
Abstract
Objective
To determine whether there are differences in MACI (matrix-induced autologous chondrocyte implantation) treatment in the United States, by comparing cartilage defects and patient characteristics between the initial 1,000 patients treated with the next 5,000
Methods
Following initial analysis of the first 1,000 consecutive patients treated with MACI, data were collected and analyzed for the subsequent 5,000. Patients were identified by MACI lot number and surgery date. Adverse events were summarized with descriptive statistics. Group differences were assessed with t-tests and chi-square, with significance set at P < 0.05.
Results
Five thousand adults (5,198 knees) were implanted with MACI by 1,130 surgeons. Patient sex (male 49.2%) was evenly split, and the mean age was 33.6 years. Most patients had a single cartilage defect treated, and the mean defect size was 4.4 cm2. The patella was the most treated surface (38.4%), followed by the medial femoral condyle (25.7%). Most patients (85.5%) had concomitant surgical procedures at the time of cartilage biopsy procurement. There were statistically significant differences in the number of patella (P < 0.001), medial femoral condyle (P < 0.001), and “not specified” (P = 0.008) between groups. Mean defect size and mean total defect size were both larger (P < 0.001 and P = 0.009, respectively) in the subsequent 5,000 patients.
Conclusion
The utilization of MACI has remained consistent. Patient demographics and concomitant surgical procedures between the first 1,000 MACI patients and subsequent 5,000 MACI patients were comparable. Patellofemoral defects were the most treated in both subsets, and an overall low rate of adverse events was observed.
Keywords
Introduction
Injuries involving the cartilage of the knee are exceedingly common. While a large number of these injuries are asymptomatic, symptoms can include pain, stiffness, or mechanical complaints such as clicking or locking of the joint. Furthermore, injuries to the cartilage can lead to alterations in its ability to distribute weightbearing forces effectively and create a susceptibility for further degeneration, eventually leading to osteoarthritis. 1 Treatment of cartilage defects, especially in the younger population, has historically presented a challenge.2,3 Factors such as defect size, location, knee alignment, patient demand in addition to sex, and body mass index (BMI) have all been proposed as useful to consider when deciding on the appropriate treatment. 4 Treatments often range from debridement or microfracture to restoration techniques such as osteochondral allograft or autograft, or cell-based treatments like autologous chondrocyte implantation (ACI) or its more novel variation, matrix-induced ACI (MACI). While smaller lesions are typically best managed with microfracturing or osteochondral autograft, the cell-based treatments are typically indicated in cases of younger patients with defects larger than 2 cm2. 5 Both ACI and MACI have been shown to have positive clinical outcomes in this setting.6,7
In December 2016, MACI (autologous cultured chondrocytes on porcine collagen membrane) received approval from the US Food and Drug Administration (FDA) for the treatment of symptomatic articular cartilage defects of the knee with or without bone involvement in adults. The FDA approval of MACI was supported by the results of the European SUMMIT (Superiority of MACI Implant Versus Microfracture Treatment) trial—a phase 3, 2-year, prospective, multicenter, randomized, open-label, parallel-group study that enrolled a total of 144 patients who had at least 1 symptomatic Outerbridge grade III or IV focal cartilage defect on the medial femoral condyle, lateral femoral condyle, and/or trochlea. 8 The initial 1,000 MACI patients in the United States were compared to those of the SUMMIT trial and found to be similar in patient age and mean total MACI-treated defect size. 9
As the number of patients being treated with MACI in the United States continues to grow, a re-examination of patient characteristics and trends associated with this procedure is necessary. The purpose of the present study is to determine whether there are any differences in trends in how MACI is being utilized in the United States, by comparing cartilage defects and patient characteristics between the initial 1,000 patients treated and the next 5,000 patients. Furthermore, by expanding on the initial study of MACI in the United States, we can further examine how trends in patient and defect characteristics may differ from those seen in the SUMMIT trial.
Methods
Data Collection and Storage
Following the initial analysis of the first 1,000 patients treated with MACI, the subsequent 5,000 patients were analyzed. Patient data, including demographic data and cartilage defect characteristics, were collected by Vericel (Vericel Corporation, Cambridge, MA). Patient names were removed for confidentiality, and patients were identified by MACI lot number and surgery date, prior to analysis by study authors. Thus, local Institutional Review Board (IRB) approval was not required to proceed with data analysis. Safety data were derived from the pharmacovigilance database, and adverse events were summarized with descriptive statistics.
Matrix-Induced Autologous Chondrocyte Implantation Manufacturing
Vericel (Vericel Corporation) provided a cartilage biopsy kit for the acquisition of cartilage specimens. All cartilage specimens were sent to Vericel, where chondrocytes were then cultured and cryopreserved. Once an MACI order was received, manufacturing was initiated, and implants were tested prior to shipment for surgery. Implants undergo rigorous testing, including several assays that ensure the implant contains chondrocytes that are viable, capable of producing a cartilage matrix (chondrogenic potential), and safe. Each biopsy was assigned a specific lot number. In a similar manner to the first 1,000 patients, 9 biopsy transmittal information as well as manufactured MACI sample information was recorded and entered in a customer relationship management (CRM) database.
Matrix-Induced Autologous Chondrocyte Implantation Treatment
All surgeons implanting MACI had undergone training in cartilage biopsy procurement, MACI implantation, and post-MACI rehabilitation before the initial shipment of MACI. The cartilage defects were to be prepared and the MACI implanted as described in the MACI prescribing information. Vericel cell therapy specialists or their designees were generally present for MACI surgeries.
Safety Data
Spontaneously reported adverse events were monitored and coded using the Medical Dictionary for Regulatory Activities (MedDRA).
Data Analysis
Patient demographics, cartilage defect characteristics, concomitant surgical procedures, and adverse events were summarized with descriptive statistics through the use of SAS (Version 9.4; SAS Institute, Cary, NC). Group differences were assessed with t-tests for continuous variables. Chi-square tests were performed to analyze the association between categorical variables. Significance was set at P < 0.05. Statistical analyses were performed with SigmaStat (version 3.5, San Jose, CA).
