
Abstract
Objective
To perform a scoping literature review evaluating and reporting on outcomes and return to pivoting sports after cartilage procedures. For this review, the following cartilage procedures were evaluated: microfracture, osteochondral autograft transplantation (OAT), osteochondral allograft transplantation (OCA), and autologous chondrocyte implantation (ACI).
Design
The scoping review incorporated articles identified using PubMed (MEDLINE), CINAHL, and Cochrane Central Register of Controlled Trials. Screening of reference lists of included studies and forward citation tracking were performed to identify additional studies. Reported on return to pivoting sports after cartilage surgery written in English language.
Results
Sixteen studies fulfilled the inclusion criteria. The return to sports (RTS) rates after microfracture ranged from 44% to 83%, and to preinjury level from 25% to 75%. The RTS rates after OAT ranged from 87% to 100%, and to preinjury level from 67% to 93%. The RTS rates after OCA ranged from 77% to 80%, and to preinjury level 64%. The RTS rates after ACI ranged from 33% to 96%, and to preinjury level from 26% to 67%.
Conclusions
There was a high heterogeneity and range in rates of RTS in athletes participating in pivoting sports. Most studies reported high rates of RTS; however, return to preinjury level was lower. These data may be important to clinicians in shared decision making on the type of procedure to be performed and counseling pivoting sports athletes on prognosis and expected RTS rates.
Introduction
The prevalence of knee cartilage injuries is alarmingly high among athletes, occurring in up to 36%, which is more than twice than that in the general population. 1 This high prevalence may be due to an acute injury or repetitive microtrauma especially in pivoting and high-impact sports such as soccer and basketball.2 -4 Although these cartilage injuries may initially be treated conservatively, injured cartilage has poor healing capacity, and the resulting pain and dysfunction can lead to poor sports performance. 5 There is potential for progressive joint cartilage degeneration without any treatment, 6 ultimately leading to development of early post-traumatic osteoarthritis (PTOA). Furthermore, athletes may require surgical treatment of focal cartilage injuries to restore function and increase probability of returning to sports. The current main treatment options available for the management of focal chondral defects include microfracture, osteochondral autograft transplantation (OAT), osteochondral allograft transplantation (OCA), and autologous chondrocyte implantation (ACI).7 -10
For athletes who wish to return to competitive level, the probability of being able to return to sports (RTS) after surgery is of particular importance. Therefore, the RTS outcome is an important variable to consider when selecting cartilage treatment for both clinicians and athletes. 11 Several meta-analyses and systematic reviews have reported the rates of return to play for all sports following these surgical management of focal knee articular lesions.12 -14 However, there is significant variability in how RTS is defined in the literature currently. 11 The outcome is specific to individual athletes and focuses on their sport-specific goals. The probability of RTS for an athlete competing in pivoting sports or running activities may be different, because the cartilage load is dependent on the type of sports activity. Therefore, the RTS among all sports may not be an appropriate outcome variable to estimate an accurate outcome prediction for an athlete participating in pivoting sports.11,15,16
To help the surgeon and patient, this review focused on RTS after focal chondral lesion surgery in pivoting sports where the prevalence of cartilage injuries and the cartilage load is particularly high.2 -4 The purpose of this scoping review was to identify gaps in the current research and present available evidence for rates of RTS after cartilage procedures in pivoting sports athletes. The hypothesis of this study was that the RTS in pivoting sports is lower than RTS in all sports. Knowing this information may enable clinicians to better counsel athletes on RTS rates.
Methods
As no research has been conducted in this area, a scoping review was conducted which is superior to a systematic review in addressing the exploratory research question.17,18 We followed the methodological framework proposed by Arksey and O’Malley and the Joanna Briggs Institute when conducting and reporting this scoping review.17 -19
Our research question was “What are the rates of RTS among pivoting sports athletes after cartilage procedures of the knee joint?”
