
Abstract
Objective
To synthesize the literature concerning return to sport (RTS) and related outcomes after cartilage restoration surgery of the knee in professional athletes.
Design
Cochrane, PubMed, and OVID/Medline databases were queried for data pertaining to RTS after knee cartilage surgery in professional athletes. Demographic information, cartilage lesion characteristics, and RTS-specific information were extracted. Freeman-Tukey Double-Arscine Transformations with Dersimonian-Laerd random-effects estimators were constructed to quantitatively describe the cumulative incidence of RTS, while heterogeneous data described narratively.
Results
Eleven studies (476 athletes; mean age 27.5 ± 2.1 years; 96.6% male) were included. Nine (81.8%) studies investigated a form of microfracture as treatment, with 6 (54.5%) performing isolated microfracture. The remaining studies investigated osteochondral allograft transplantation and mosaicplasty. More than half (n = 6; 54.5%) did not report cartilage lesion location or size. The pooled RTS rate was 84.3% (95% CI: 75.4%-91.8%) at a mean 39.9 (range, 12-104) weeks postoperatively. In 6 studies reporting competition level, a trend toward returning to a lower than pre-injury level was observed. The definition of RTS was only provided in 6 (54.5%) studies, while the criteria for RTS was only reported in 2 (18.2%) studies, suggesting limited transparency. One study reported an objective imaging assessment of reparative tissue, while none reported formal RTS testing protocols or minimum RTS timeline.
Conclusion
Although the majority of professional athletes are reported to achieve a successful RTS after cartilage restoration surgery of the knee, the literature predominantly reflects microfracture treatment. Current limitations in this literature include a substantial lack of female representation and infrequent reporting of cartilage lesion characteristics, rehabilitation and RTS criteria, and objective imaging assessments of reparative tissue.
Introduction
Articular cartilage injuries of the knee often cause significant disability in professional athletes.1,2 Due to the strenuous physical demands experienced across the tibiofemoral and patellofemoral joints during professional sports as a result of repetitive loading and pivoting, the articular cartilage experiences considerable stresses predisposing to a high incidence of cartilage injuries.3,4 Cartilage lesions may occur due to both acute traumatic injuries and insidious onset from cumulative trauma.1,5-7 Importantly, the avascular nature of cartilage limits its inherent healing and regenerative potential, while associated alterations in biomechanics due to symptoms from an inflammatory cytokine milieu may promote further cartilage breakdown and progression to early osteoarthritis8-10; therefore, in the setting of symptomatic cartilage defects of the knee in professional athletes that limit ability to compete, treatment interventions may be promptly indicated.
Multiple surgical treatment strategies have been implicated in the treatment of cartilage defects of the knee depending on the lesion size and location including bone marrow stimulation procedures such as microfracture (MF), autologous chondrocyte implantation (ACI), osteochondral autograft transplantation (OAT), and osteochondral allograft transplantation (OCA).11-18 Despite an accumulation of evidence in recent years surrounding the propensity for return to sport (RTS) after cartilage surgery,19-24 treatment outcomes in homogenous cohorts of professional athletes remain inconsistently reported and challenging to find. This paucity of data has led to continued debate and discussion regarding the optimal treatment approach in this challenging population of patients with high baseline functional capabilities and multiple internal and societal pressures to expedite RTS. Therefore, it is critical to better understand the propensity for RTS in professional athletes for prognostic counseling.
Additional clarity regarding treatment response and recovery may allow for enhanced decision-making with respect to treatment approach and both ability and timing of expected RTS. As such, the purpose of the current study was to synthesize the literature concerning RTS and related outcomes after cartilage restoration surgery of the knee in professional athletes. The authors hypothesized that the majority of athletes would report successful RTS, but that there exists limited data on treatment outcomes for procedures such as ACI and OCA given their extensive rehabilitation requirements.
Methods
Article Search Process
This systematic review and meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) statement. 25 Literature reporting on return to sport rates for athletes undergoing any cartilage restoration procedure in the knee was performed using the following indexing databases: (1) Cochrane Database of Systematic Reviews, the Cochrane Central Register of Controlled Trials, (2) PubMed, and (3) OVID/MEDLINE. The query was performed in December 2023 using combinations of the following Boolean search and terms: “Professional,” “Athlete,” “Athletic,” “Sport,” “Cartilage,” “Chondrocyte,” “Chondral,” “Osteochondral,” “Articular,” “Allograft,” and “Autograft.” This review was registered with the PROSPERO international prospective register of systematic reviews prior to initiation of data collection (PROSPERO identification: CRD42023483412).
