
Abstract
Objective
To investigate whether meniscal injury leads to the development of patellofemoral (PF) osteoarthritis (PFOA) and to explore how synovitis and gait kinematics mediate this relationship.
Methods
Fifty-four male Wistar rats (12 weeks old) were randomly assigned to the control, sham, or destabilized medial meniscus (DMM) groups. The rats were subjected to gait analysis to assess the kinematic changes at 2, 4, and 8 weeks postoperatively. Subsequently, the rats were euthanized, and their right knees were harvested for histological analysis.
Results:
The Osteoarthritis Research Society International (OARSI) and modified Mankin (MM) scores in the DMM group were significantly higher than those in the control and sham groups at week 2 and significantly higher than those in the control group at week 4. The OARSI and MM scores in the sham group were significantly higher than those in the control group at weeks 2 and 4. The association between the DMM and OARSI scores was significantly mediated by the synovitis score and knee flexion angle at foot contact (proportion mediated: 58% and 10%, respectively). The association between the sham and OARSI scores was significantly mediated by the synovitis score and knee flexion angle (proportion mediated: 24% and 24%, respectively).
Conclusions:
DMM surgery induced articular cartilage damage in the PF joint. Synovitis and the knee flexion angle significantly mediated the association between DMM or sham surgery and PFOA development.
Introduction
The meniscus plays a critical protective role in the tibiofemoral joint via shock absorption and load distribution.1,2 Several recent studies have reported the relationship between meniscal pathology and patellofemoral (PF) osteoarthritis (OA) (PFOA).3-6 However, the relationship has not been adequately validated, and the mechanism by which meniscal injury causes PFOA remains unclear.
Synovial inflammation plays an important role in OA development. 7 Inflammation caused by meniscal pathology may also affect the PF joints. Moreover, biomechanical changes play an important role in the development of OA. 8 Meniscal pathology can cause compensatory changes in gait kinematics, and knee kinematic changes can alter PF joint contact pressure.9-12 However, the degree to which synovial inflammation or kinematic gait changes mediate the relationship between meniscal pathology and PFOA has not been examined. Understanding the mediating factors in meniscal injuries that lead to PFOA will aid in devising strategies for the prevention and treatment of PFOA, including rehabilitation.
This study aimed to investigate whether meniscal injury leads to the development of PFOA in an experimental model and to explore the degree to which synovitis and gait kinematics mediate the relationship between meniscal injury and PFOA. We hypothesized that meniscal injury would induce PFOA development and that synovitis and gait kinematics would mediate the relationship between meniscal injury and PFOA.
Methods
Animal Preparation
This study was approved by the Animal Research Committee of Kyoto University (approval number: Med Kyo 20010) and was conducted according to the Animal Research: Reporting of In Vivo Experiments (ARRIVE) guidelines. 13 Fifty-four male Wistar rats (12 weeks old) were purchased from SHIMIZU Laboratory Supplies Co., Ltd. (Kyoto, Japan) and placed in plastic cages with paper bedding on a 12-hour light/dark cycle at a constant temperature. The rats were allowed to move freely into their cages and had free access to food and water. They were randomly separated into 3 groups: control, sham, and destabilized medial meniscus (DMM), to confirm that DMM surgery causes PFOA (n = 18 in each group). All rats were subjected to gait analysis to assess kinematic changes at 2, 4, and 8 weeks postoperatively (n = 6 for each time point; weeks 2, 4, and 8). Subsequently, the rats were euthanized, and their right knees were harvested for histological analysis.
