal studies from Greece, Spain, and Italy have shown that economic downturns are linked to declining MD adherence, primarily due to the reduced affordability of essential MD components like fresh vegetables, fruits, fish, and olive oil.24,25 However, the shift towards ultra-processed foods, not traditionally part of the MD, is not solely driven by price, indicating that other socio-economic and cultural factors contribute to these dietary changes. 26
Lebanon, a Middle Eastern Mediterranean country with a rich culinary heritage rooted in the MD, has been severely impacted by an ongoing economic crisis. Since 2019, the country has faced an economic collapse, marked by an 80% currency devaluation, banking sector paralysis, and a 183% surge in food prices. 27 These disruptions have exacerbated food insecurity and significantly altered dietary habits. 28 While Lebanese adults demonstrated medium-to-high MD adherence prior to the crisis, recent surveys reveal a notable decline. 29 There is a paucity of research examining how such socio-economic disruptions interact with individual, social, and environmental determinants to influence MD adherence in Lebanon and the broader Middle Eastern Mediterranean region.
Therefore, this study aims to investigate the key determinants of MD adherence among Lebanese adults during the economic crisis, with a specific focus on socio-cognitive and social and economic environmental factors. Guided by the SEM, this research seeks to provide a comprehensive understanding of how individual, social, and environmental influences collectively shape MD adherence among Lebanese adults.
Materials and methods
Design
This was a cross-sectional study, conducted between November 2023 and January 2024. A convenience sampling method was employed using an online questionnaire in both Arabic and English. The research ethics committee at Notre Dame University-Louaize (NDU) (Institutional Review Board at NDU) approved the study protocol (IRB# 202247).
Participants and recruitment
The target population consisted of healthy adults aged 18 and above, residing in Lebanon for over 10 years, and free from nutrition-related diseases such as diabetes, cardiovascular diseases and cancer. Using “Calculator.net,” a target sample size of 270 participants was determined to assess the association between various determinants and MD adherence based on an assumed medium effect size (Cohen's w = 0.3).30,31
An informational letter, including a link to the questionnaire, was disseminated in public spaces (gyms and supermarkets). Participants were further recruited through announcements on the social media platforms of the Lebanese investigators and the official platforms of NDU, such as WhatsApp, Facebook, LinkedIn, and Instagram. An informational message about the study, including a link to the questionnaire, was posted on these platforms and announced five times. To enhance participant diversity and expand reach, the announcements were also shared with students enrolled in liberal arts curriculum classes at NDU, as this group includes students from a variety of majors beyond health-related fields. The link was also distributed via WhatsApp groups of school alumni of the Lebanese investigators. Furthermore, a snowball sampling approach was implemented, where initial participants were encouraged to share the questionnaire link within their personal and professional networks.
Prior to participation, an informed consent procedure was implemented, using Google Forms. Participants were presented with a link that redirected them to the information sheet detailing the study's purpose, confidentiality, voluntary participation and the contact details of the primary investigator. Informed consent was obtained electronically by clicking an ‘I Agree’ button, which provided access to the questionnaire. Eligibility criteria were assessed through initial screening questions at the start of the online questionnaire. Participants who did not meet these criteria were automatically redirected towards a page indicating that they could not participate and were not enrolled as participants.
Questionnaire
Data was collected via an online self-administered survey available in both English and Arabic. The survey contained 70 questions divided into four main sections: socio-demographic variables, adherence to the MD, socio-cognitive determinants and social and economic environmental determinants.
Socio-demographic variables
The survey began with a section of 13 questions designed to collect socio-demographic data. Participants were asked to provide their age (in years), gender (male/female), and height (in cm) and weight (in kg) to calculate BMI (
14-item Mediterranean diet adherence screener (14-MEDAS)
The validated 14-item Mediterranean Diet Adherence Screener (14-MEDAS), derived from the PREDIMED (Prevention with MD) study, 31 was utilized to assess adherence to the MD. The tool includes nine items focused on the frequency and number of servings of cardioprotective elements commonly found in the MD, such as vegetables, fruits, whole grains, fish, legumes, and olive oil. Additional questions addressed the consumption of meat and meat products, fat servings, food habits, and the intake of specific items such as nuts, soda drinks, and “sofrito” (a traditional Mediterranean sauce made from tomato, garlic, onion, and olive oil). Participants were asked to respond to each of the 14 items in the MEDAS by reporting the number of servings they typically consumed of the specified food items, reflecting their usual dietary habits. Responses were then scored to calculate the MEDAS score. Each question was assigned a score of 0 or 1 based on predefined adherence criteria: a score of 1 was given if the participant's response aligned with the recommended MD guidelines (e.g., consuming ≥2 servings of vegetables per day or using olive oil as the primary fat for cooking). Conversely, a score of 0 was assigned if the response did not meet the adherence criteria (e.g., consuming <2 servings of vegetables per day or not using olive oil for cooking). The scores from all 14 questions were summed to produce the MD adherence score, which ranged from 0 to 14, with higher scores indicating greater adherence to the MD. 31
A brief explanation of the MD principles was provided after completing the 14-MEDAS, to avoid influencing the assessment of MD adherence, but before the questions on socio-cognitive and environmental variables, ensuring that participants fully understood the MD concept regardless of their level of adherence. The explanation used to explain MD principles is provided as supplementary material.
