
Abstract
Objective
To describe recent trends in US MACI (autologous cultured chondrocytes on porcine collagen membrane) insurance approval rates, including the impact of defect location and the number of defects.
Design
MyCartilageCare case management team provides insurance prior authorization support for potential MACI patients through Vericel Corporation, the manufacturer of MACI. Data from insurance claims from 2021 to 2022 were assessed for non-military patients aged 17 to 55 years. Insurance outcomes were summarized, with approval defined as pre-authorization or pre-determination for the MACI procedure being secured prior to the initiation of treatment or cases where an estimate of coverage was provided prior to the initiation of treatment, respectively.
Results
A total of 5,158 cases were identified. In total, 87.7% of MACI cases were approved on initial submission, 9.4% were approved on appeal, 2.4% were not appealed, and 0.5% were denied after appeal. A total of 51.4% of cases included a patella defect, with similar rates of approval: 87.4% approved on initial submission, 9.6% approved on appeal, 2.5% not appealed, 0.5% denied after appeal. 29.9% contained more than one defect which were approved at similar rates: 87.1% approved on initial submission, 10.2% approved on appeal, 2.3% not appealed, and 0.5% denied after appeal.
Conclusions
MACI claims in the knee cartilage repair treatment algorithm are broadly supported by US third-party payers, with nearly 88% of all knee cartilage patients obtaining insurance approval on their initial submission and 97% of patients obtaining approval in total following appeal of initially denied claims. This is consistent across all groups including patella, non-patella, single, and multiple-defect cases.
Introduction
Focal cartilage defects can impact a patient’s pain, function, and activity level. Many cartilage repair and restoration procedures are available within the United States, including microfracture, subchondral drilling, osteochondral grafting procedures, autologous chondrocyte implantation, and matrix-induced autologous chondrocyte implantation. 1 MACI (autologous cultured chondrocytes on porcine collagen membrane) which was approved by the Food and Drug Administration (FDA) in 2017, is a two-staged procedure frequently employed for larger cartilage lesions (greater than 2 cm2) to harvest chondrocytes through a cartilage biopsy which are then cultured on a collagen membrane and finally implanted over the cartilage defect secured by fibrin glue.1 -3 The results of MACI have been promising with a shorter operative time compared to autologous chondrocyte implantation and satisfactory patient outcomes with high rates of patient satisfaction, improved Knee Injury and Osteoarthritis Score, International Knee Documentation Committee Score, Tegner score, Lysholm score, and low rates of treatment failure.4 -8 Despite the positive clinical outcomes, limitations to the procedure have included accessibility, given it requires a two-staged surgical procedure, and cost. 9
Cost is variable depending on the cartilage restoration procedure, but in the context of autologous chondrocyte implantation, which has been around longer and thus further investigated, one study showed the cost per additional quality-adjusted life year for autologous chondrocyte implantation was $6,791. 10 When assessed for defects greater than 2 cm2, another study demonstrated cost savings of $88,000 due to a reduction in the time lost from work due to their condition. 11 However, it remains a consideration that the cost will be dependent on insurer, country of residence, and the variation in MACI compared to ACI, as well as adjustments for current healthcare costs. A more recent study assessing the cost comparison between MACI and microfracture in Germany found MACI to have a higher initial cost during the first year of surgery but demonstrated treatment cost became comparable in post-operative years 2 and 3, with decreased treatment cost in post-operative years 4 and 5. 12 This is likely related to the identified durability of MACI/ACI with studies demonstrating high success rates over long-term follow-up.13,14
As MACI has been adopted as an important treatment option for chondral defects in the knee, it is imperative to identify if any insurance barriers can be reduced to potentially increase accessibility to treatment in appropriately indicated patients. The purpose of this study is to evaluate recent insurance approval rates for those in the United States who have submitted pre-authorization or pre-determination claims for MACI to determine the potential impact on cost, and, thus, the role of insurance on accessibility, including further investigation of the impact on defect location and defect number on the rates of approval. Our study aims to evaluate the overall rates of insurance approval and identify any difference in approval rates based on the number of defects or defect location. We hypothesize that the rates of approval for patients with multiple defects or patellar-containing defects would be lower overall compared to their counterparts.