Surgical Procedures
DMM and sham surgeries were performed under anesthesia with 1.0 ml/kg pentobarbital sodium (Somnopentyl; Kyoritsu Seiyaku Corp., Tokyo, Japan). The right knees of the rats were shaved, disinfected, and prepared for aseptic surgery using sterile drapes, gloves, scalpels, sutures, needle holders, forceps, and pruners. DMM surgery was performed on the right knee, as previously described.6,14 The right knee joint was exposed following a medial capsular incision over the distal patella to the proximal tibial plateau and gentle lateral displacement of the knee extensors without patellar ligament transection. Subsequently, the medial meniscotibial ligament was transected, and the medial meniscus was displaced. After the replacement of the extensor muscles, the medial capsular incision was sutured, and the skin was closed. Sham surgery was performed on the right knee as an internal control using the same approach without transection of the medial meniscotibial ligament. The rats in the control group did not receive any intervention and served as naïve controls. If there were surgical failures, such as anterior cruciate ligament (ACL) cutting, the rats were excluded. However, there were no exclusion criteria for this study.
Histological Analysis
The knee joint samples were decalcified in 10% ethylenediaminetetraacetic acid for 3-4 weeks and cut halfway along the midsagittal plane. Subsequently, the samples were paraffin-embedded and sliced into 6-μm sections at 50-μm intervals. Paraffin-embedded sections were stained with hematoxylin and eosin to evaluate the degree of synovitis around the patella. Paraffin sections were stained with Safranin O/Fast green to determine the severity of articular cartilage degeneration. Synovitis was assessed using the synovitis scoring system described in Table 1 and a previous study. 15 Three membrane features (synovial lining cell layer, stromal cell density, and inflammatory infiltrate) were assessed as follows: 0 (none), 1 (slight), 2 (moderate), and 3 (strong). The synovitis score was determined by summing all the parameters. The parameter values were summarized and interpreted as follows: 0-1, no synovitis; 2-4, low-grade synovitis; and 5-9, high-grade synovitis. Cartilage degeneration in the patella of the PF joint was assessed using the Osteoarthritis Research Society International (OARSI) score and modified Mankin (MM) scores.16,17 The OARSI score consists of 6 grades and 4 stages on a scale of 0 (intact) to 24 (severe damage). The MM score comprised 3 features (pericellular matrix staining, spatial arrangement of chondrocytes, and interterritorial matrix staining) on a scale of 0 (intact) to 8 (severe). Cartilage degeneration was evaluated in the medial, lateral, and central regions of the patella at the PF joint. The average score of the 3 parts was defined as the outcome. The maximum score was used for all scoring systems and samples.
Synovitis Scoring System.

Gait Analysis
Gait analysis was performed to evaluate kinematic changes using a 3-dimensional (3D) motion capture apparatus (Kinema Tracer System; Kissei Comtec, Nagano, Japan). According to a previous study, before walking on the treadmill, the rats were anesthetized and equipped with markers. 18 Colored hemispheric markers were attached bilaterally to the anterior superior iliac spine, great trochanter (hip), lateral knee joint (knee), lateral malleolus (ankle), and lateral fifth metatarsophalangeal joint (MTP) on shaved skin. The colors of the adjacent markers were different. Subsequently, we calibrated the exact coordinates of a standard object (height, 100 mm; width, 50 mm; and length, 200 mm) before each session to ensure data accuracy. Following calibration, the rats walked on a treadmill at a speed of 18 m/min, and hind limb motion was recorded using cameras. Ten steps from the trials, during which the animals walked through at least 5 consecutive steps, were recorded for each rat, and the affiliated software automatically built 3D kinematic models based on the tracing markers attached to the 5 body landmarks. The knee flexion and toe-out angles were measured, and foot contact (FC) angles were used as outcomes. The knee flexion angle was formed by a line connecting the markers on “hip” and “knee” and another line connecting the markers “knee” and “ankle.” The toe-out angle was formed by a line connecting the markers “ankle” and “MTP” and the Y-axis line, which is the longitudinal direction of the treadmill. Kinematic data were averaged for each gait cycle.