Study Eligibility and Data Procurement
Studies qualified for inclusion if the topic of the identified study reported on any component of RTS in professional athletes that underwent a primary cartilage restoration procedure of the knee and were published in the English language. Exclusion criteria consisted of (1) editorials, abstracts, case reports, technical notes, and surveys, (2) biomechanical or cadaveric studies, (3) did not describe athletes based on competition level (i.e., reported as elite or highly competitive, but did not disclose whether athletes participated in professional competition); (4) did not report any RTS metrics; and (5) studies that combined the outcomes of professional athletes with other lower levels of competitive play, such as collegiate or high school athletes, thereby precluding the isolation of data for only the professional athletes. No restriction on level of evidence was imparted, with only level of evidence 5 being excluded. The term “professional athlete” in the current study was defined as athletes participating in an organized sport beyond the collegiate level, including semi-professional, professional, or Olympic competition.
All articles identified by the search were screened by 2 independent reviewers (RNU, ZDT). Sequential screening of all articles was performed, which included assessment of duplicates, screening of article title, evaluation of content within the abstract, and full text review. References of identified articles were also explored and reconciled in order to minimize risk of missing relevant literature. Furthermore, when duplicate cohorts were identified, the article with longer follow-up was included. All data were recorded into a custom spreadsheet using a modified information extraction table. 26 Categories for data collection for each full article included (1) article information; (2) cartilage restoration method; (3) patient information; (4) lesion size and location; and (5) RTS information, including type of sport, ability to RTS, level of competition, and time to RTS.
Assessment of Methodological Quality
The Methodological Index for Non-randomized Studies (MINORS) checklist 27 was used to evaluate the quality of all studies. The MINORS checklist involves 12 items to assess quality, of which only 4 are applicable to comparative studies. The 4 additional criteria specific to comparative groups were used to assess the bias present in articles when selecting cohorts. The maximum MINORS score is 16 for non-comparative studies and 24 for comparative studies.
Statistical Analysis
All statistical analyses were performed using the computing software R (Version 3.6.1) and RStudio (Version 1.2.5033, R Foundation for Statistical Computing, Vienna, Austria). A 2-tailed P-value of less than 0.05 was considered to indicate statistical significance. To quantify the rate of RTS, a meta-analysis of proportions with inverse-variance proportion models using Freeman-Tukey Double-Arscine Transformations and Dersimonian-Laerd random-effects estimators was constructed. The pooled proportion estimate, calculated as weighted averages of the individual effects from each included studied where weights represent the amount of information contributed by each study, were presented with estimates of uncertainty. The 95% confidence interval (CI) was used to report all pooled statistics. For all other recorded outcomes, trends were described narratively due to data heterogeneity and the potential to propagate bias and misleading conclusions. Heterogeneity was assessed by the I2 statistic using random-effects models and was regarded as insignificant when I2 = 0%, possibly unimportant when the I2 value was less than 40%, moderate between 40% and 75%, and considerable when more than 75%. 28
Results
A total of 11 studies comprising outcomes of 476 professional athletes that underwent a cartilage restoration procedure of the knee were included ( Fig. 1 ). The mean age of all athletes was 27.5 ± 2.1 years, and 96.6% (460/476) athletes were male. Nine (81.8%) studies investigated a variation of microfracture as treatment. Isolated microfracture was performed in 6 (54.5%) studies, with the remaining 3 studies performing microfracture with a concomitant treatment. One study performed microfracture and applied a Hyalofast membrane (Anika Therapeutics Inc., Bedford, MA, USA) with tissue glue stabilization of the membrane; one study was a prospective comparison of isolated microfracture versus autologous chondrocyte implantation; and one study performed arthroscopic mechanical and thermal chondroplasty, with 33% of patients also undergoing microfracture. The final study investigated the utility of osteochondral allograft transplantation (OCA) ( Table 1 ).