Determinants of MD adherence
The potential determinants of adherence to the MD were examined within the framework of the SEM. 11 Socio-cognitive factors were assessed through a set of 16 items rated on a 5-point Likert scale, including cognitive and affective attitude beliefs (9 items), intention (1 item), knowledge (1 item), subjective norms (3 items) and perceived behavioral control (2 items). Additionally, the food environment was evaluated using 27 questions addressing key aspects of the social and economic environment (7 items), food availability (11 items), food accessibility (7 items) and food affordability (2 items). Further details on the assessment measures and answering options are provided in Table 1. The questionnaire items were developed for the current study based on constructs from the Theory of Planned Behavior (TPB), 32 a widely used theoretical framework in health behavior research.
Determinants of the Mediterranean diet: concepts, items, and response scales.
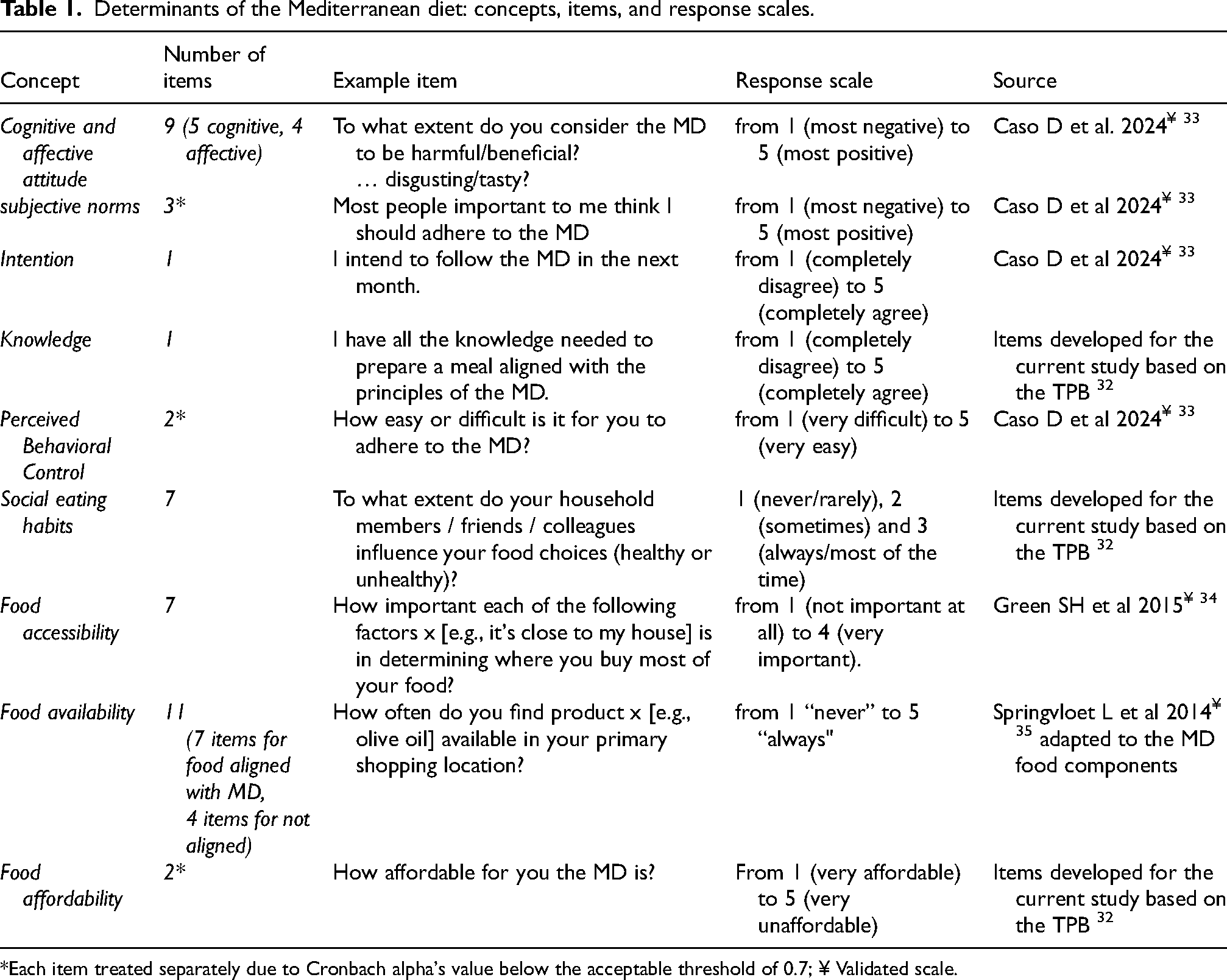
*Each item treated separately due to Cronbach alpha's value below the acceptable threshold of 0.7; ¥ Validated scale.
Statistical analysis
As a first step in the data analysis, the quality of questionnaire completion was assessed. The cognitive-affective attitude items were found to exhibit repetitive response patterns and a high proportion of missing data, with around 57% of participants selecting identical responses across items and approximately 7% leaving items unanswered. Due to potential unreliability of the responses, we decided to exclude the attitude items from the analyses.
Categorical variables in the socio-demographic section were summarized using proportions, while quantitative variables were described using means and standard deviation to reflect central tendency and variability.