Statistical Analysis
First, the OARSI and MM scores were compared among the 3 groups to confirm the development of PFOA following meniscal surgery. Kruskal-Wallis and post hoc Steel-Dwass tests were used to examine the differences between groups. Second, we explored whether synovitis or gait kinematics mediated the relationship between meniscal surgery (control, sham, or DMM) and PFOA development (
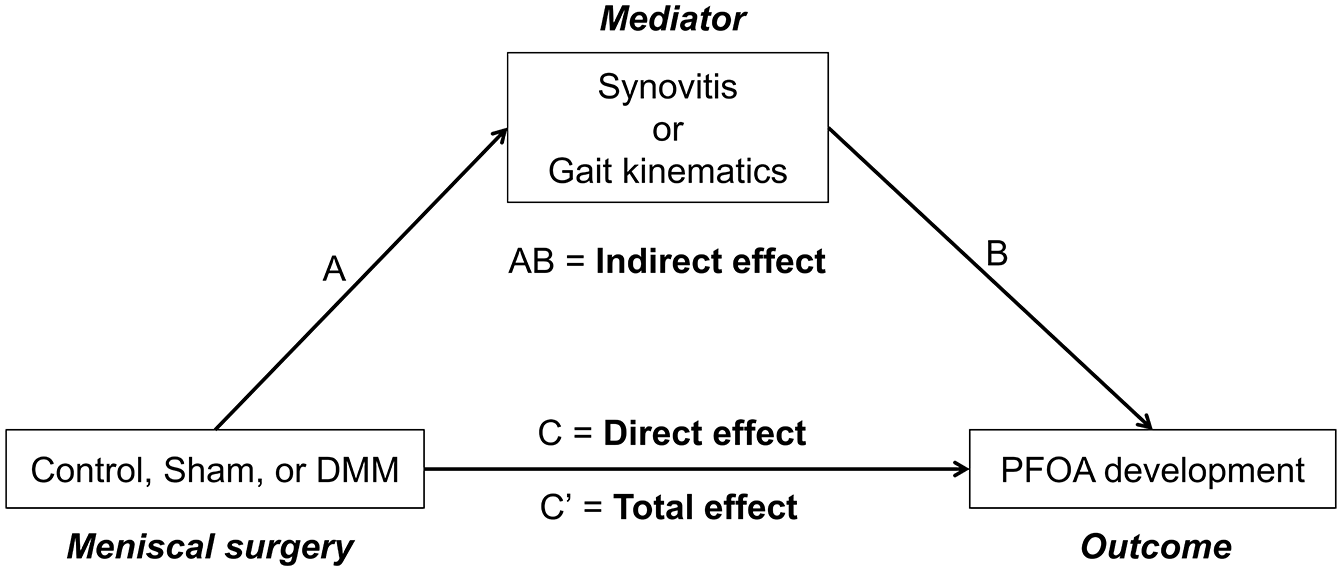
Conceptual path diagram of the association between meniscal surgery (control, sham, or DMM) and PFOA development mediated by synovitis or gait kinematics. DMM = destabilized medial meniscus; PFOA = patellofemoral osteoarthritis.