Methods
Data Collection and Storage
In 2017, the US FDA approved the clinical use of matrix-induced autologous chondrocyte implantation. The Vericel Corporation, which owns the exclusive patented rights to MACI, established the MyCartilageCare case management team. This team functions to exclusively provide all insurance authorization support for any potential MACI patient. Through the MyCartilageCare program, all patient insurance information is stored and managed in a secure database. Data comprising MyCartilageCare’s case work were assessed. Patient names were removed for confidentiality, and patients were identified by MACI lot number and date at which case management work began (“case activation date”). A case is defined as a potential patient treatment instance (i.e., someone believed to benefit from MACI). All submissions pertaining to the same treatment instance are only counted once. Furthermore, all data represents case-level denial rates, such that if a payer denied a case based on its policy, those denials would be captured within the scope of the data set. Given the data were retrospectively assessed, de-identified, and provided by the corporation who run the established program, IRB approval was not required.
Inclusion Criteria
To assess recent insurance approval rates for those in the United States who have submitted pre-authorization or pre-determination claims for the MACI procedure, data were gathered on all patients who activated these claims for insurance approval of the procedure over 8 fiscal quarters spanning from quarter 1 of the 2021 fiscal year through quarter 4 of the 2022 fiscal year (
Inclusion and Exclusion Criteria.
Claims Information