The following databases were used: PubMed (MEDLINE), CINAHL, and Cochrane Central Register of Controlled Trials by 2 authors (S.T. and G.M.) independently on February 20, 2022. The same authors also independently performed all aspects of the study selection. The search period was from January 2002 to February 2022. The following search words were used: “(cartilage OR articular cartilage OR chondral OR chondrocyte OR articular OR osteoarticular OR osteochondral) AND (transplant OR transplantation OR allograft OR autograft OR autologous OR implantation OR implant OR mosaicplasty OR oat OR oats OR microfracture OR maci OR aci OR caci OR restore OR repair) AND (athlete OR athletic OR sport OR activity) AND (knee).” All studies identified were reviewed independently by the authors and checked for potentially inclusive references. We also screened the reference lists of included studies and conducted forward citation tracking.
The inclusion criteria included the following:
primary research studies that evaluated the RTS after cartilage repair;
English language;
human subjects;
patients with focal nearly full- or full-thickness (grade III or IV) chondral and osteochondral defects or osteochondritis dissecans of the femoral condyles, trochlea, patella, or tibial plateau;
results of studies after the following surgical interventions: microfracture, OAT, OCA, or ACI;
subjects are limited in athletes involved in pivoting sports. Pivoting sport was defined as level I sports according to Hefti et al. and included soccer, handball, basketball, tennis, and other ball games with rapid start and stop movements,20,21
minimum follow-up of 12 months.
Data extraction was performed independently by 2 investigators. A template was used for data extraction that included study design, participants, inclusion/exclusion criteria, intervention, outcome measures (number of athletes, mean defect size, mean age, location of the cartilage injury, mean number of previous operations, RTS, return to preinjury level, level of sports), and conclusion. Although some studies defined RTS and return to preinjury level and some did not, this review collected all studies that stated RTS and return to preinjury level. The internal validity of included studies was not conducted because we contend that our descriptive summary is unlikely to be adversely influenced by the internal validity of the included studies.
Results
The flow chart of study selection is detailed in Figure 1. We selected and included 16 studies in our scoping review. Seven studies reported on microfracture, 2 studies on OAT, 2 studies on OCA, 3 studies on ACI, 1 study on microfracture and OAT, and 1 study on microfracture and ACI. Outcomes of each procedure are reported below.
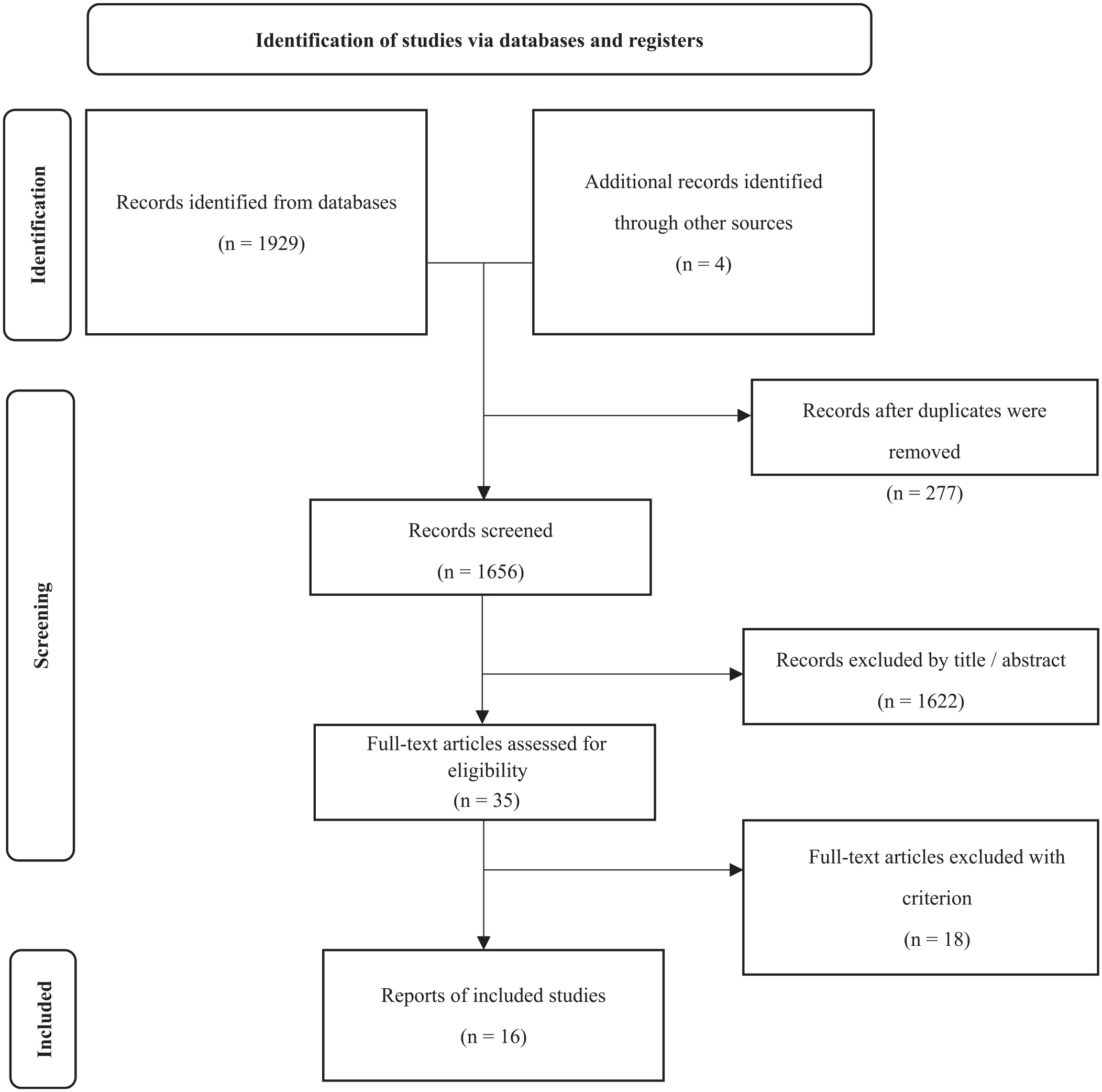
PRISMA 2020 flow diagram showing the study selection process.
Microfracture