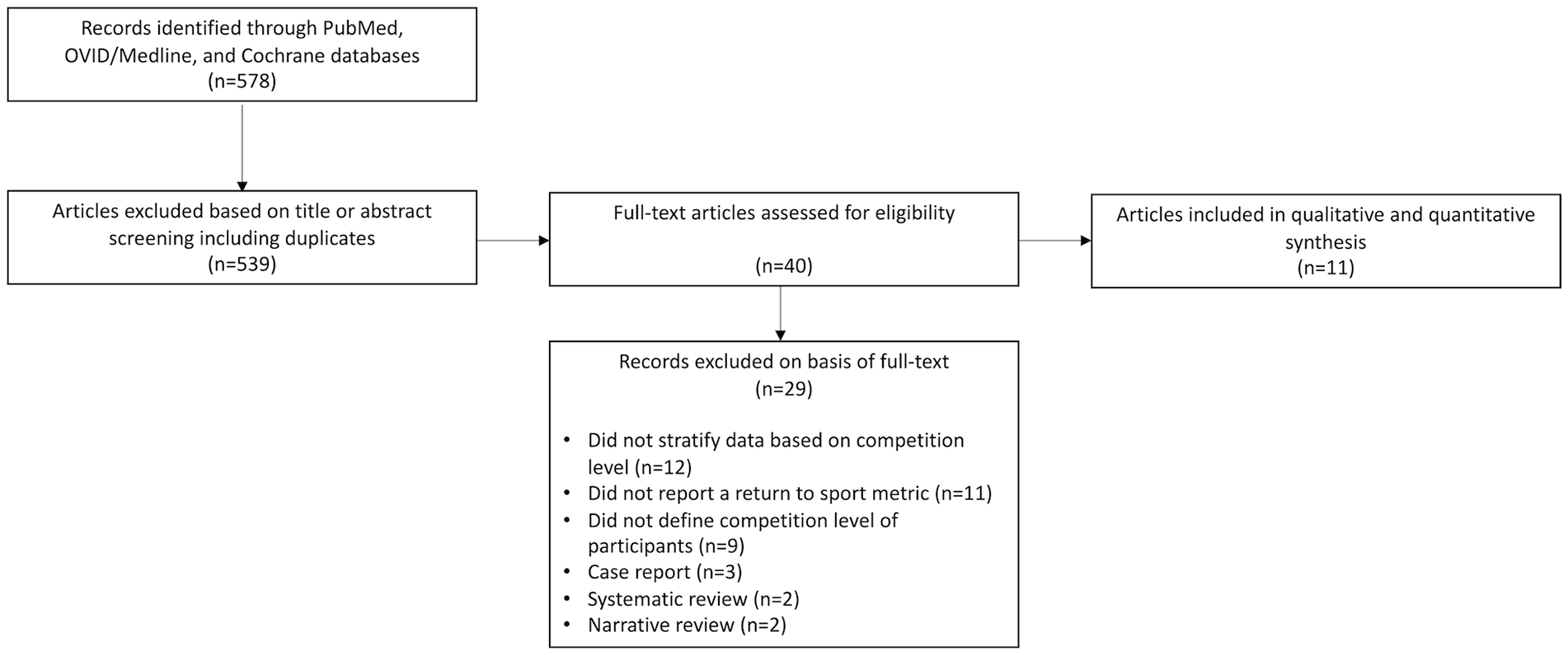
Study eligibility and selection process.
Study Characteristics and Patient Selection Criteria.