Results
Patient Demographics
Patient demographics are shown in Table 1 . A total of 5,000 adults (5,198 knees) were implanted with MACI by 1,130 surgeons. The average age was 33.6 years of age (SD 9.88). The male to female distribution was evenly split, with 2,539 patients being female (50.8%). A distribution of percentage of patients in each age range is shown in comparison to the first 1,000 patients in Fig. 1 . No significant differences in patient demographics, including age and sex, between subsequent 5,000 patients and the initial 1,000 patients were noted ( Table 1 ). The age range with the majority of patients in the next 5,000 patient cohort was the 30 to 40 age (35.7%).
Patient Demographics (First 1,000 vs. Next 5,000 Patients).
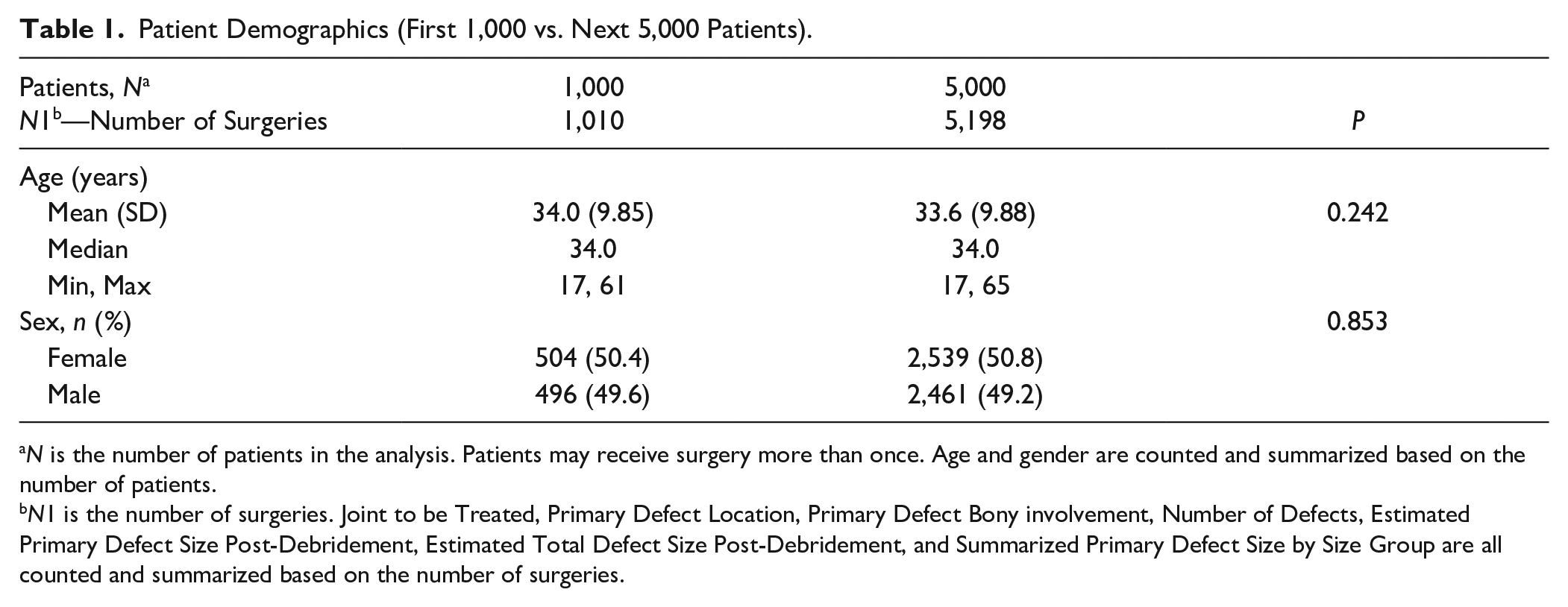
N is the number of patients in the analysis. Patients may receive surgery more than once. Age and gender are counted and summarized based on the number of patients.
N1 is the number of surgeries. Joint to be Treated, Primary Defect Location, Primary Defect Bony involvement, Number of Defects, Estimated Primary Defect Size Post-Debridement, Estimated Total Defect Size Post-Debridement, and Summarized Primary Defect Size by Size Group are all counted and summarized based on the number of surgeries.
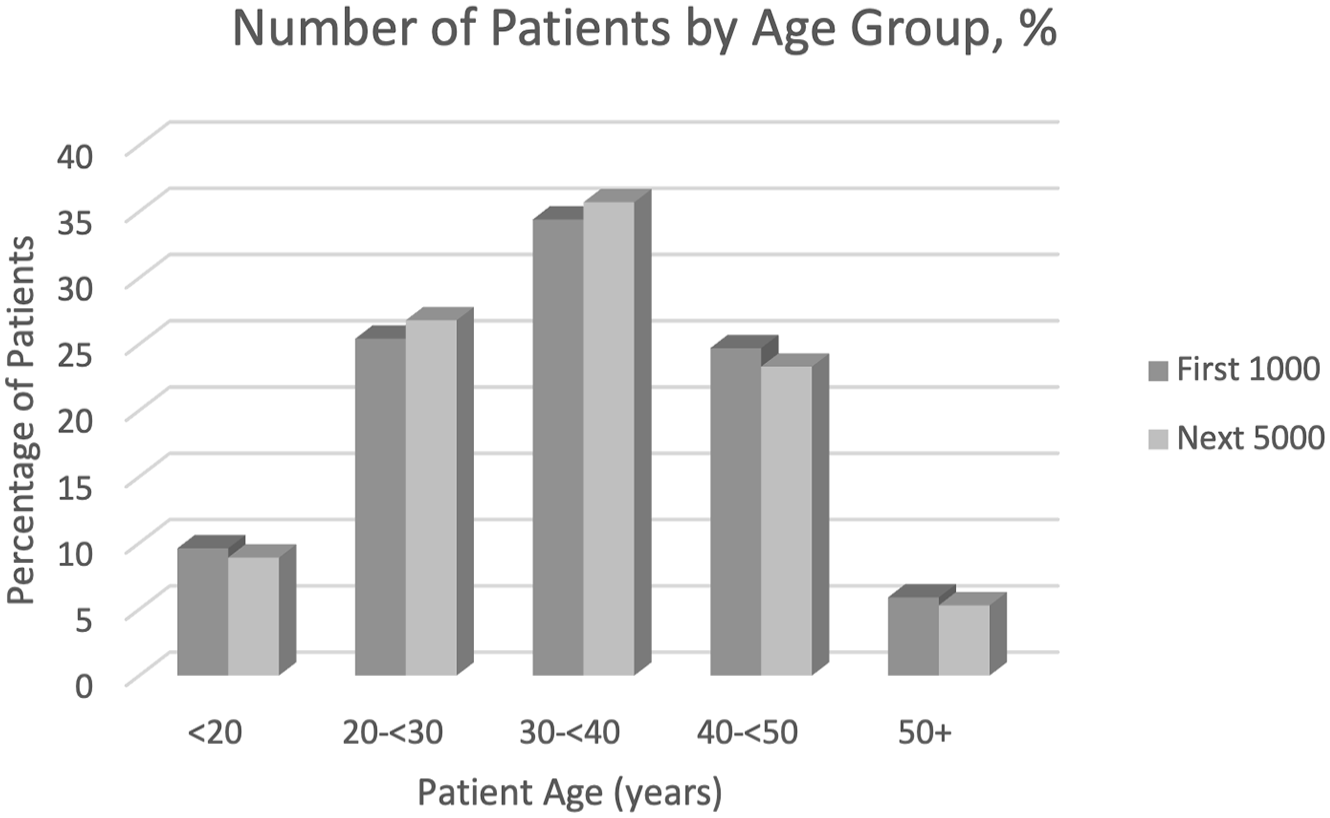
Age distribution of patients treated with MACI (autologous cultured chondrocytes on porcine collagen membrane) in the initial 1,000 patients and the next 5,000 patients. Shown are the age categories for MACI-implanted adult patients aged 17 years and older.