All insurance activations were assessed. Patients either submitted claims as prior authorizations or pre-determinations. Prior authorizations were defined as cases where insurance approval was secured prior to the initiation of treatment, and pre-determinations were defined as an estimate of coverage provided prior to the initiation of treatment. Data on insurance approval or denial of these claims was collected as follows: initial prior authorization approved, initial prior authorization denied, prior authorization approved on appeal, prior authorization denied on appeal, pre-determination approved, pre-determination approved on appeal, and pre-determination denied. Ambiguous responses in this study were not appealed, and any resubmissions were handled by the case management team. These data were then interpreted in 4 groupings as percentages of the total number of claims for each grouping as follows: claims initially approved, claims denied and not appealed, claims denied and denied on appeal, and claims denied and approved on appeal.
Statistical Analysis
Statistical analyses were performed in R (R version 4.3.1, http://www.r-project.org). Prior authorization and pre-determination counts were pooled. Two-by-two contingency tables compared approval outcome (approved vs. denied) across lesion location (patella-containing vs. non-patella) and lesion number (multiple vs. single defects). Pearson’s chi-square test assessed associations (α = 0.05). Unadjusted odds ratios (OR) with 95% confidence intervals (CI) were calculated with the Woolf log-method; Non-patella and Single defect served as reference categories.
Results
All Activations
From the beginning of fiscal year 2021 through the end of fiscal year 2022, there were 5,158 total activations for all non-military patients aged 17 to 55 who submitted prior authorization or pre-determination approval for MACI. Of these 5,158 activations, 3,948 were approved on the initial prior authorization, 95 were denied on their initial prior authorization, 420 were approved on appeal of their initially denied prior authorization, 24 were denied on their appeal of their initially denied prior authorization, 574 were approved on their initial pre-determination, 31 were denied outright without appeal on their initial pre-determination, and 66 were approved on appeal of their initially denied pre-determination (