Results
Histological Analysis of the PF Joint
Articular cartilage damage to the patella was observed as fissure and matrix staining depletion at all experimental periods in the DMM and sham groups. However, the cartilage damage was more severe in the DMM group than in the sham group (
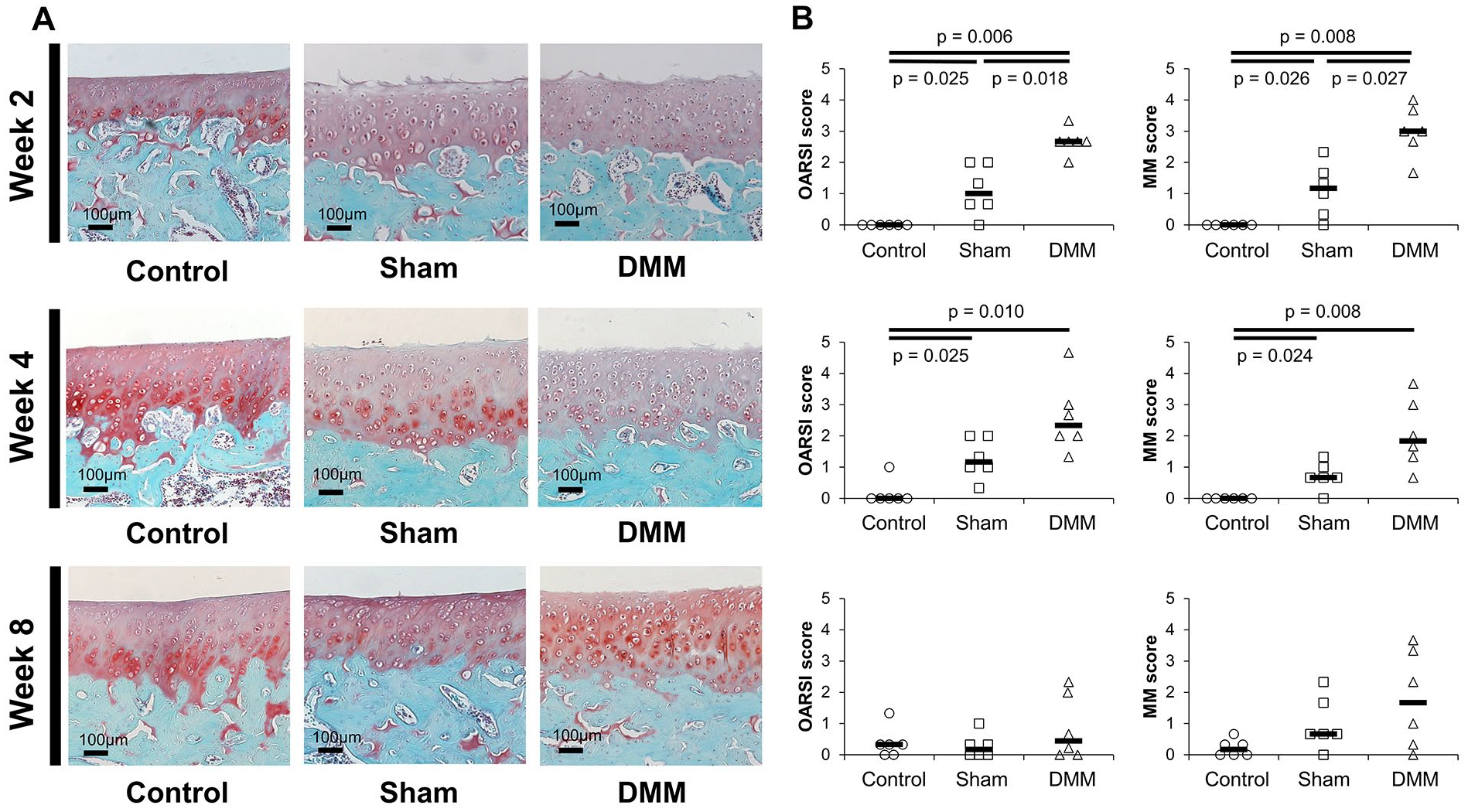
Histological images of Safranin O/Fast green stained specimens and osteoarthritis scores. (
In the post hoc analysis, power between the control and DMM groups was 1 (d = 9.94) at 2 weeks, 0.997 (d = 3.074) at 4 weeks, and 0.172 (d = 0.646) at 8 weeks for the OARSI score, and 1 (d = 5.66) at 2 weeks, 0.994 (d = 2.88) at 4 weeks, and 0.667 (d = 1.53) at 8 weeks for the MM score. Between the sham and DMM groups, power was 0.985 (d = 2.652) at 2 weeks, 0.678 (d = 1.55) at 4 weeks, and 0.251 (d = 0.821) at 8 weeks for the OARSI score, and 0.968 (d = 2.454) at 2 weeks, 0.777 (d = 1.744) at 4 weeks, and 0.187 (d = 0.683) at 8 weeks for the MM score.