Cartilage Defect Characteristics
Defect size and defect characteristics are shown in Tables 2 and 3 . Among the 5,198 knees treated, a single cartilaginous defect was treated in the majority (67.1%) of cases ( Table 2 ). There were statistically significant differences in the number of patella (P < 0.001), medial femoral condyle (P < 0.001), and “not specified” (P = 0.008) between groups. Furthermore, lesions in both the trochlea and patella also were statistically difference (P = 0.005). The estimated primary defect size across the 5,198 defects analyzed was 4.36 cm2, while mean estimated total defect size, including multiple defects, was 5.44 cm2 ( Table 3 ). Mean defect size and mean total defect size were both statistically larger (P < 0.001 and P = 0.009, respectively) in the subsequent 5,000 patients compared to the first 1,000. A distribution of percentage of defects in each size range is shown in comparison to the first 1,000 patients in Fig. 2 . The size range with the highest percentage of defects was from 4 to 5 cm2. The majority of patients fell within the 2 to 6 cm2 range (69.7%).
Defect Characteristics (First 1,000 vs. Next 5,000 Patients).
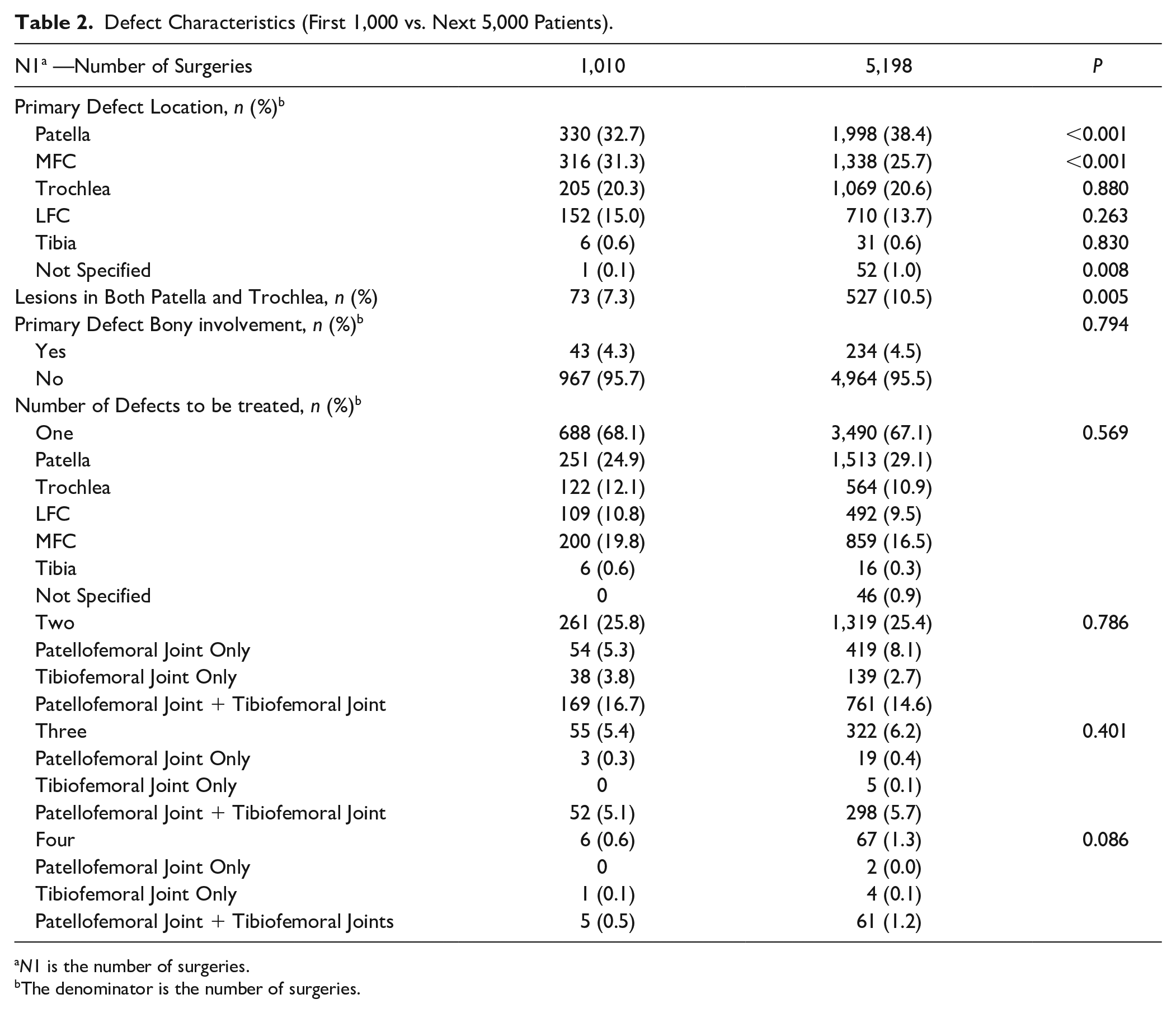
N1 is the number of surgeries.