The MEDAS adherence score was first described using mean and standard deviation. To assess the normality of the adherence score, skewness and kurtosis values were examined alongside visual inspection using a histogram. Additionally, formal normality tests, including the Kolmogorov-Smirnov and Shapiro-Wilk tests, were conducted to ensure the data's distribution met the assumptions for parametric testing. Despite significant results from the Kolmogorov-Smirnov and Shapiro-Wilk tests (p < 0.001), the distribution of the adherence score was considered approximately normal based on the large sample size, near-zero skewness (−0.154) and kurtosis (−0.145), and the histogram's alignment with a normal distribution. In addition, the adherence score was categorized into three levels of adherence: low adherence (scores up to 5), moderate adherence (scores between 6 and 9) and high adherence (scores of 10 and above). 31 Regarding determinants of adherence, scores for each concept were calculated when applicable and described using means and standard deviations. All other variables were also described using means and standard deviations.
To assess bivariate associations between the MD adherence score and potential determinants, the student's t-test was used to examine relationships with binary categorical variables, including gender (males/females), place of residence (urban/rural), field of work (health/non-health) and having children (yes/no). A one-way ANOVA test evaluated adherence in relation to categorical variables with at least three categories: employment status (not employed/ employed full time/ employed part time) and income before and after the crisis (< 450 USD/ 450–800 USD/ 800–1300 USD/ 1300–2000 USD/≥ 2000 USD). Pearson correlations were used to analyze the correlation between MD adherence and age, BMI calculated through height (m2) and weight (Kg), household size, number of children and all socio-cognitive and environmental variables.
A multiple linear regression analysis was conducted to assess the associations of the various categories of determinants with adherence to the MD. The results were presented as standardized regression coefficients (β) and unstandardized regression coefficients (β) and their corresponding 95% confidence intervals (Cl). P-values less than 0.05 were considered statistically significant in all models, indicating meaningful associations between the predictors and the adherence score. All statistical analyses were performed using IBM SPSS version 29 (SPSS Inc., Chicago, IL, USA).