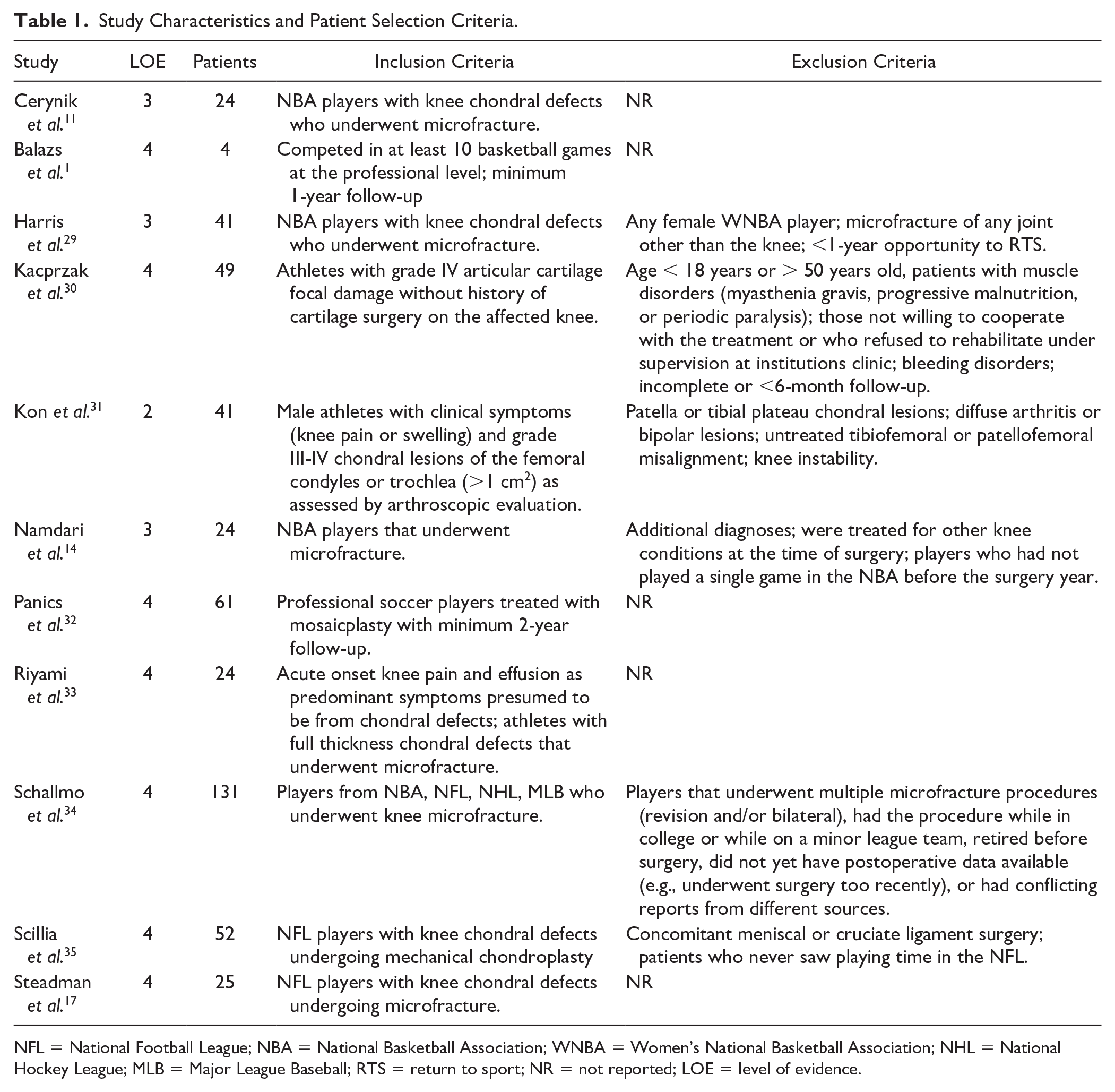
NFL = National Football League; NBA = National Basketball Association; WNBA = Women’s National Basketball Association; NHL = National Hockey League; MLB = Major League Baseball; RTS = return to sport; NR = not reported; LOE = level of evidence.
Lesion characteristics were variably reported. More than half (n = 6; 54.5%) of studies did not report cartilage lesion location or size. Of the remaining 5 studies comprising 200 professional athletes with 210 cartilage defects,17,30-33 the distribution of the locations of cartilage lesions were as follows: medial or lateral femoral condyles: 174 (82.9%); trochlea: 18 (8.6%); medial or lateral tibial plateaus: 9 (4.3%); multiple-surfaces or bipolar: 3 (1.4%); and patella: 6 (3.5%). The mean defect size was 2.4 ± 0.7 (range, 1.9-3.8) cm2.
Methodological Quality and Bias Assessment
The mean MINORS score among all studies was 17.2 ± 4.1 For the 6 noncomparative studies, the mean MINORS score was 13.0 ± 0.82 For the remaining 5 comparative studies, the mean MINORS score was 20.6 ± 0.89 Overall, included studies demonstrated a low risk of bias, with the most frequent concerns pertaining to prospective calculation of study samples and loss to follow-up exceeding 5% ( Fig. 2 ).