The denominator is the number of surgeries.
Defect Characteristics (First 1,000 vs. Next 5,000 Patients).
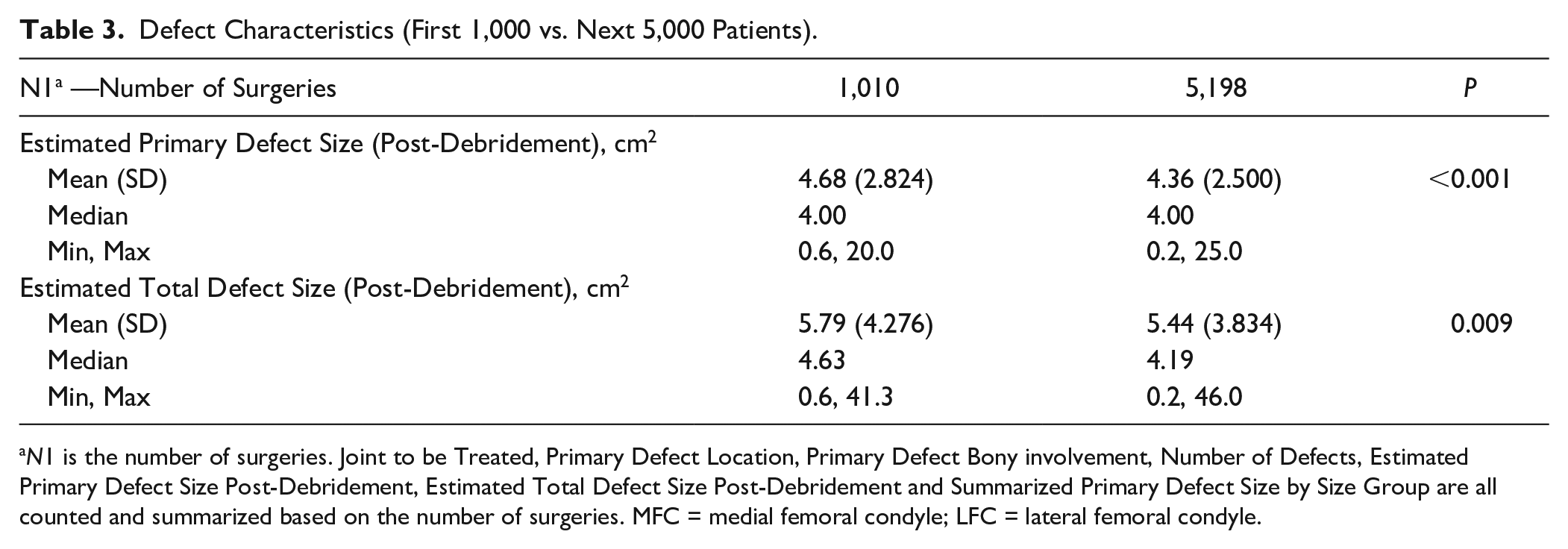
N1 is the number of surgeries. Joint to be Treated, Primary Defect Location, Primary Defect Bony involvement, Number of Defects, Estimated Primary Defect Size Post-Debridement, Estimated Total Defect Size Post-Debridement and Summarized Primary Defect Size by Size Group are all counted and summarized based on the number of surgeries. MFC = medial femoral condyle; LFC = lateral femoral condyle.
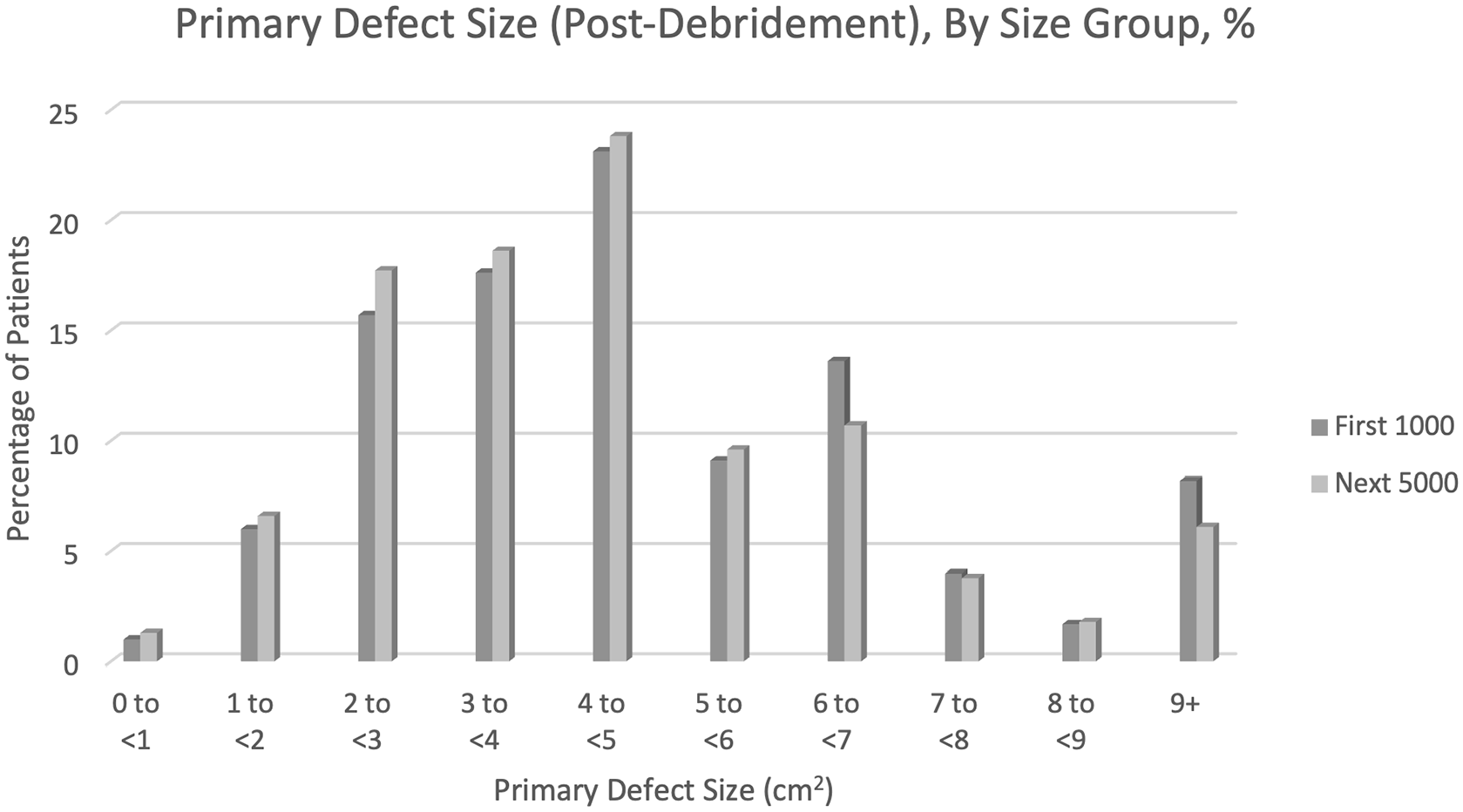
Size categories of cartilage defect treated with MACI (autologous cultured chondrocytes on porcine collagen membrane). Shown are the percentage of patients among the first 1,010 MACI-implanted knees and the next 5,198 MACI-implanted knees, in size categories for the larger/largest (if >1) MACI-implanted cartilage defect post-debridement.