Results
Initially, 337 individuals expressed interest in completing the survey, completed in English (n = 212) or Arabic (n = 125). After applying the eligibility criteria at the start of the questionnaire, 304 eligible participants were able to proceed and were included in the final sample.
Socio-demographic characteristics
Table 2 presents the socio-demographic characteristics of participants. The sample had a mean age of 33.3 ± 11.2 years and a mean BMI of 24.2 ± 4.2 kg/m². The majority of participants were female (74.7%), with 64.0% living in urban areas. Educational attainment was high, with 40.0% holding a bachelor's degree and 38.6% a master's degree. About half were employed full-time, and 56.3% worked in non-health-related fields, while 30.0% were unemployed. Nearly half (49.8%) were married or in a domestic partnership, and 54.1% had children.
Characteristics of the sample (n = 304).
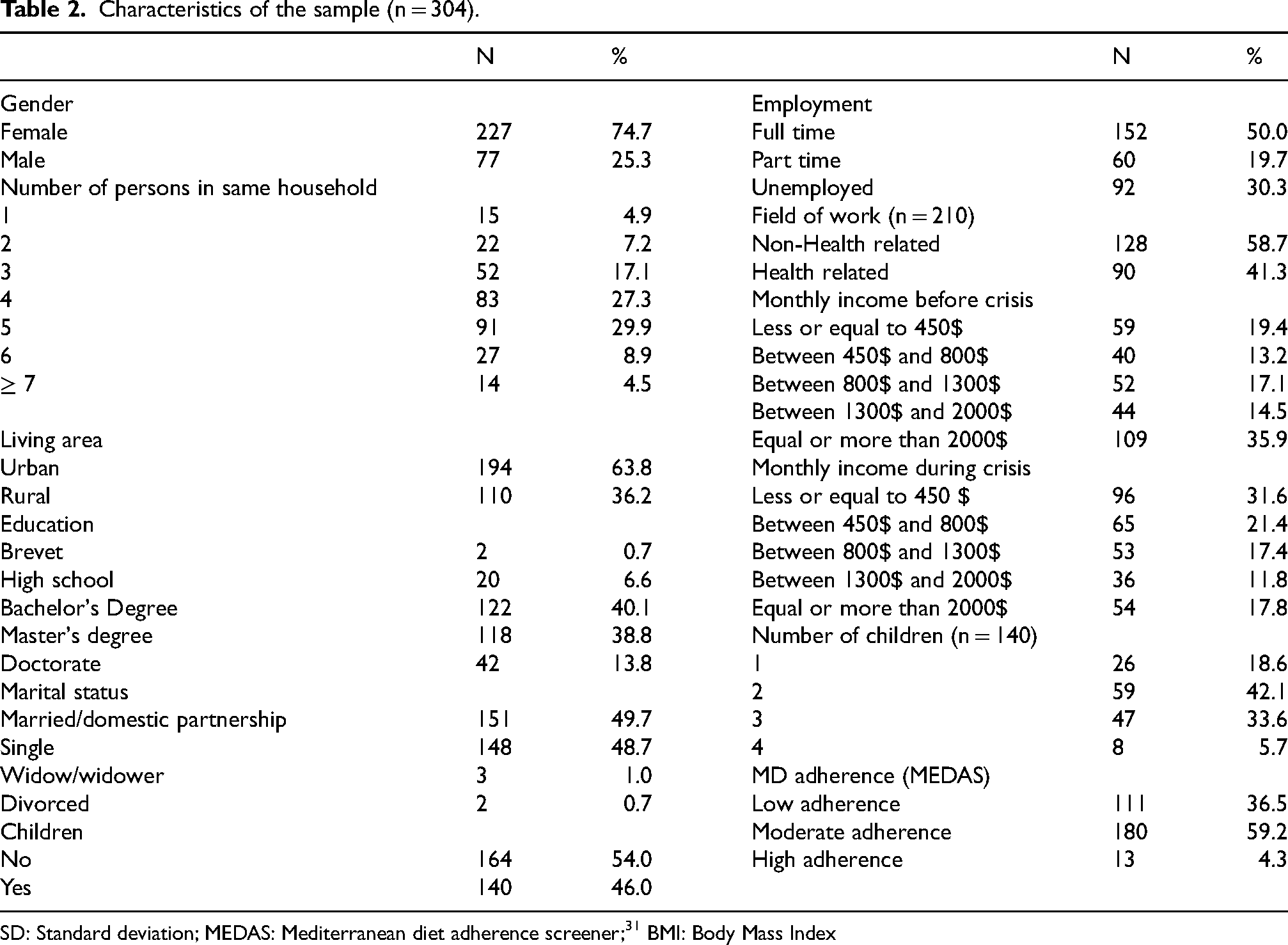
SD: Standard deviation; MEDAS: Mediterranean diet adherence screener; 31 BMI: Body Mass Index
Adherence to the MD was generally low to moderate. The mean MEDAS adherence score was 5.9 ± 2.0 (scale 0-14), the lowest score was 1 and the highest was 11, with 59.2% of participants showing moderate adherence (score 6–9) and only 4.3% exhibiting high adherence (score ≥10).
Bivariate analysis of correlates of MD adherence
MD adherence scores differed by gender and work field
Bivariate analysis of MD adherence by socio demographic variables (n = 304).
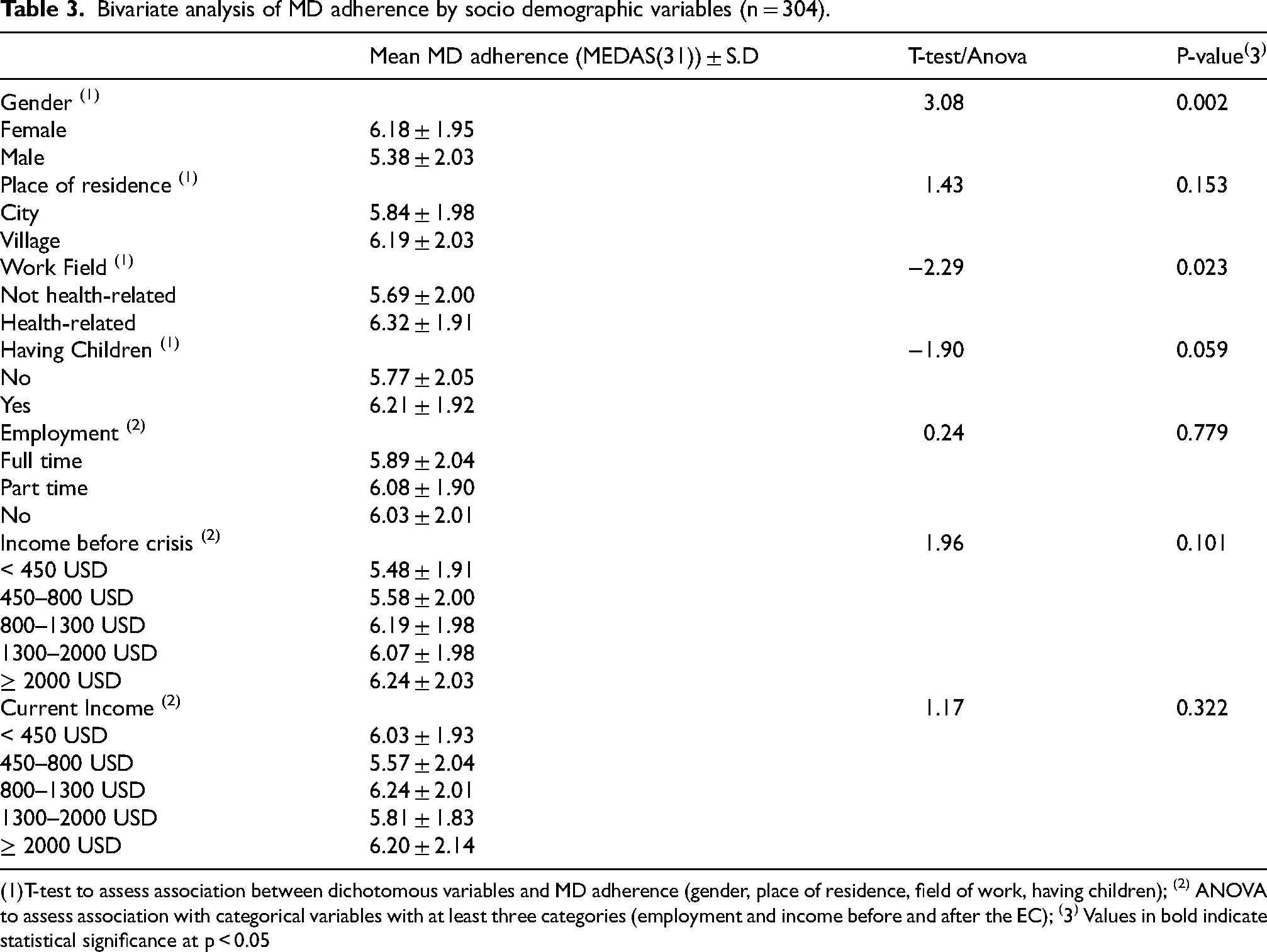
T-test to assess association between dichotomous variables and MD adherence (gender, place of residence, field of work, having children); (2) ANOVA to assess association with categorical variables with at least three categories (employment and income before and after the EC); (3) Values in bold indicate statistical significance at p < 0.05
Intention, descriptive norm, perceived ease of following the MD, and knowledge showed significant positive correlations with adherence to the MD (p < 0.001). Tradition and the availability of MD-aligned foods also exhibited weaker but significant associations (p < 0.05). In contrast, perceived affordability, store access, and perceived price were not significantly correlated. Further details are presented in Table 4.