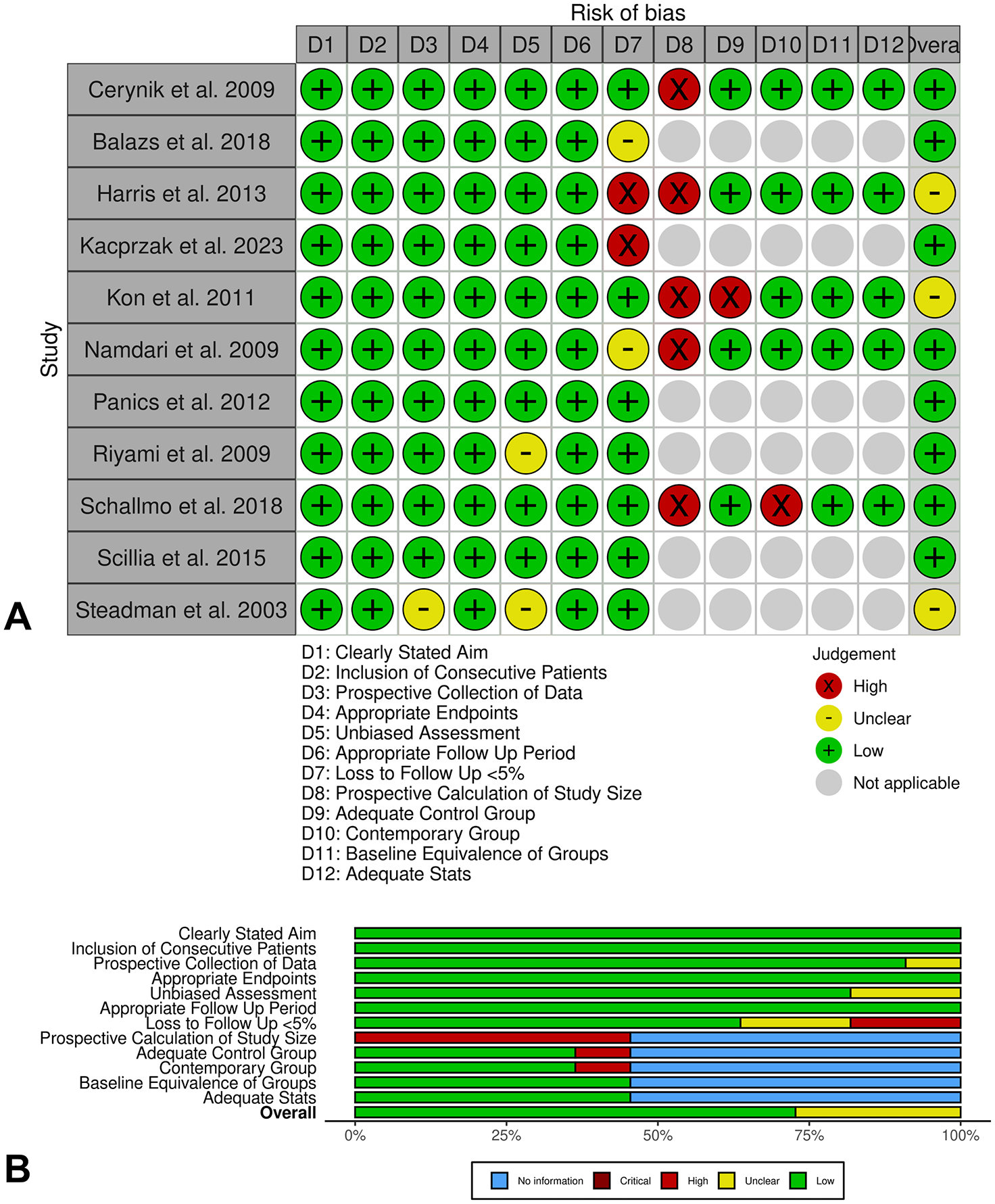
Traffic light (
Return to Sport Analysis
All eleven studies reported the proportion of professional athletes that successfully returned to sport. Four studies reported on solely NBA players,1,11,14,29 2 on solely NFL players,17,35 and 2 solely on soccer players.31,32 One study reported on a cohort of professional football, basketball, and handball players; 30 one on professional football and rugby players; 33 and one on a combined cohort of MLB, NBA, NFL, and NHL players. 34 The pooled RTS rate was 84.3% (95% confidence interval [CI]: 75.4%-91.8%; Fig. 3 ) at a mean 39.9 weeks after surgical intervention. Timing of RTS ranged widely across studies, with the shortest average RTS time being 12 weeks and the longest mean RTS time being 104 weeks.