A total of 234 surgeries were for defects with bony involvement ( Table 2 ). The patella was the most common site for cartilage defect, present in 1,998 knees (38.4%), followed by medial femoral condyle in 1,338 (25.7%), and trochlea in 1,069 (20.6%). Among the 3,490 (67.1%) surgeries where 1 defect was planned to be treated, the patella was most common. In those where 2 or more defects were to be treated, the majority (1,120/1,708, 65.6%) were in both the patellofemoral and tibiofemoral joints. A total of 527 patients had defects within the trochlea and the patella concomitantly (10.5%) (Appendix).
Concomitant Procedures
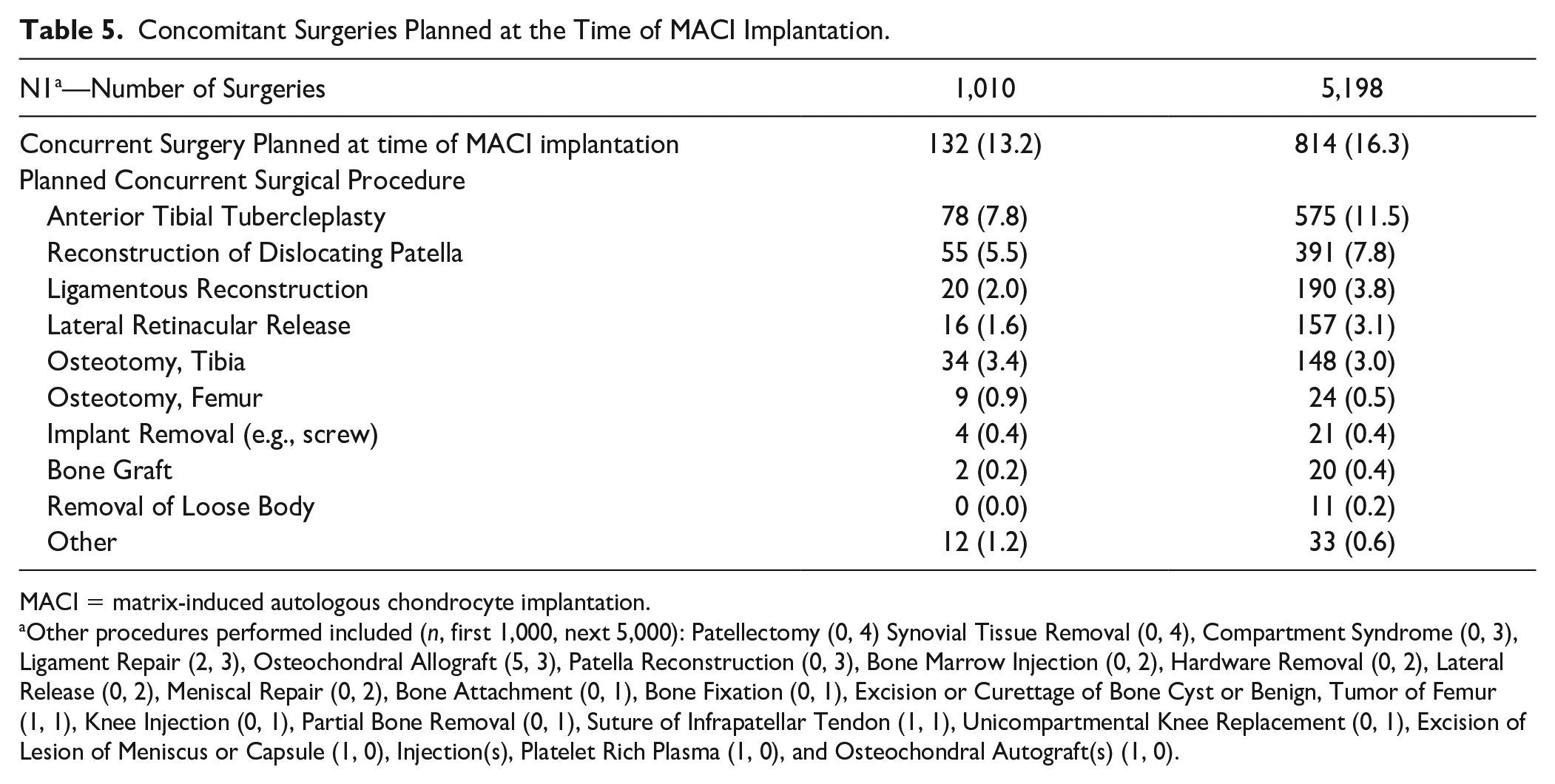
Concurrent procedures of any type at the time of biopsy occurred in the majority (85.5%) of cases ( Table 4 ). The most common concomitant procedure at the time of biopsy was chondroplasty and cartilage debridement in 78.5% of such cases (3,927 knees). By contrast, a minority of patients (814, 16.3%) had concurrent operations planned at the time of MACI implantation ( Table 5 ). The most common planned concomitant procedure at the time of implantation was anterior tibial tubercleplasty (575, 11.5%).
Concomitant Surgeries at the Time of Cartilage Biopsy.