Bivariate analysis of mean scores of potential determinants and their correlations with MD adherence score (31) (n = 304).
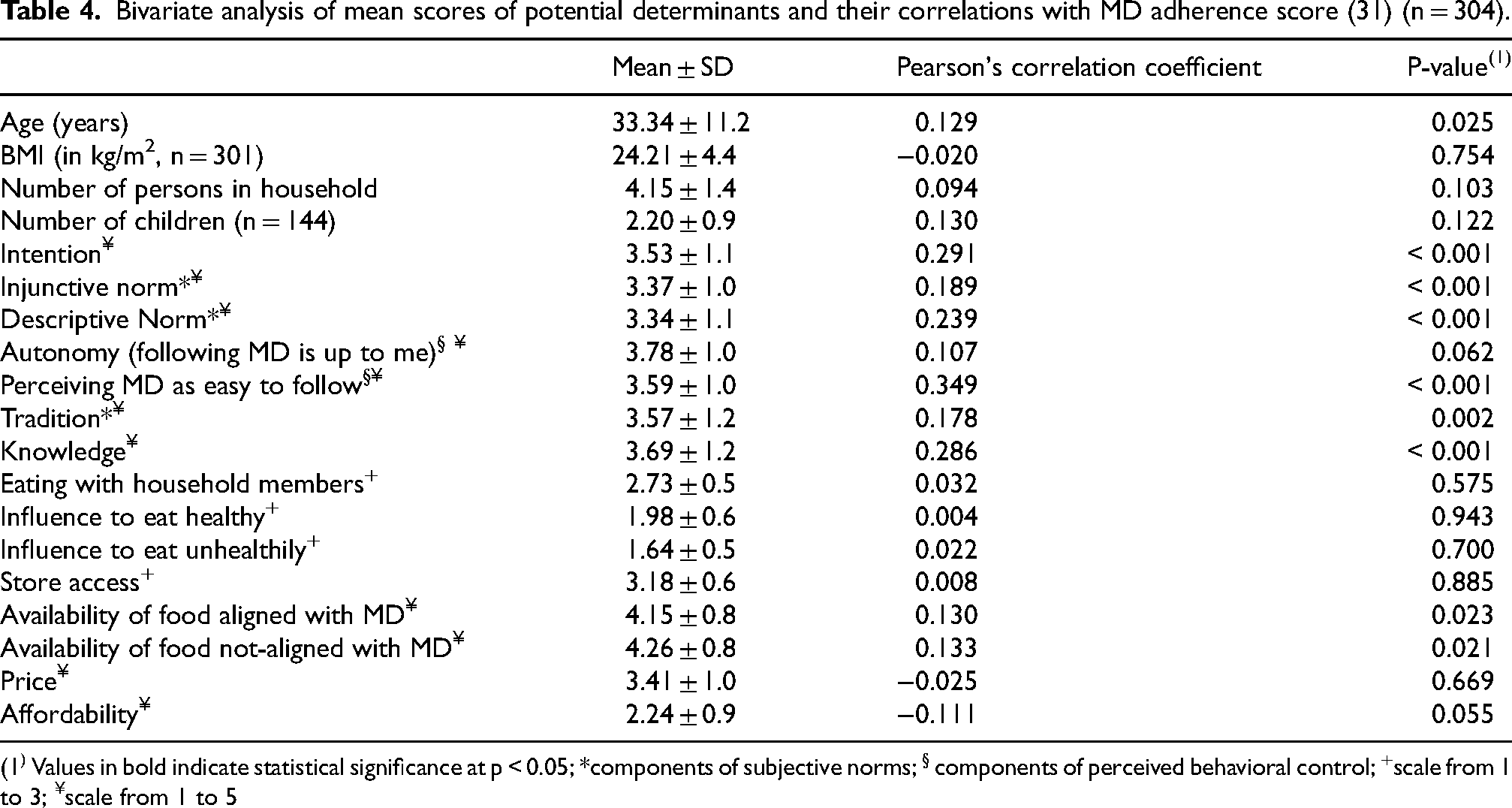
1) Values in bold indicate statistical significance at p < 0.05; *components of subjective norms; § components of perceived behavioral control; +scale from 1 to 3; ¥scale from 1 to 5
Multiple regression analysis of potential determinants associated with MD adherence
A multiple regression analysis was conducted to identify key factors associated with MD adherence. The results indicated that among the examined predictors, perceived ease in adhering to the MD emerged as the strongest and only statistically significant factor (standardized β = 0.23; p = 0.002). Further details are presented in Table 5.