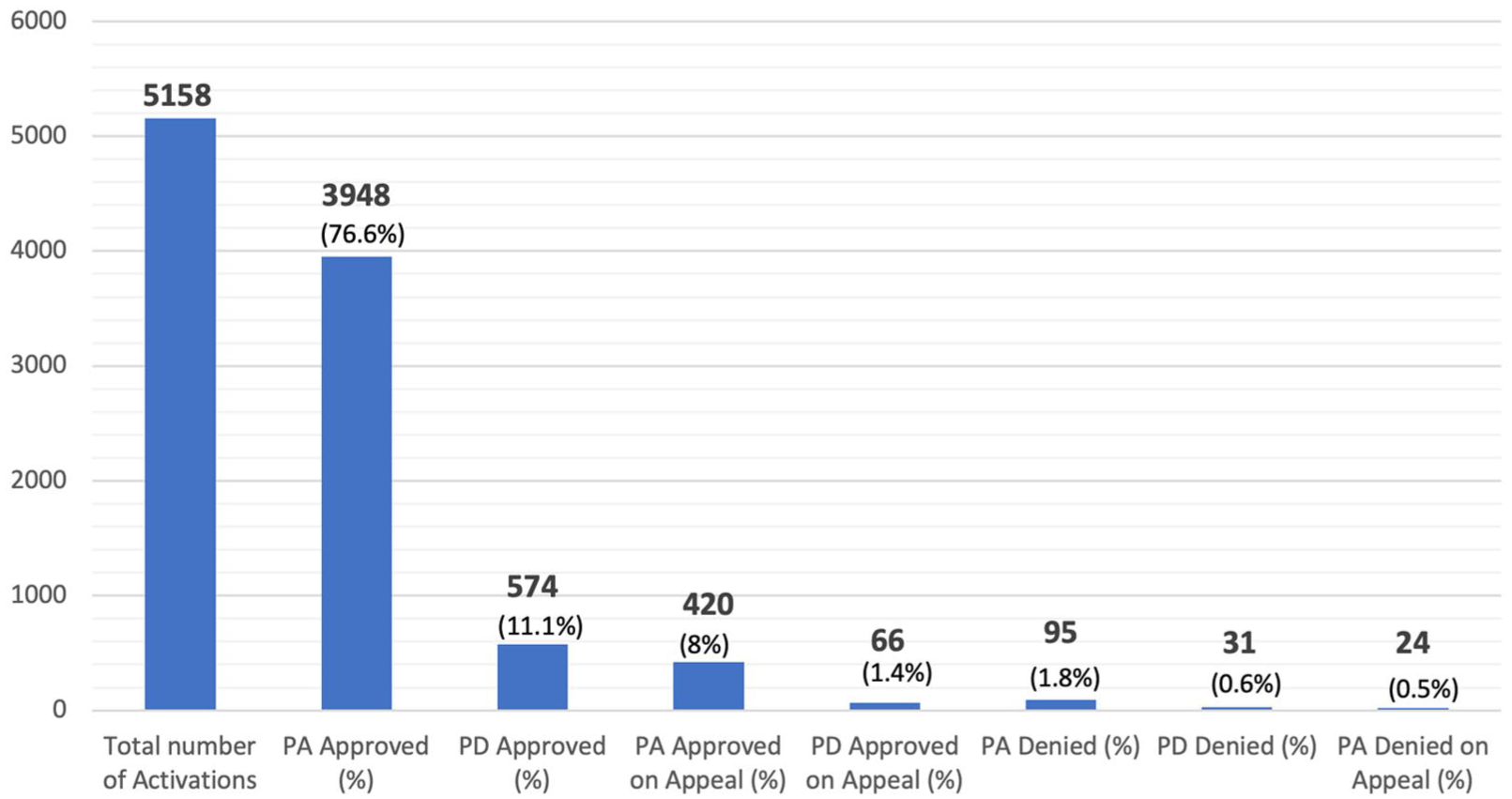
Total number of activations with the number of patients experiencing initial approval, approval on appeal, denial on appeal, and outright denial. PA = prior authorization; PD = pre-determination. Data reported as n (%).
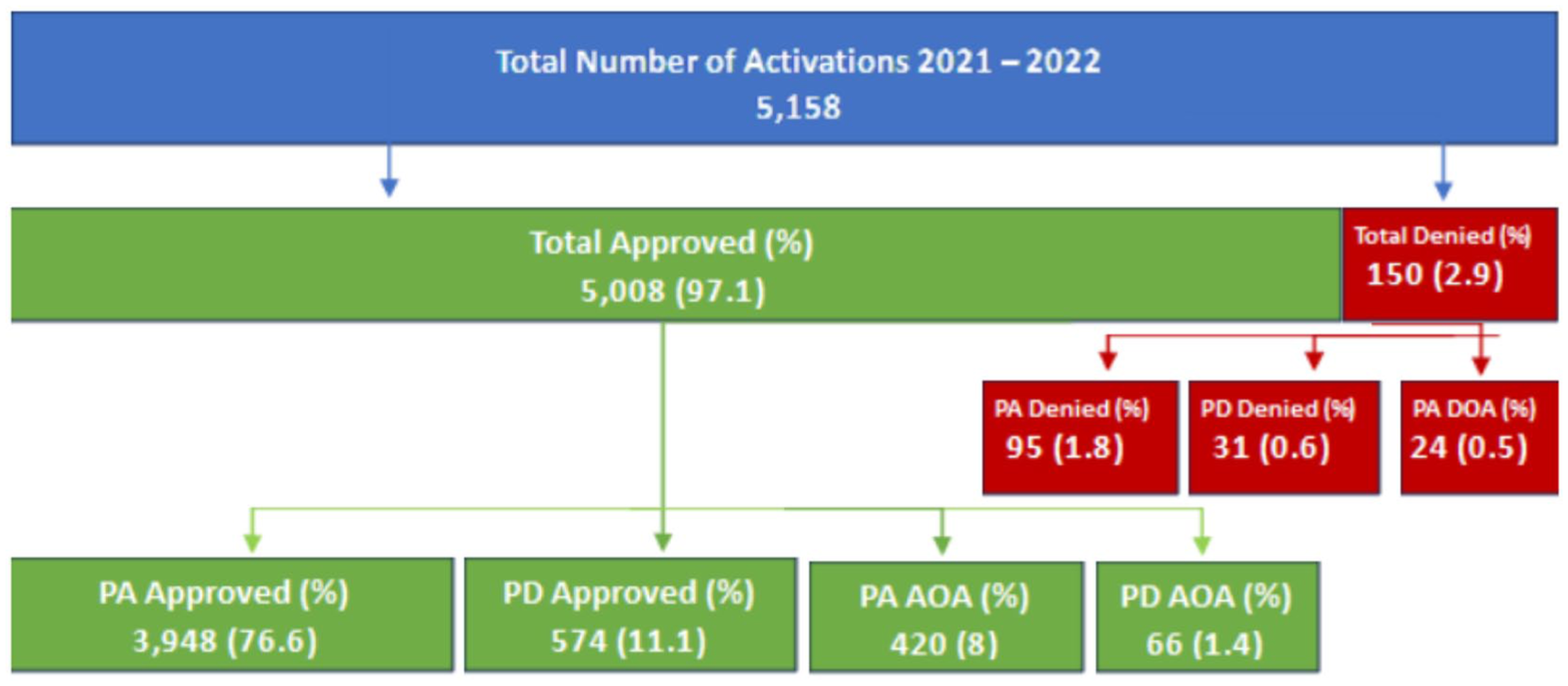
Total number of activations with the number of patients experiencing initial approval, approval on appeal, denial on appeal, and outright denial. PA = prior authorization; PD = pre-determination; DOA = denied on appeal; AOA = accepted on appeal. Data reported as n (%).
Activations with Patellar-Containing Cartilage Defects
Of all activations during this period, 2,653 of them had cases with patella-containing lesions. Of these, 2,022 were approved on the initial prior authorization, 50 were denied on their initial prior authorization, 226 were approved on appeal of their initially denied prior authorization, 13 were denied on their appeal of their initially denied prior authorization, 297 were approved on their initial pre-determination, 16 were denied outright without appeal on their initial pre-determination, and 29 were approved on appeal of their initially denied pre-determination. This led to an initial approval rate of 87.4%, an approval on appeal rate of 9.6% for claims initially denied, a denial on appeal rate of 0.5% for claims initially denied, and an outright denial rate without appeal of 2.5% (
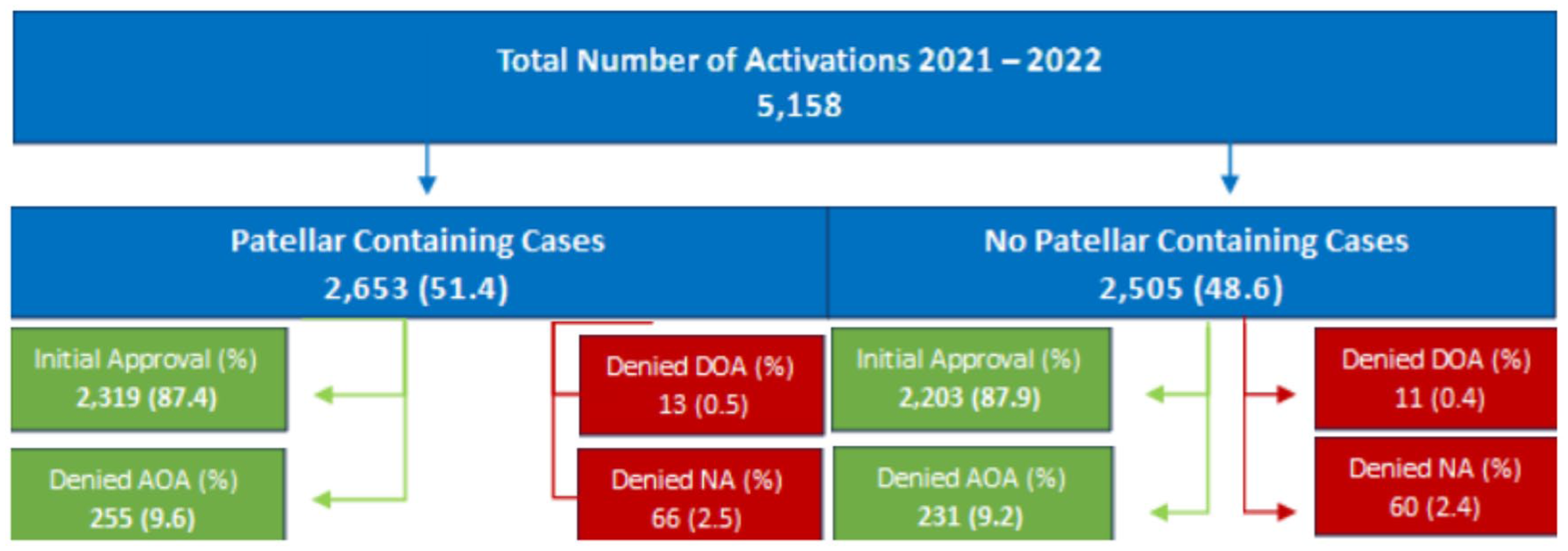
Total number of activations with the number of patients experiencing initial approval, approval on appeal, denial on appeal, and outright denial with or without patellar defects. NA = not appealed; DOA = denied on appeal; AOA = accepted on appeal. Data reported as n (%).