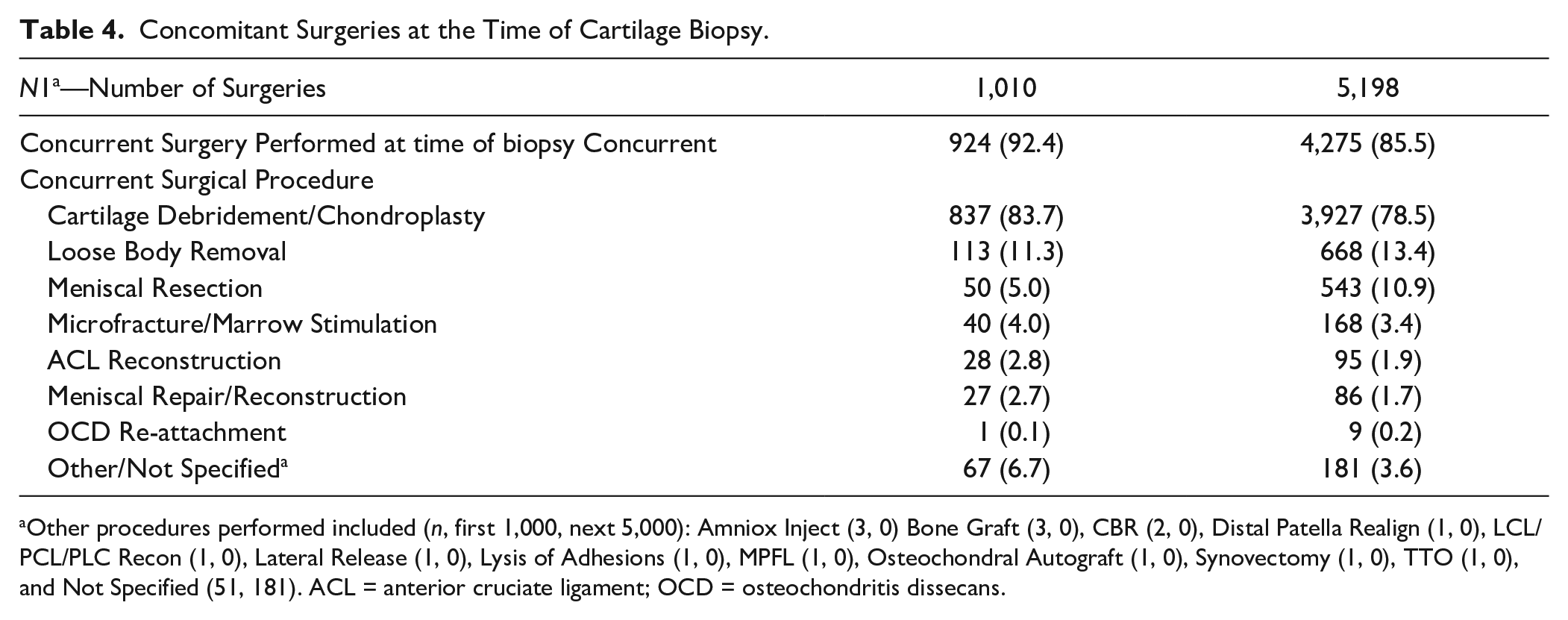
Other procedures performed included (n, first 1,000, next 5,000): Amniox Inject (3, 0) Bone Graft (3, 0), CBR (2, 0), Distal Patella Realign (1, 0), LCL/PCL/PLC Recon (1, 0), Lateral Release (1, 0), Lysis of Adhesions (1, 0), MPFL (1, 0), Osteochondral Autograft (1, 0), Synovectomy (1, 0), TTO (1, 0), and Not Specified (51, 181). ACL = anterior cruciate ligament; OCD = osteochondritis dissecans.
Concomitant Surgeries Planned at the Time of MACI Implantation.
MACI = matrix-induced autologous chondrocyte implantation.
Other procedures performed included (n, first 1,000, next 5,000): Patellectomy (0, 4) Synovial Tissue Removal (0, 4), Compartment Syndrome (0, 3), Ligament Repair (2, 3), Osteochondral Allograft (5, 3), Patella Reconstruction (0, 3), Bone Marrow Injection (0, 2), Hardware Removal (0, 2), Lateral Release (0, 2), Meniscal Repair (0, 2), Bone Attachment (0, 1), Bone Fixation (0, 1), Excision or Curettage of Bone Cyst or Benign, Tumor of Femur (1, 1), Knee Injection (0, 1), Partial Bone Removal (0, 1), Suture of Infrapatellar Tendon (1, 1), Unicompartmental Knee Replacement (0, 1), Excision of Lesion of Meniscus or Capsule (1, 0), Injection(s), Platelet Rich Plasma (1, 0), and Osteochondral Autograft(s) (1, 0).
Adverse Events
Overall, an adverse event was reported in 1.9% of cases or 95 patients. In total, there were 161 spontaneously reported adverse events. By MedDRA System Organ Class, General disorders and administration site conditions had the most patients with a reported event (36, 0.7%), followed by Injury, poison, or procedure complications (34, 0.7%), product issues (28, 0.6%), and musculoskeletal and connective tissue disorders (24, 0.5%) ( Table A1 in Appendix). These data were similar to the analysis of the first 1,000 patients, 9 with no individual events reported in more than 1% of patients in either analysis.
Discussion
This study demonstrates consistency in indications for MACI procedure the United States since its approval in 2016, with some important differences comparing the next 5,000 patients to receive the treatment. Since the initial 1,000 patients to undergo this procedure in the United States, the majority of patients are still managed for a single defect, and the patellofemoral joint continues to be the predominant implanted region of the knee joint. 9 Furthermore, no differences among patient demographics (age, sex) were noted. A few statistically significant differences between these populations were seen, however. Namely, the number of patella, medial femoral condyle, and those unspecified differed between groups, as well as lesions in both the trochlea and patella concomitantly. Furthermore, mean defect size and mean total defect size were both statistically larger in the subsequent 5,000 patient group.
The initial study of the first 1,000 patients to receive MACI in the United States revealed a population of patients and defects similar to that of the European SUMMIT (Superiority of MACI Implant Versus Microfracture Treatment) trial. 8 The SUMMIT study included a minimum cartilage defect size of 3 cm2. While this same requirement was not included in either this or the prior study assessing patients to receive the procedure in the United States, the vast majority of defects included in this study continue to be those greater than this mark. Based on the findings in this study, it can be deduced that the subsequent 5,000 MACI patients in the United States, although not discretely compared to the SUMMIT study population, demonstrate the same differences and consistencies as the present comparison. With overall similarities in patient demographic data, including age and sex, an overall consensus in patient population among surgeons both in the United States and Europe is indicated. The differences noted in defect characteristics, although statistically significant, may lack clinical relevance. It is possible that the defect size and number of defects may be increasing over time as a result of surgeons’ overall comfort and trust in the procedure growing.