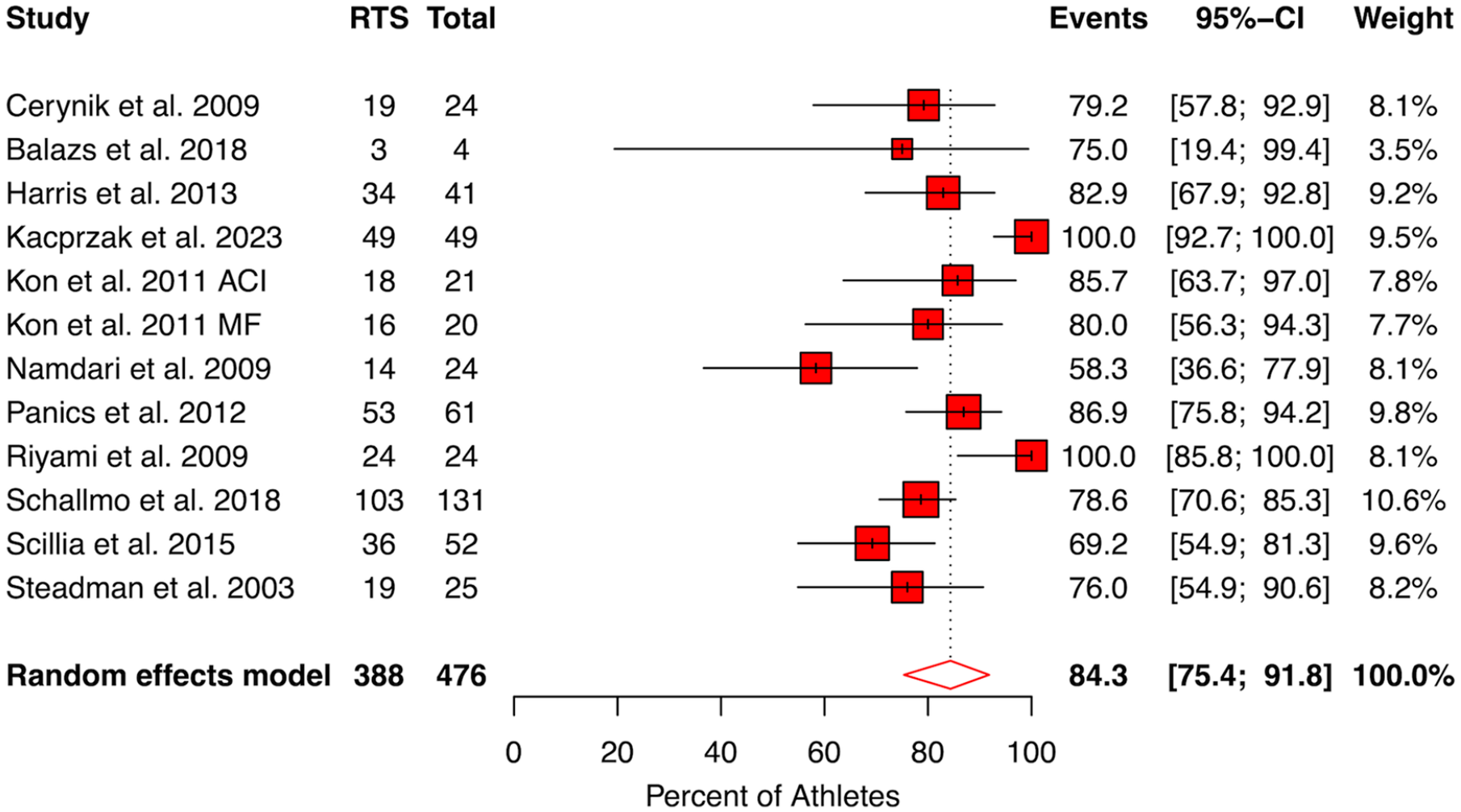
Forest plot depicting random-effects model for proportion of professional athletes that returned to sport after undergoing cartilage restoration procedures for the knee. Events indicated the percentage of patients that returned to sport; 95% CI, 95% confidence interval. The x-axis depicts incremental changes in the percentage of patients returning to sport. Red boxes represent the weighted contribution of each study, with the horizontal black lines representing the 95% CI of the treatment estimate. RTS, return to sport. The heterogeneity is I2 = 79.3% (64.4%-87.9%).