Activations without Patellar-Containing Cartilage Defects
Of all activations during this period, 2,505 of them had cases without patella-containing lesions. Of these, 1,926 were approved on the initial prior authorization, 45 were denied on their initial prior authorization, 194 were approved on appeal of their initially denied prior authorization, 11 were denied on their appeal of their initially denied prior authorization, 277 were approved on their initial pre-determination, 15 were denied outright without appeal on their initial pre-determination, and 37 were approved on appeal of their initially denied pre-determination. This led to an initial approval rate of 87.9%, an approval on appeal rate of 9.2% for claims initially denied, a denial on appeal rate of 0.4% for claims initially denied, and an outright denial rate without appeal of 2.4% (
Activations with a Single Cartilage Defect
Of all activations during this period, 3,614 of them had cases with a single cartilage defect. Of these, 2,786 were approved on the initial prior authorization, 71 were denied on their initial prior authorization, 282 were approved on appeal of their initially denied prior authorization, 17 were denied on their appeal of their initially denied prior authorization, 391 were approved on their initial pre-determination, 20 were denied outright without appeal on their initial pre-determination, and 47 were approved on appeal of their initially denied pre-determination. This led to an initial approval rate of 88%, an approval on appeal rate of 9% for claims initially denied, a denial on appeal rate of 0.5% for claims initially denied, and an outright denial rate without appeal of 2.5% (
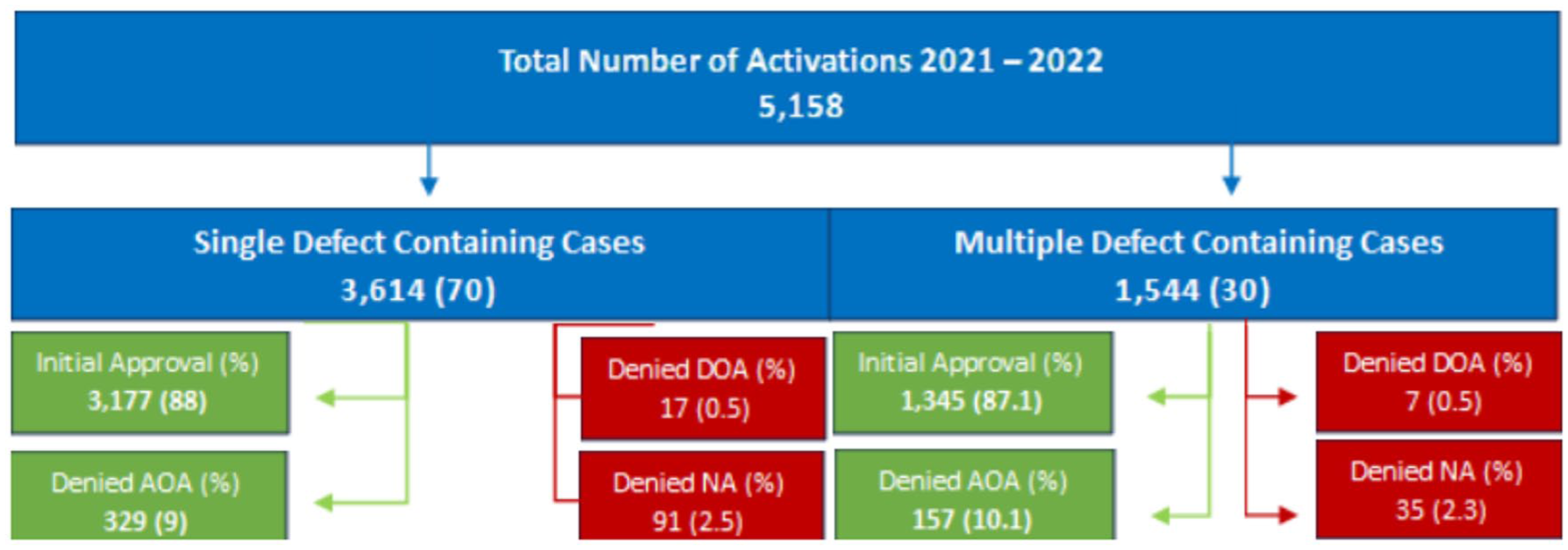
Total number of activations with the number of patients experiencing initial approval, approval on appeal, denial on appeal, and outright denial with or without multiple defects. NA = not appealed; DOA = denied on appeal; AOA = accepted on appeal. Data reported as n (%).