The application of cell-based treatments for osteochondral defects in the United States has continued to evolve as with post-operative rehabilitation and return-to-activity guidelines. Initially, with ACI, use was limited to femoral condyle lesions only. In the last decade, this application has progressed to the present day, where MACI has approval for any lesion within the knee joint. Our sample shows that the patellofemoral joint has emerged as the primary location of lesions treated with this technique, indicating a complete evolution in its use. Furthermore, since the first 1,000 patients in the United States, consensus regarding post-operative protocols have been developed for patients after an MACI procedure. 10 The present study does not include any outcome-related data, and future studies are necessary to continue to evaluate these outcomes in light of a well-defined protocol.
Limitations to MACI use as it currently stands are a paucity of data existing in older individuals, as well as efficacy of its use outside of the knee joint. Limitations exist within the present study itself as well. Namely, no patient-reported outcomes data is assessed in this study, and no data regarding patient activity level, medical history, prior surgeries, or sports participation were included. In the study assessing the initial 1,000 patients to receive MACI in the United States, the potential influence of insurance claims on the reported defect size and concomitant procedures was brought forth. This included the potential for underreporting or overreporting cartilage defect characteristics to facilitate insurance coverage, which may ultimately influence the accuracy of the findings included. Given the similar nature of the database on the subsequent 5,000 patients included in the present study, this potential limitation remains. Furthermore, while the present study attempts to report on the prevalence of concomitant procedures in MACI surgery, it reports only on planned concomitant procedures prior to surgery. The actual concomitant procedures performed may be much different than those initially planned. An additional limitation exists in the individual bias among surgeons when choosing to or not to perform the MACI procedure. While 1,130 surgeons performed the 5,198 procedures, the distribution in unlikely to be uniform, and thus, indications included may be dictated by a small minority of surgeons. Finally, adverse event reporting and safety analysis are subject to a short follow-up period, and further study regarding long-term follow-up of these patients is necessary. All reported adverse effects were included to remain consistent with the initial 1,000 patient analysis; however, it is acknowledged that reporting on potentially unrelated adverse events may be inconsistent and introduce bias into the study.
Conclusion
The utilization of MACI has remained consistent. Patient demographics, defect characteristics, and concomitant surgical procedures between the first 1,000 MACI patients and subsequent 5,000 MACI patients were comparable. Utilization of MACI to treat larger defects was observed in the more recent cohort of patients, perhaps indicating an increase in surgeons’ confidence. Age and defect size continue to be consistent with FDA recommendations. Patellofemoral defects were the most commonly treated in both subsets, and an overall low rate of adverse events was observed.
Footnotes
Appendix
Adverse Events by MedDRA System Organ Class.

| N1—Number of Surgeries | 1,010 | 5,198 |
|---|---|---|
| Adverse Events by MedDRA System Organ Class | Adverse events, n (%) | |
| Blood and lymphatic system disorders | 1 (0.1) | 0 (0.0) |
| Bone marrow edema | 1 (0.1) | 0 (0.0) |
| Gastrointestinal disorders | 1 (0.1) | 0 (0.0) |
| Abdominal pain, lower | 1 (0.1) | 0 (0.0) |
| General disorders and administration site conditions | 13 (1.3) | 36 (0.7) |
| Asthenia | 1 (0.1) | 0 (0.0) |
| Atrophy | 0 (0.0) | 1 (0.0) |
| Chills | 0 (0.0) | 1 (0.0) |
| Complication of device insertion | 0 (0.0) | 1 (0.0) |
| Condition aggravated | 0 (0.0) | 1 (0.0) |
| Crepitations | 1 (0.1) | 1 (0.0) |
| Death | 0 (0.0) | 1 (0.0) |
| Discomfort | 0 (0.0) | 2 (0.0) |
| Effusion | 0 (0.0) | 1 (0.0) |
| Fatigue | 1 (0.1) | 0 (0.0) |
| Feeling abnormal | 1 (0.1) | 0 (0.0) |
| Gait inability | 1 (0.1) | 0 (0.0) |
| Hypertrophy | 0 (0.0) | 1 (0.0) |
| Implant site pain | 1 (0.1) | 0 (0.0) |
| Inflammation | 1 (0.1) | 0 (0.0) |
| Malaise | 1 (0.1) | 1 (0.0) |
| No adverse event | 0 (0.0) | 1 (0.0) |
| Pain | 3 (0.3) | 10 (0.2) |
| Peripheral swelling | 1 (0.1) | 0 (0.0) |
| Procedural failure | 0 (0.0) | 1 (0.0) |
| Pyrexia | 0 (0.0) | 1 (0.0) |
| Swelling | 1 (0.1) | 4 (0.1) |
| Treatment failure | 3 (0.3) | 13 (0.3) |
| Ulcer | 0 (0.0) | 1 (0.0) |
| Immune system disorders | 1 (0.1) | 0 (0.0) |
| Autoimmune disorder | 1 (0.1) | 0 (0.0) |
| Infections and infestations | 2 (0.2) | 4 (0.1) |
| Cellulitis | 1 (0.1) | 0 (0.0) |
| Diverticulitis | 1 (0.1) | 0 (0.0) |
| Folliculitis | 1 (0.1) | 0 (0.0) |
| Infection | 0 (0.0) | 2 (0.0) |
| Post-operative wound infection | 0 (0.0) | 1 (0.0) |
| Septic shock | 0 (0.0) | 1 (0.0) |
| Skin infection | 1 (0.1) | 0 (0.0) |
| Staphylococcal sepsis | 0 (0.0) | 1 (0.0) |