Multiple regression analysis of factors associated with MD adherence (n = 301).
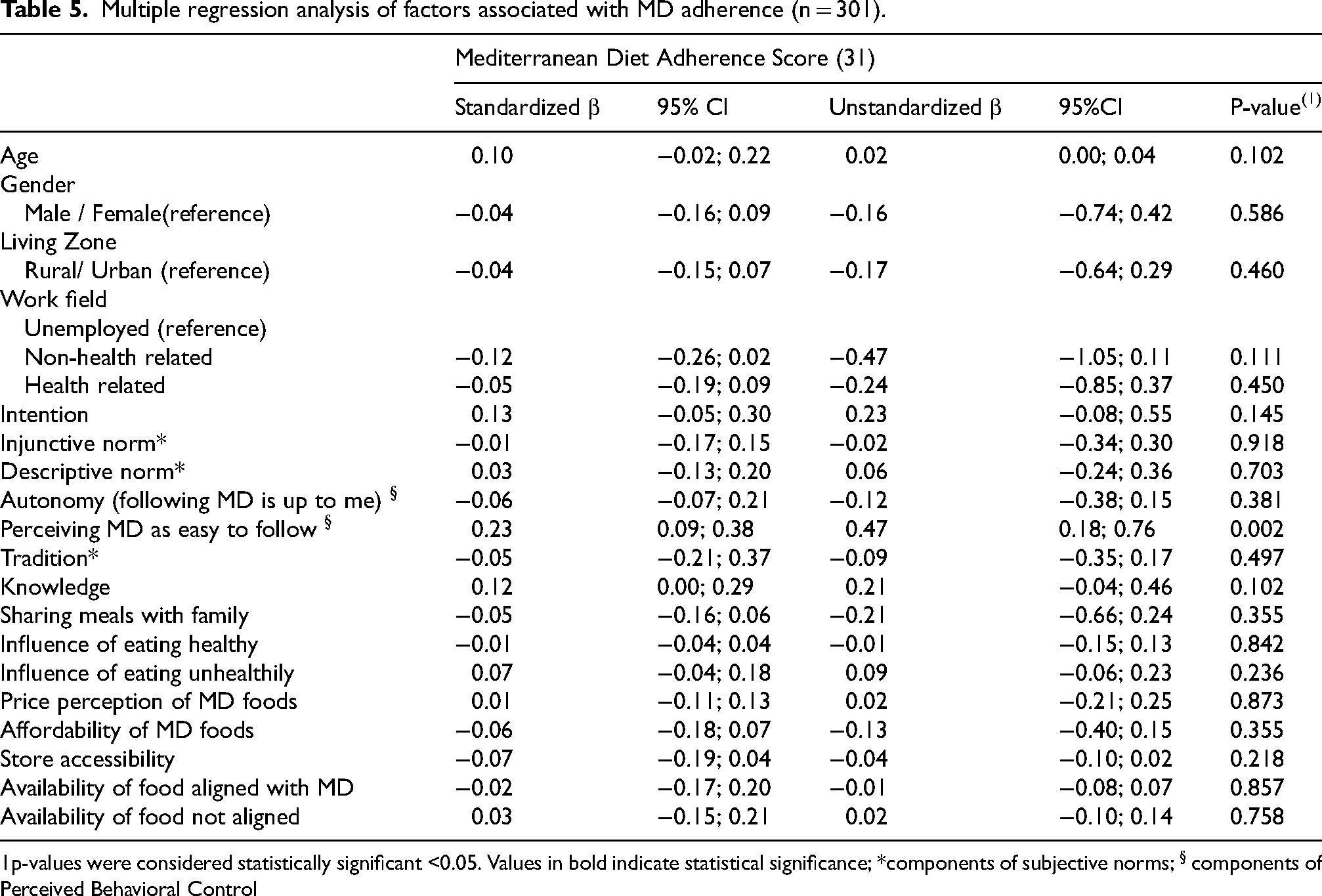
p-values were considered statistically significant <0.05. Values in bold indicate statistical significance; *components of subjective norms; § components of Perceived Behavioral Control
Discussion
This study aimed to investigate the key factors associated with adherence to MD among Lebanese adults during the economic crisis, with a specific focus on socio-cognitive and environmental factors. The participants in our study showed generally low to moderate adherence to the MD, with a mean MEDAS adherence score of 5.97 ± 2.0 (scale: 0-14). Only a small proportion (4.3%) had high adherence. These findings align with other studies in Lebanon and other Middle Eastern Mediterranean countries, which have documented low to moderate adherence to the MD due to the increasing adoption of Westernized diets and ongoing socio-political stressors 28,36,37 In particular, Nasreddine et al. (2021) documented a dietary shift away from the MD in favor of processed and fast foods. 36 Given that our study was conducted during an economic crisis characterized by soaring food prices, loss of income, 27 and food insecurity, 38 the low adherence observed may reflect the challenging socioeconomic conditions at the time. While some evidence — including our previous qualitative study in Lebanese adults — suggests that people may turn to more traditional dietary patterns during economic hardship due to limited access to imported foods, 16 such changes may not necessarily lead to improved overall adherence to the MD, which requires diversity, balance, and regularity in dietary intake. 9 To better understand the drivers of MD adherence, we examined potential determinants of MD adherence. Grounded in socio-cognitive theory and informed by our earlier qualitative research, 16 we hypothesized that attitudes, perceived behavioral control of following the MD and environmental-level factors would be associated with MD adherence. However, our findings only partially supported these expectations: among the examined factors, only perceiving MD as easy to follow, as part of perceived behavioral control, was significantly associated with MD adherence.