Six studies disclosed at least one level of magnitude of RTS in terms of the postoperative level of play achieved (lower than pre-injury level, same as pre-injury level, or greater than pre-injury level).11,29-32 Cerynik et al. 11 and Harris et al., 29 both of whom studied homogenous cohorts of NBA players that underwent microfracture, reported that 100% of NBA players returned to levels of play that were lower than their pre-injury level. Kacprzak et al. 30 reported that all patients in their cohort that played professional football, basketball, or handball returned to their same pre-injury level of play. Both Panics et al. 32 and Kon et al. 31 only reported whether or not professional soccer players returned to their same pre-injury level of play. Panics et al. reported that of the 87% of athletes that achieved RTS, 67% of them returned at the same level. In the study by Kon et al., of the patients that underwent microfracture, 75% returned to their pre-injury level of play, while 67% of those who underwent ACI returned to their pre-injury level of play. Balazs et al. 1 reported that there was a general trend toward decreasing player productivity in the NBA after OCA, but did not separate these statistics for professional athletes specifically.
The definition of RTS was only provided in 6 studies,1,11,17,29,34,35 while the criteria for RTS was only reported in 2 studies,1,35 suggesting limited transparency ( Table 2 ). Of the studies providing RTS definitions, the threshold for achieving this milestone was modest, with all studies considering a successful RTS as participation in a single game regardless of whether the athlete continued play. In the 2 studies that provided RTS criteria, the milestones were vague, consisting of the achievement of subjectively symmetric range of motion and strength or progression through performance assessments. No studies mentioned specifics of formal RTS testing protocols or a minimum timeline
Return to Sport (RTS) Definitions and Criteria Among Included Studies.

NBA = National Basketball Association; NFL = National Football League; NR = not reported.
Objective Lesion Evaluations: Imaging and Second-Look Arthroscopy
Only 2 studies routinely obtained magnetic resonance imaging (MRI) in the postoperative period; one study did not provide objective MRI assessments of the appearance of reparative tissue and describe MRI appearances narratively, 30 while the remaining study performed objective grading using a modified Henderson classification. Riyami et al. 33 obtained MRI at 6, 12, and 18 months postoperatively after microfracture surgery. At 6 months, 37.5% of patients demonstrated nearly complete or complete healing, while 33.3% demonstrated no healing, and 29.2% incomplete healing. At 12 months, 83.3% demonstrated nearly complete or complete healing, no patients demonstrated no healing, and 16.7% demonstrated incomplete healing. At 18 months, 87.5% demonstrated nearly complete or complete healing, 12.5% demonstrated incomplete healing, and no patients demonstrated no healing.
Interestingly, these authors stated that 10/24 patients underwent second look arthroscopy at a mean 5.8 months postoperatively due to requests from team medics and managers for proof of lesion healing before allowing the players to be considered for RTS. The authors graded second look assessments with the ICRS score and reported the following: grade I (firm lesion) was observed in 2/10 subjects; grade II (soft on probing) was observed in 6/10 patients; and grade III (“abnormal”) was observed in 2/10 patients.
Adverse Events
Five studies reported that either reoperations or complications occurred postoperatively, although two did not specifically report the frequency or type of complications.1,32 Therefore, data on adverse events was available for 3 studies.29-31 In these studies, comprising 131 professional athletes, a total of 6 reoperations were reported for residual symptoms related to persistent cartilage defects, resulting in a pooled reoperation rate of 4.6%.
Discussion
The main findings of the current study are as follows: (1) a high overall RTS rate was observed for professional athletes, with pooled data estimating that 84.3% may expect to return to professional competition after cartilage restoration surgery of the knee; (2) the primary intervention utilized for the treatment of chondral and osteochondral lesions of the knee in professional athletes was microfracture, with all studies exploring a variation of microfracture as treatment; (3) female athletes are poorly represented in cartilage literature examining RTS in professional athletes; and (4) important episode of care characteristics that may influence outcomes and interpretation of results, such as lesion size, lesion location, rehabilitation and clearance protocols, and objective imaging assessments of the reparative tissue, are infrequently and variably reported in the literature.