Activations with Multiple Cartilage Defects
Of all activations during this period, 1,544 of them had cases with multiple cartilage defects. Of these, 1,162 were approved on the initial prior authorization, 24 were denied on their initial prior authorization, 138 were approved on appeal of their initially denied prior authorization, 7 were denied on their appeal of their initially denied prior authorization, 183 were approved on their initial pre-determination, 11 were denied outright without appeal on their initial pre-determination, and 19 were approved on appeal of their initially denied pre-determination. This led to an initial approval rate of 87.1%, an approval on appeal rate of 10.1% for claims initially denied, a denial on appeal rate of 0.5% for claims initially denied, and an outright denial rate without appeal of 2.3% (
Statistical Analysis
Chi-square testing showed no significant difference in initial denial rates between patella-containing and non-patella lesions (12.6% vs. 12.1%; OR = 1.05, 95% CI = 0.89-1.24; P = 0.56) or between multiple and single defects (12.9% vs. 12.1%; OR = 1.08, 95% CI = 0.90-1.29; P = 0.43). After appeal, final denial remained low (≤ 5%) and similarly non-different across groups (all P > 0.75) (
Insurance-Approval Outcomes by Lesion Location and Lesion Number.
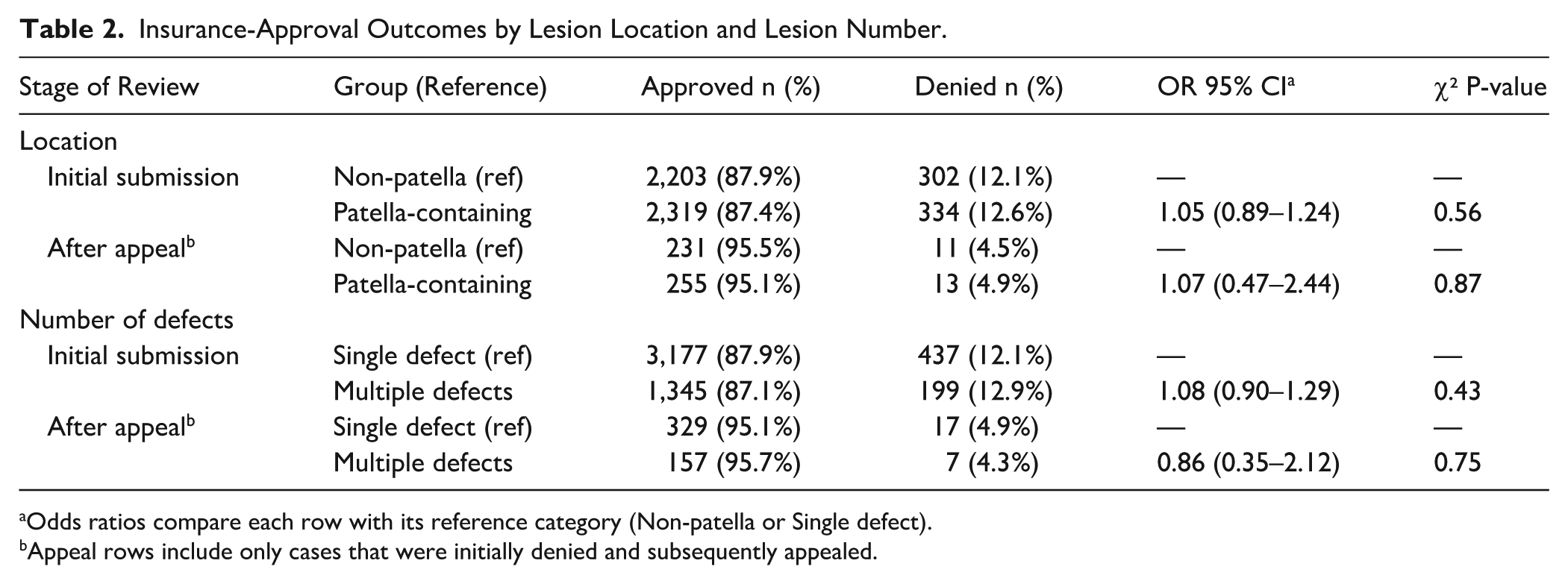
Odds ratios compare each row with its reference category (Non-patella or Single defect).