| Wound infection | 0 (0.0) | 1 (0.0) |
| Injury, poisoning and procedural complications | 8 (0.8) | 34 (0.7) |
| Cartilage injury | 0 (0.0) | 2 (0.0) |
| Contusion | 1 (0.1) | 0 (0.0) |
| Delayed graft function | 0 (0.0) | 1 (0.0) |
| Fall | 0 (0.0) | 3 (0.1) |
| Graft complication | 2 (0.2) | 3 (0.1) |
| Graft delamination | 3 (0.3) | 12 (0.2) |
| Graft overgrowth | 2 (0.2) | 2 (0.0) |
| Joint dislocation | 1 (0.1) | 0 (0.0) |
| Joint injury | 0 (0.0) | 1 (0.0) |
| Ligament sprain | 0 (0.0) | 1 (0.0) |
| Post-procedural hemorrhage | 0 (0.0) | 1 (0.0) |
| Post-procedural swelling | 1 (0.1) | 0 (0.0) |
| Procedural pain | 3 (0.3) | 9 (0.2) |
| Transplant failure | 0 (0.0) | 2 (0.0) |
| Investigations | 1 (0.1) | 5 (0.1) |
| Arthroscopy | 0 (0.0) | 4 (0.1) |
| Quality of life decreased | 0 (0.0) | 1 (0.0) |
| White blood cell count increased | 1 (0.1) | 0 (0.0) |
| Metabolism and nutrition disorders | 0 (0.0) | 1 (0.0) |
| Iron deficiency | 0 (0.0) | 1 (0.0) |
| Musculoskeletal and connective tissue disorders | 13 (1.3) | 24 (0.5) |
| Arthralgia | 8 (0.8) | 11 (0.2) |
| Arthrofibrosis | 1 (0.1) | 0 (0.0) |
| Arthropathy | 1 (0.1) | 2 (0.0) |
| Cartilage hypertrophy | 1 (0.1) | 0 (0.0) |
| Chondromalacia | 1 (0.1) | 0 (0.0) |
| Exostosis | 0 (0.0) | 1 (0.0) |
| Joint effusion | 3 (0.3) | 1 (0.0) |
| Joint instability | 1 (0.1) | 1 (0.0) |
| Joint lock | 0 (0.0) | 2 (0.0) |
| Joint noise | 0 (0.0) | 3 (0.1) |
| Joint range of motion decreased | 1 (0.1) | 1 (0.0) |
| Joint stiffness | 1 (0.1) | 0 (0.0) |
| Joint swelling | 1 (0.1) | 1 (0.0) |
| Knee deformity | 1 (0.1) | 0 (0.0) |
| Loose body in joint | 0 (0.0) | 2 (0.0) |
| Mobility decreased | 0 (0.0) | 2 (0.0) |
| Muscle atrophy | 1 (0.1) | 1 (0.0) |
| Musculoskeletal disorder | 0 (0.0) | 1 (0.0) |
| Pain in extremity | 0 (0.0) | 1 (0.0) |
| Tendonitis | 0 (0.0) | 1 (0.0) |
| Weightbearing difficulty | 0 (0.0) | 1 (0.0) |
| Neoplasms benign, malignant and unspecified (including cysts and polyps) | 1 (0.1) | 0 (0.0) |
| Benign laryngeal neoplasm | 1 (0.1) | 0 (0.0) |
| Nervous system disorders | 0 (0.0) | 1 (0.0) |
| Hypoesthesia | 0 (0.0) | 1 (0.0) |
| Product issues | 0 (0.0) | 28 (0.6) |
| Device dislocation | 0 (0.0) | 1 (0.0) |
| Device failure | 0 (0.0) | 2 (0.0) |
| Device material issue | 0 (0.0) | 1 (0.0) |
| Device physical property issue | 0 (0.0) | 2 (0.0) |
| Product complaint | 0 (0.0) | 20 (0.4) |
| Product contamination physical | 0 (0.0) | 1 (0.0) |
| Product size issue | 0 (0.0) | 1 (0.0) |
| Psychiatric disorders | 4 (0.4) | 0 (0.0) |
| Depression | 2 (0.2) | 0 (0.0) |
| Emotional distress | 1 (0.1) | 0 (0.0) |
| Insomnia | 1 (0.1) | 0 (0.0) |
| Psychiatric symptoms | 1 (0.1) | 0 (0.0) |
| Stress | 1 (0.1) | 0 (0.0) |
| Respiratory, thoracic, and mediastinal disorders | 1 (0.1) | 1 (0.0) |
| Dyspnea | 1 (0.1) | 0 (0.0) |
| Pulmonary embolism | 1 (0.1) | 1 (0.0) |
| Skin and subcutaneous tissue disorders | 1 (0.1) | 1 (0.0) |
| Blister | 0 (0.0) | 1 (0.0) |
| Urticaria | 1 (0.1) | 0 (0.0) |
| Social circumstances | 1 (0.1) | 2 (0.0) |
| Bedridden | 0 (0.0) | 1 (0.0) |
| Loss of personal independence in daily activities | 1 (0.1) | 1 (0.0) |
| Surgical and medical procedures | 0 (0.0) | 3 (0.1) |
| Knee operation | 0 (0.0) | 1 (0.0) |
| Post-operative care | 0 (0.0) | 2 (0.0) |
| Vascular disorders | 2 (0.2) | 2 (0.0) |
| Deep vein thrombosis | 2 (0.2) | 0 (0.0) |
| Hot flush | 0 (0.0) | 1 (0.0) |
| Thrombosis | 0 (0.0) | 1 (0.0) |
Acknowledgments and Funding
The authors acknowledge Vericel for their collaboration with this project. The authors, individually and collectively, are responsible for all content and editorial decisions and have received no payment from Vericel directly or indirectly through a third party related to the development or presentation of this publication. The authors, individually and collectively, are responsible for all content and editorial decisions and have received no payment from Vericel directly or indirectly through a third party related to the development or presentation of this publication. The full prescribing information for MACI (autologous cultured chondrocytes on porcine collagen membrane) can be found via the MACI website ![]() .
.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: David C. Flanigan has received consulting fees from Medical Device Business Services Inc., Linvatec Corp., Smith and Nephew, Vericel, and DePuy Synthes; compensation for services other than consulting from Smith and Nephew; speaking fees from Vericel; and travel and lodging payments from Linvatec, Smith and Nephew, and Medical Device Business Services Inc. James Carey has received consulting fees and speaking fees from Vericel.
Ethical Considerations
Given the data were retrospectively assessed, de-identified, and provided by the corporation who run the established program, IRB approval was not required.
Consent to Participate
Given the data were retrospectively assessed, de-identified, and provided by the corporation who run the established program, individual consent to participate was not necessary for this study.
Consent for Publication
Not applicable.
Data Availability
The data that support the findings of this study are available from Vericel. Restrictions apply to the availability of these data.