Characteristics
Table 2
presents the characteristics of the study variables according to group. The average body weights in rats (12 weeks old) of the control, sham, and DMM groups were 265.11 ± 14.25, 258.89 ± 9.89, and 258.28 ± 9.92 g, respectively. The Mdn OARSI and MM scores were 0 and 0 points in the control group, 0.83 and 0.67 points in the sham group, and 2.17 and 2.5 points in the DMM group, respectively. The plots and Mdns of the synovitis scores for each group are shown in
Figure 3A
. The synovitis score in the DMM group was much higher than in the other groups, whereas the score in the sham group was slightly higher than in the control group. The scores in the DMM and sham groups were higher during the early postoperative period. The plots and means of knee flexion and toe-out angles at FC for each group are shown in
Characteristics of Each Group.

IQR = interquartile range; SD = standard deviation.
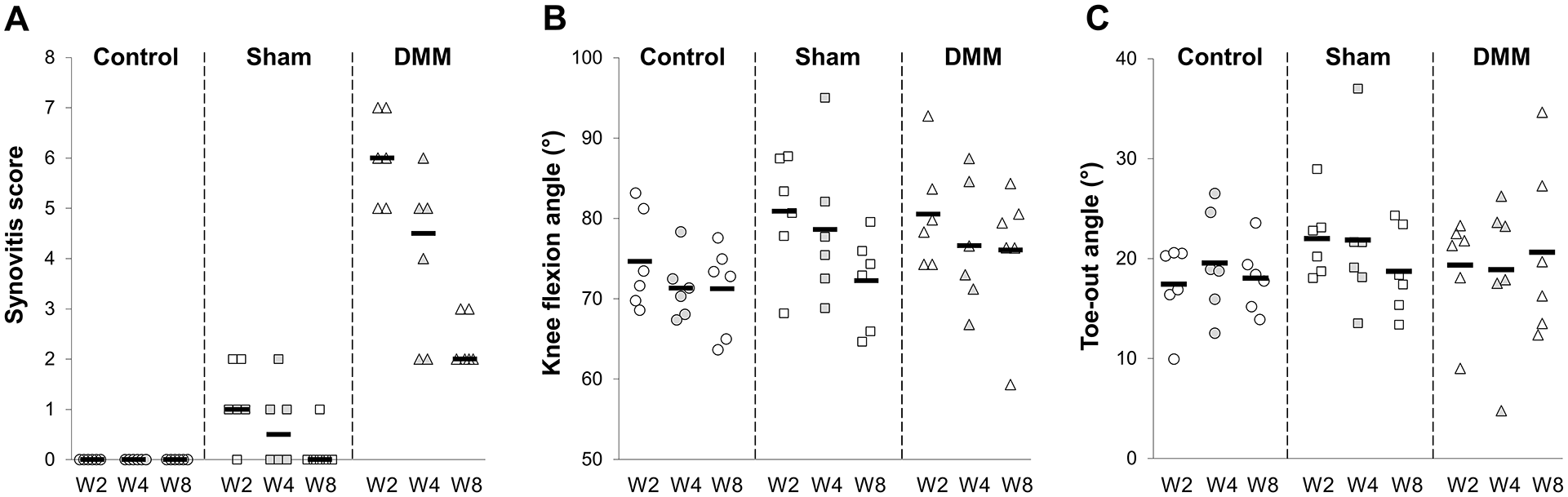
Plot diagram of the synovitis score, knee flexion angle, and toe-out angle by group. (
Total Effect of Meniscal Surgery on PFOA Development
The total effects of meniscal surgery on PFOA scores are presented in Table 3 . The total effects β (95% CIs) of the sham and DMM on the OARSI score were 0.70 (0.13-1.28) and 1.86 (1.29-2.44), respectively. The total effects β (95% CIs) of the sham and DMM on the MM score were 0.87 (0.31-1.43) and 2.20 (1.64-2.76), respectively. Significant associations were found between all examined variables. The power in the post hoc analysis was 0.999 (R 2 = 0.459) for the OARSI score and 0.999 (R 2 = 0.553) for the MM score.