Details of the included variables for studies reporting on microfracture procedure in pivoting sports are listed in Table 1. RTS and return to preinjury level was reported in 44% to 83% and 25% to 75% of the patients, respectively. The reported time to RTS varied between 6.2 and 10 months, and the mean defect size varied from 1.9 to 4.9 cm2. The most commonly reported location of cartilage surgery was at medial femoral condyle (MFC; 53%-89%), and mean number of previous operations varied from 0.5 to 0.9 times.
Included Studies on RTS in Pivoting Athletes after Microfracture Procedure.
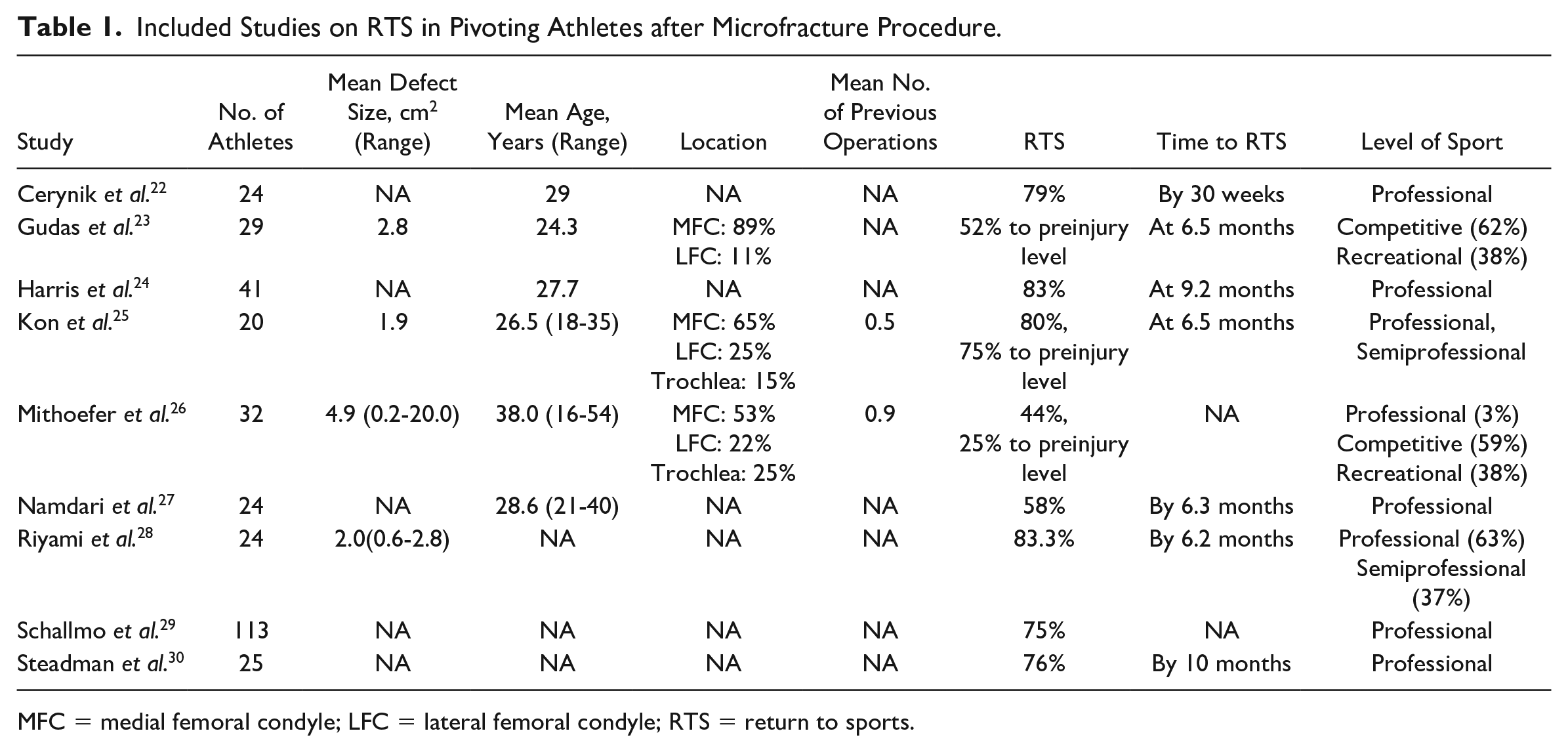
MFC = medial femoral condyle; LFC = lateral femoral condyle; RTS = return to sports.
OAT
Details of the included variables for studies reporting on OAT procedure in pivoting sports are listed in Table 2. RTS and return to preinjury level was reported in 87% to 100% and 67% to 93% of the patients, respectively. The reported time to RTS varied between 11.8 weeks and 6.5 months, and the mean defect size varied from 1.34 to 2.9 cm2. The most commonly reported location of cartilage injury was at MFC between 62% and 79%, and mean number of previous operations was not reported in the included studies.
Included Studies on RTS in Pivoting Athletes after Osteochondral Autograft Transplantation (OAT) Procedure.
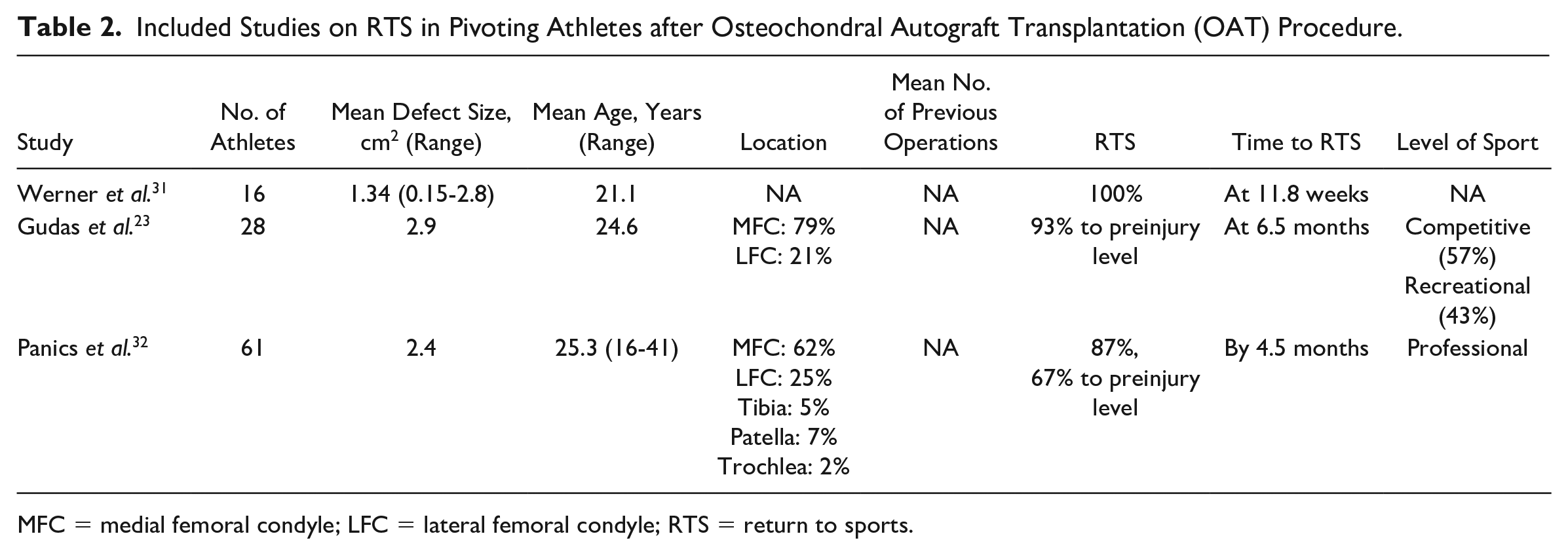
MFC = medial femoral condyle; LFC = lateral femoral condyle; RTS = return to sports.