On the Individual-level, while certain sociodemographic factors, such as gender, initially appeared to be associated with MD adherence in the correlation analysis, these associations did not hold in the multiple regression analysis. Instead, only perceived ease of following the MD remained a significant predictor, suggesting that psychological factors, particularly individuals’ sense of control over their dietary choices, play a more central role than demographic characteristics in shaping adherence behavior. 39 The findings show an association between perceived behavioral control and higher adherence to the MD. However, it is also possible that individuals who already adhere to the diet perceive it as easier to follow, or that they have better skills to manage these barriers. 40 Nonetheless, perceived behavioral control could be an important factor to address in interventions. Similar results have been reported in other countries. For instance, among Iranian and Moroccan adults, self-efficacy (which is similar to perceived behavioral control of following the MD) and perceived ease of healthy eating were identified as strong predictors of dietary adherence.41,42 These studies also found that the perception of control often outweighed knowledge or attitudes in influencing behavior,41,42 which is in line with our finding that knowledge was not significantly related to adherence in the multiple regression analysis. Feeling in control seems particularly critical in crisis settings like the current Lebanese context, where external constraints may feel overwhelming. 43 It also suggests that interventions aimed at improving adherence should prioritize enhancing perceived control of following the MD, through — through skill-building, meal planning, coping planning (i.e., anticipating and managing potential barriers), or affordable recipe guidance — and by increasing the availability and accessibility of MD products, 32 rather than relying solely on knowledge dissemination.
Although attitude was initially included as a potential determinant of MD adherence, it was excluded from the analysis due to limited response variability, likely caused by repetitive patterns. This prevented assessment of a construct widely recognized as a key predictor of dietary behavior.16,44 Prior studies and our qualitative research highlight attitude—especially beliefs about health benefits and taste—as a major influence on MD adherence.16,45,46 Future research should therefore ensure robust measurement of attitude, particularly in crisis contexts where other factors may be less impactful.
Interpersonal factors—such as family meal frequency and social support—were not significant predictors of MD adherence in our multivariate analysis, contrasting with findings from another Middle Eastern study linking these factors to healthier eating, 47 as well as our prior qualitative research in Lebanon, highlighting the influence of family and social networks on food choices. 16 This discrepancy may stem from differences in measurement tools. Our current study used simple quantitative indicators that might have failed to capture the complexity of cultural and social food dynamics, whereas other studies employed more comprehensive, culturally sensitive methods. 48 Future research should use more culturally tailored and nuanced approaches, including qualitative or mixed methods, to better assess social influences—especially during crises when routines and roles may shift. Without such tools, the true impact of interpersonal dynamics on dietary behavior may be underestimated. 49
On the environmental level, variables such as affordability, store access, and availability of MD-compatible foods were not significant predictors of adherence. This diverges from findings in other Mediterranean countries, where affordability and food access were among the top reported barriers to MD adherence.23,50 It is possible that our environmental items did not fully capture the dynamic and severe constraints experienced by Lebanese households during this period of economic collapse, including informal food markets and currency devaluation. 51 Moreover, given the sociodemographic profile of our sample, these null associations may reflect selection rather than absence of effect; affordability and access could still meaningfully constrain adherence among less affluent or otherwise under-resourced groups. 17 Thus, our findings should not be generalized to populations with different socioeconomic characteristics, and future work should test these relationships in more diverse samples (e.g., stratified by income/education) to assess potential effect heterogeneity. Alternatively, the overwhelming presence of structural constraints in the Lebanese context may have normalized these barriers across the sample, 52 reducing variability in responses and thus statistical associations. Another explanation is that, even when food is available, people may still not perceive themselves as able to prepare or consume it regularly 53 —again emphasizing the role of perceived control. Importantly, this constraint on perceived control is often sharper among less affluent or lower-educated groups—and may vary by gender—because financial limits, time scarcity, and fewer cooking resources make it harder to translate availability into regular consumption. 54
Together, these findings highlight the potential role of perceived behavioral control of following the MD as a motivational factor associated with MD adherence, particularly during periods of economic crisis. They also suggest that despite positive intentions, individuals may face challenges in consistently translating these intentions into actual dietary behavior, underscoring the importance of supporting people in overcoming such challenges. 55 For practice, interventions should focus on enhancing individuals’ capacity to follow the MD, for example simplifying meal preparation and addressing financial or time constraints. 55 Future research should adapt and validate culturally relevant, reliable tools, such as those to assess socio-cognitive determinants, 32 specifically for the Lebanese context. The limited validity of the assessed constructs may have contributed to inconclusive findings. 56 Studies should also use more representative samples, as well as longitudinal and qualitative designs are needed to explore how perceived ease of following the MD interacts with socio-economic factors to influence dietary adherence over time. 57