Association of Meniscal Surgery With PFOA Mediated By Synovitis or Gait Kinematics.

Statistically significant associations are shown in bold.
β = regression coefficient; CI = confidence interval; T = total effect; D = direct effect; I = indirect effect; PM = proportion mediated; NA = not applicable.
Mediation Analysis
The results of the mediation analyses are presented in Table 3 . The mediation analysis showed that the association between the DMM group and the OARSI score was significantly mediated by the synovitis score and knee flexion angle at FC (indirect effects: β = 1.07 and 0.19, PM = 58% and 10%, respectively). Similarly, the association between the sham group and OARSI score was also significantly mediated by the synovitis score and knee flexion angle (indirect effects: β = 0.17 and 0.17, PM = 24% and 24%, respectively). The association between the DMM group and MM score was significantly mediated by the synovitis score (indirect effect: β = 0.85, PM = 39%).
Discussion
This is the first study to show that synovitis and knee flexion angle at the FC mediate the association between DMM and PFOA development and to validate that DMM surgery induces articular cartilage damage in the patella.
The relationship between inflammation and PFOA has been previously reported. Hart et al. 21 showed that synovitis in patients after ACL reconstruction was associated with the worsening of PF bone marrow lesions. In experimental models of patellar tendon shortening and monosodium iodoacetate (MIA) injections, synovitis has been shown to occur with the development of PFOA.22,23 Conversely, Egloff et al. 24 reported that acute inflammation may not be an independent factor in OA development because inflammatory stimuli (intra-articular injection of carrageenan) alone did not cause PFOA in rabbits. In the present study, synovitis and knee gait kinematics significantly mediated the development of PFOA in the DMM and sham groups. These findings suggest that synovitis may be a key factor in the development of PFOA, even if the initial triggers differ. Inflammation may not be a factor in OA development alone but may work synergistically with biomechanical factors. Moreover, the PM in the synovitis score was 58% (full mediation), and the knee flexion angle was 10% (partial mediation) in terms of the association between DMM and the OARSI score. This suggests that synovitis may contribute more compared with biomechanical changes to the association between DMM and PFOA. As a biomechanical factor, the knee flexion angle significantly mediated PFOA in the DMM and sham groups. These results are similar to those of a previous study, in which a decreased knee extension angle was associated with PFOA in patients with ACL injuries. 25 The toe-out gait has been reported to increase PF contact pressure in humans; 11 however, it did not have a significant mediation effect in the present study. The reasons for the lack of a mediation effect in this study could be that rats, which are quadrupedal, performed compensatory movements differently than humans, and that the gait analysis was performed on a treadmill.
In addition, this study confirmed that DMM surgery induces articular cartilage damage in the patella. This finding strengthens the relationship between meniscal pathology and PFOA in previous studies.3-6 In addition, it has been suggested that DMM surgery can be used as a PFOA model. Several animal models of PFOA have been established, including models of ACL transection,26-28 noninvasive ACL rupture, 29 patellar tendon shortening, 23 intra-articular injections of MIA, 22 and weakening of the quadriceps muscle by surgical denervation or intramuscular drug injection. 24 Tsai et al. 26 reported histological changes in rats after ACL transection, which resulted in subchondral bone marrow edema at 16 weeks and matrix degeneration with an irregular cartilage surface at 32 weeks. Fleischer et al. 29 used a model of noninvasive ACL rupture in rats and observed histopathological changes in the superficial zone of the cartilage with an early OA phenotype, including fibrillation, fissures, and increased cellularity at 2 weeks. Bei et al. 23 used a rat model of patellar tendon shortening to observe cartilage fibrils, chondrocyte swelling, horizontal clefts, and denudation after 10 weeks. Takahashi et al. 22 used a model of intra-articular injection of 1 mg MIA and observed histopathological changes with early OA resulting from cartilage fibrillation and fissuring at 4 weeks and with terminal OA resulting from erosion and denudation at 8 and 12 weeks. Thus, the PFOA model with MIA injection is useful for studying terminal PFOA. However, this model does not follow the typical OA process because OA is caused by chemically induced chondrocyte death. 30 In the present study, the DMM model showed early PFOA development that was histologically similar to that observed in ACL transection and rupture models. However, according to a previous study, meniscal surgery may increase contact pressure in the PF joint, 31 whereas ACL failure decreases contact pressure in the PF joint. 32 Therefore, the pathogenic mechanisms and appropriate therapeutic interventions may differ among PFOA models. Moreover, sham surgery, which involves a minor incision of the skin and capsule on the medial patellar tendon, resulted in mild PFOA, although similar sham surgeries in a previous study did not result in PFOA development. 26 In the sham group in the present study, mild synovitis was induced in the early postoperative period, and we believe that this was one of the factors leading to PFOA. As the sham group in the previous report was observed at 16 and 32 weeks postoperatively, inflammation and cartilage damage may have already resolved. In addition, the decreased stability and mobility of the PF joint associated with sham surgery may have contributed to PFOA.