Appeal rows include only cases that were initially denied and subsequently appealed.
Discussion
The most important finding of this study is that MACI is approved at a very high rate among insurance carriers, with a total approval rate of 97.1%. Formal statistical testing confirms that neither lesion location nor lesion number meaningfully influences MACI insurance approval. These findings support the study’s conclusion that US payers apply consistent coverage criteria across common anatomical scenarios, reinforcing the overall accessibility of MACI for appropriately selected patients. The indications for MACI and adoption of treatment by US surgeons have been well described in the first 1,000 cases in the United States. 15 MACI is most used for a larger defect lesion size throughout the knee with a high percentage in the patellofemoral joint. The results of this study are encouraging as they relate to payer behavior surrounding insurance approval for the MACI, with overall high approval rates for prior authorization and pre-determination claims submitted for patients who have been clinically determined to benefit from MACI.
From the insurance aspect, it should be noted prior authorization and pre-determination are distinct, although both are completed prior to the clinical event or delivery of service. Generally, prior authorization, or pre-authorization or prior approval, is utilized by insurance companies to determine the medical necessity of the proposed treatment plan; however, it is the responsibility of the provider to submit the necessary medical information, often including things such as patient demographics, insurance, and clinical indications. Based on this request, the company may approve or deny the request, request additional information, or recommend alternative treatment options, thus not guaranteeing reimbursement. Conversely, pre-determination is a review of a patient’s proposed treatment compared to the medical and reimbursement policies of their insurance provider. While not always required, it is a way for the patient to confirm what portion of the proposed fees will be reimbursed and help them understand what their insurance plan will not cover. Despite the subtle differences, based on the results of this study, it is evident that regardless of claim type, the overall approval rate remains high for both types with a 97.3% approval percentage for those submitting prior authorizations and 95.4% approval percentage for those submitting pre-determinations.
Furthermore, the overall approval rate for all claims was 97% with nearly 88% of all knee cartilage patients ages 17 to 55 obtaining insurance approval on their initial submission regardless of a lesion in the patella or multiple cartilage defects. This is not insignificant, as prior research has identified the cost of treatment and insurance payment as a proposed barrier to cartilage restoration procedures. 9 Cost and accessibility of health care in the United States, in general, is a well-known barrier, so much so that the US Department of Health and Human Services, through the Agency for Healthcare Research and Quality, identified improving accessibility and affordability as two of their three major aims for improving healthcare nationally. 16 While not a direct surrogate for accessibility, the high rates of insurance approval for MACI in this study suggest most patients will receive insurance coverage and decreased overall treatment cost. More specifically, for those who receive insurance approval, as outlined in the Vericel MyCartilageCare procurement and reimbursement guide, 65% of commercially insured patients had $0 out-of-pocket expense, with 85% of patients having less than $2,000 in out-of-pocket expense. 17
With similar first-time approval rates for all cases (87.7%), those with (87.4%) or without (87.9%) a patellar defect, or single (88%) or multiple (87.1%) cartilage defects, recent insurance trends have decreased the out-of-pocket costs for the two-staged cartilage restoration procedure for a multitude of patient cases, likely increasing its overall affordability for patients seeking this treatment option. This is imperative, as a prior 2019 study on the cost-efficacy of knee cartilage defect treatments in the United States identified the total base cost of MACI including secondary operations at $65,263, with projections to increase to $67,373 by this year, compared to $25,662 for microfracture, $79,985 for osteochondral allograft, and $53,625 for knee arthroplasty. 18 By decreasing out-of-pocket costs through high rates of insurance approval, patients have a higher likelihood of being able to receive cost-effective treatment for their cartilage injury. At the orthopedic surgery benchmark for cost-effectiveness of $50,000 per quality-adjusted life year, MACI has been shown to remain a cost-effective treatment option even if symptom relief did not meet the minimally clinically important amount of 16.7 points on the International Knee Documentation Committee (IKDC) subjective score, there was a 50% increase in upfront treatment cost from baseline, or in a model projecting a 10-year failure rate of 15%.18,19