The majority of professional athletes were reported to RTS at the professional level at a mean 39.9 weeks after cartilage restoration surgery of the knee. A recent systematic review by Hurley et al. reported that the pooled rate of return to play ranged between 77.4% and 88.2% depending on treatment. Specifically, the rate of return to play after microfracture was 77.4% and ranged between 51.7% and 95%. In the current study, the specific RTS rate was 84.3%, which may reflect the physical durability and mental fortitude of professional athletes, as well as the contractual and social demands of returning to play. However, of studies reporting level of return, the majority indicated that professional athletes generally return to a lower level of play than their pre-injury state, which is consistent with prior literature and may reflect the requirement for a high level of function in professional sports. 24 Interestingly, all but 2 studies investigated a variation of microfracture as treatment. In an epidemiologic study of knee cartilage injury and management across FIFA Medical Centers of Excellence, Marom et al. 7 reported that the most common operative treatment employed across 15 centers from 5 continents was microfracture. It is plausible that the narrow scope of treatments published in the literature is a function of the delicate balance between organizational pressures for professional athletes to RTS in an expeditious manner and the necessity to surgically treat a symptomatic cartilage defect that is limiting a player’s performance. Indeed, player absence may have substantial consequences on a team’s performance, which has financial implications, and other forms of cartilage treatment including osteochondral grafting or autologous cell transplantation often require prolonged rehabilitation phases which would not be feasible in this high-demand environment. Regardless, there is an important need to understand the clinical treatment response and propensity for RTS in professional athletes who are subjected to other contemporary forms of cartilage restoration surgery such as osteochondral autograft transplantation and matrix-assisted chondrocyte implantation.
In studies investigating RTS in professional athletes after cartilage restoration surgery of the knee, less than 4% of patients were female. Unfortunately, female athletes have been repeatedly excluded from the focus of sports medicine outcomes research.36,37 Prior systematic reviews have also reported that females represent a minority in certain literature, precluding the accumulation of important evidence for therapeutic treatments, and that there exists a “gender blindness” for various sports medicine-related conditions.38,39 It appears that such disparities are also present in the cartilage field, and the lack of representation is concerning and warrants attention. The absence of sufficient data limits our ability to identify optimal treatment and to provide prognostic information for high-level female athletes. Attention should be raised to this limitation in the literature, and there is currently a strong need to provide high-quality evidence on the treatment and outcomes of professional women athletes with cartilage defects of the knee across a variety of sports.
Important considerations when performing cartilage restoration surgery and guiding athletes through rehabilitation, such as lesion size, location, RTS clearance protocols, and objective imaging assessments, were not commonly disclosed or were vague. This lack of transparency precludes study generalizability and presents challenges when attempting to extrapolate data to real-world clinical practice. This finding is in accordance with prior literature on cartilage restoration surgery and emphasizes the sustained need for improvements in reporting and transparency. Jones et al. 40 reviewed 113 clinical studies on articular cartilage restoration of the knee over a 5-year period and reported that 32.7% of articles did not report how lesion size was measured, while 11.5% did not report units of measurement. Furthermore, less than half of studies reported the depth when sizing osteochondral defects, and the lesion sizing method was highly variable. It is important to recognize the limitations inherent in contemporary literature in order to propose guidelines for improved reporting. The limitations identified in this study suggest the need for an expert consensus on minimum reporting standards concerning cartilage restoration outcome studies in the professional athlete population.
Limitations
Several important limitations should be considered. First, factors that may be important in the assessment of RTS such as concomitant procedures, prior surgeries, lesion characteristics, and rehabilitation criteria were infrequently and variably reported. However, this lack of reporting highlights an important area of concern in this literature that needs to be addressed in order to advance the field of cartilage surgery for athletes. Second, the definitions of RTS were variable and in some instances vague; despite this, a common theme was a return to a professional sporting event, providing some unifying theme, though future investigations should consider more detailed and refined definitions of RTS in this high-demand population. Finally, studies were retrospective and therefore inherent biases in these studies may influence the results synthesized in the current review.
Conclusions
Though the majority of professional athletes are reported to achieve a successful RTS after cartilage restoration surgery of the knee, the literature predominantly reflects microfracture treatment. Current limitations in this literature include a substantial lack of female representation and infrequent reporting of cartilage lesion characteristics, rehabilitation and RTS criteria, and objective imaging assessments of reparative tissue. Investigations concerning other contemporary cartilage treatments, studies focusing on female professional athletes, and improved transparency in reporting are needed.
Footnotes
Acknowledgements and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was exempt from institutional board approval.