This study strengthened the relationship between meniscal injury and PFOA. PFOA development should be prevented because it affects clinical symptoms, such as crepitation, anterior knee pain, and difficulties during stair ambulation.33-35 The findings of this study suggest that early improvement in synovial inflammation and knee extension during gait is important for preventing the development of PFOA after meniscal injury. Synovitis promotes cartilage degradation by producing pro-inflammatory mediators. 36 Therefore, mechanical loading of the PF joint should be carefully managed, especially during the inflammatory phase. In addition, restoration of knee extensor muscle strength, prevention of knee flexion contracture, and bracing or taping may be beneficial for improving knee extension during gait. However, it is important to note that rapid overloading of the PF joint during exercise may disrupt cartilage tissue homeostasis. 37 The load on the PF joint is 2 to 6 times greater when climbing steps, 5 to 10 times greater when descending stairs, and 5 times greater when squatting at 60° than when walking. 38 In addition, the load on the PF joint increased rapidly with closed kinetic chain exercises (e.g., squat and leg press) from 45° to 100° of knee flexion and open kinetic chain exercises (e.g., leg extension) from 20° to 0° of knee flexion. 39 Exercise and activities of daily living should be performed progressively according to the symptoms and findings of PF joint loading.
This study had several limitations. First, the sample size might not have been adequate because an a priori power analysis was not performed in this study. Most path models for mediation analysis involving the MM score did not differ significantly; however, the larger sample size may have affected the statistical results. Second, evaluating inflammation in the synovial fluid and cartilage may further clarify the influence of these processes on the development of PFOA. Third, other significant mediating variables may exist in addition to those identified in this study. Tibial rotation and anteroposterior positioning affect the contact area and pressure on the PF joint.9,40 In addition, patients with PFOA exhibit decreased quadriceps and hip abductor muscle strength. 41 Thus, these variables may have mediating effects. Fourth, patellar abnormalities, including patellar alta, patellar baja, and trochlear dysplasia, may have been present in the experimental rats. If abnormalities had been present, the results might have been affected.42,43 Finally, an experimental rat model was used in this study. Our findings may not translate directly to humans because differences in anatomy and gait style between rats and humans may affect the extent of cartilage degeneration.
In conclusion, we showed that DMM surgery in rats induced articular cartilage damage in the PF joints. Our findings suggest that DMM can be used as a PFOA model. In addition, we showed significant mediating effects of synovitis and knee flexion angle at the FC on the association between meniscal surgery and the development of PFOA. This study may contribute to our understanding of the mechanisms of PFOA pathogenesis and provide insights into clinical thinking, although further detailed studies are needed.
Footnotes
Acknowledgments and Funding
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was approved by the Animal Research Committee of Kyoto University (approval number: Med Kyo 20010) and was conducted according to the Animal Research: Reporting of In Vivo Experiments (ARRIVE) guidelines.