This study has several strengths, including bilingual administration, and integration of socio-cognitive, interpersonal, and environmental variables guided by the Theory of Planned Behavior. 32 It is also the first to quantitatively assess MD adherence determinants in Lebanon within the unique context of a national economic crisis. Nonetheless, limitations must be considered. The cross-sectional design limits causal interpretation, and the use of self-reported data may introduce social desirability or recall bias.58,59 Another limitation is the non-probability sampling, which yielded a sample composed predominantly of young, university-educated women (over 90% with tertiary education), recruited through convenience and snowball sampling. These strategies—based on online dissemination within our (professional) networks and participant referrals—likely over-sampled digitally connected, health-interested participants and led to under-representation of men, older adults, and lower-education/SES groups. Because education and socioeconomic status are known correlates of MD adherence, 17 this composition may inflate average adherence in our sample and attenuate or distort associations between the study predictors and MD adherence, by restricting variance on key covariates. Findings should therefore be interpreted as exploratory and not population-representative, and future studies should use probability or quota sampling with mixed-mode recruitment to better capture under-represented groups. A major limitation of this study was the exclusion of the attitude component from the analysis. Although assessing attitudes towards the MD was one of the study's primary objectives, the attitude items showed poor response quality (straight-lining/repetitive patterns and substantial missing data), which prevented reliable scoring. Questionnaire design factors—particularly the ordering and layout of the attitude block—may have induced respondent fatigue and satisficing (e.g., straight-lining), especially on mobile devices. Consequently, we removed the attitude component from the final statistical models. This reduces the comprehensiveness of our findings and limits the robustness of the regression analyses, given that attitude is central in the Theory of Planned Behavior 32 and has been linked to dietary behaviors in prior research.59,60 Moreover, several questionnaires were translated/adapted for this study without a full cultural-linguistic validation process. As a result, internal consistency, test–retest reliability and construct validity could not be comprehensively confirmed in our sample. This raises the possibility of measurement error that could attenuate or bias estimated associations. Future research should follow rigorous cross-cultural adaptation procedures (forward–back translation, expert review, cognitive interviewing, pilot testing) and evaluate reliability and validity before deployment. Finally, while multiple testing can increase the chance of false positives, 61 it does not explain the lack of significance for other variables. Perceived ease of following the MD consistently emerged as a significant determinant of MD adherence in both unadjusted and adjusted models, remaining robust even under correction for multiple testing.
Conclusion
This study identified perceived ease of following the MD, a component of perceived behavioral control, as the most important correlate of adherence to the MD among Lebanese adults during a period of severe economic crisis. Despite expectations drawn from socio-cognitive theory and previous research, other individual, interpersonal, and environmental factors—such as knowledge, intention, social support, and food access—did not significantly predict adherence in a multiple regression model. These findings suggest that, in crisis settings, the perceived ease of following the MD outweighs other motivational or informational factors. Interventions should therefore prioritize strengthening individuals’ perceived control through context-sensitive strategies such as skill-building, meal planning support, coping planning and access to affordable MD options. Further research using longitudinal studies using validated instruments to assess potential determinants is needed to explore how perceived control interacts with broader socio-economic conditions to shape dietary behavior.
Supplemental Material
sj-docx-1-mnm-10.1177_1973798X251385498 - Supplemental material for Associates of adherence to the Mediterranean diet among Lebanese adults: A cross sectional study
Supplemental material, sj-docx-1-mnm-10.1177_1973798X251385498 for Associates of adherence to the Mediterranean diet among Lebanese adults: A cross sectional study by Cécile Obeid, Jessica S. Gubbels, Julia Bou Dib, Antoine Aoun, Stef PJ Kremers and Anke Oenema in Mediterranean Journal of Nutrition and Metabolism
Footnotes
Acknowledgments
We would like to express our sincere gratitude to Nancy Trezia and Reina Naaman for their valuable assistance in uploading the questionnaire on Google Forms and for their support in participant recruitment. We also extend our heartfelt thanks to all participants for their time and willingness to take part in this study. Their participation and responses were essential to the success of this research.
Ethical considerations
This study was approved by the Institutional Review Board (IRB) at Notre Dame University-Louaize (NDU), Lebanon (IRB# 202247). All procedures involving human participants were conducted in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Consent to participate
Prior to participation, an informed consent procedure was implemented via Google Forms. Participants were first presented with an information sheet detailing the study's purpose, confidentiality, voluntary nature of participation, and the contact details of the primary investigator. Informed consent was obtained electronically by clicking an “I Agree” button, which granted access to the questionnaire.
Consent for publication
This study does not include any identifiable individual data (such as individual details, images, or videos). Therefore, consent for publication is not applicable.
Author contributions
CO, AO and JG conceptualized the study. CO, AO and JG designed the questionnaire. CO translated the questionnaire to Arabic. CO and AA piloted the questionnaire and recruited participants. CO and JBD analyzed the results. CO wrote the original draft of the manuscript., AO, JG, AA and SPJK critically revised and edited the manuscript. All authors have read and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data supporting the findings of this study were collected anonymously via Google Forms and do not contain any identifying information. As such, the datasets may be made available by the corresponding author upon reasonable request, subject to institutional approval and in accordance with ethical guidelines.
Supplementary material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.