With multiple studies demonstrating significant improvements in clinical outcome scores, the benefit of high rates of insurance approval is more than just increasing patient access to cost-effective treatment but increasing access to cost-effective treatment that is clinically efficacious. In multiple studies assessing outcomes at different intervals including 2, 5, 10, and 15 years post-operatively, there have been significant improvements in a variety of patient-reported outcome measures including, Lysholm score, IKDC score, Tegner score, Knee Injury and Osteoarthritis Outcome Score, visual analog pain scale, Short Form-36, and International Cartilage Repair Society score, with high rates of overall patient satisfaction with knee function, up to 86% in 1 study with 15-year follow-up.5,20 -23
Limitations
Despite high rates of insurance approval for MACI in the United States, this study is not without its limitations. First, potential confounders such as a provider’s treatment site, geographic location, and/or formal patient diagnosis codes were not available, nor were lesion characteristics, information on prior procedures, or comorbidities, which may influence the above findings. In addition, high rates of insurance approval overall do not necessarily correlate with affordability for patients. Although Vericel notes 85% of patients have less than $2,000 in out-of-pocket costs, this does not mean this cost is affordable for 85% of patients and indicates that 15% of patients have a higher out-of-pocket cost. Furthermore, there remain a small percentage of patients that do not receive approval for which 100% of the cost would be out-of-pocket. Another limitation of the study is there is no reporting of the reasons the claims were either initially denied, denied outright, or denied on appeal. Further studies investigating this aspect may provide useful information to assist with creating and submitting successful claims. The activations assessed also did not include the type of insurance associated with the claim. Thus, further investigation into these data to assess any trends related to approval rates based on the type of insurance may prove beneficial in further understanding which patients have a higher likelihood of approval or denial. Finally, despite the most recent trend over the past 2 fiscal years, it should be acknowledged that insurance approval is fluid, and thus high insurance approval rates cannot be guaranteed annually; however, with continued investigation and ongoing literature to support the efficacy of MACI and its indications, it can be surmised that insurance approval rates should remain high overall.
Conclusion
MACI (autologous cultured chondrocytes on porcine collagen membrane) claims in the knee cartilage repair treatment algorithm are broadly supported by US third-party payers, with nearly 88% of all knee cartilage patients ages 17 to 55 obtaining insurance approval on their initial submission, with 97% of patients obtaining insurance approval in total following appeal of initially denied claims. These trends are consistent across all study groups with rates of approval between 87%–88% for patella, non-patella, single, and multiple-defect cases.
Footnotes
Acknowledgements
We would like to acknowledge Vericel for their collaboration with this project.
Authors’ Note
This study was supported by Vericel. The authors, individually and collectively, are responsible for all content and editorial decisions and have received no payment from Vericel directly or indirectly through a third party related to the development or presentation of this publication. The full prescribing information for MACI (autologous cultured chondrocytes on porcine collagen membrane) can be found via the MACI website ![]() .
.
ORCID iDs
Ethical Considerations
Through the MyCartilageCare program, all patient insurance information is stored and managed in a secure database. Patient names were removed for confidentiality, and patients were identified by MACI lot number and date at which case management work began (“case activation date”). Given the data were retrospectively assessed, de-identified, and provided by the corporation who run the established program, IRB approval was not required.
Consent to Participate
Given the data were retrospectively assessed, de-identified, and provided by the corporation who run the established program, individual consent to participate was not necessary for this study.
Consent for Publication
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The following authors declared relevant conflicts of interest as consultants for Vericel: E.J.S., MD; D.J., MD; S.L.S, MD; and D.C.F., MD. The remainder of the authors have no relevant conflicts of interest.
Data Availability Statement
Through the MyCartilageCare program, all patient insurance data are stored and managed in a secure database. All patient names were removed for confidentiality by the company prior to sharing insurance authorization data. All data are only accessible through the MyCartilageCare program.