OCA
Details of the included variables for studies reporting on OCA procedure in pivoting sports are listed in Table 3. RTS was reported in 77% to 80%, and return to preinjury level was only reported by one study, and was found in 64% of the patients. The reported time to RTS varied between 7.9 and 20 months, and the mean defect size varied from 4.5 to 5.1 cm2. The most commonly reported location of cartilage injury was at MFC (50%) and lateral femoral condyle (LFC; 43%), and mean number of previous operations varied from 1.0 to 1.7 times.
Included Studies Reporting on RTS in Pivoting Sports Athletes after Osteochondral Allograft Transplantation (OCA) Procedure.
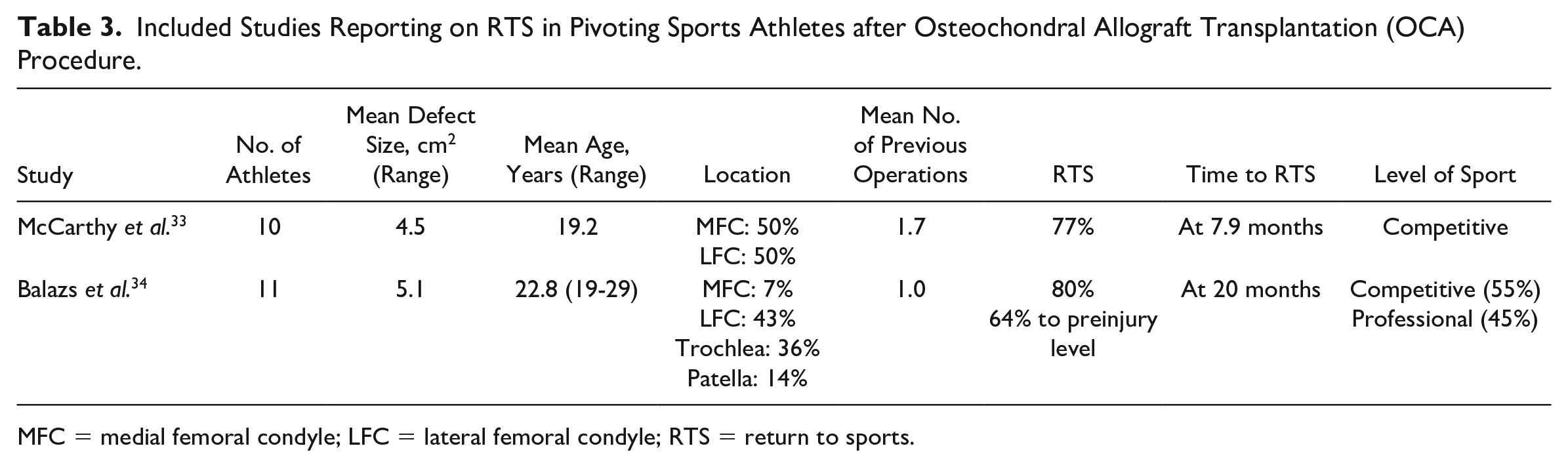
MFC = medial femoral condyle; LFC = lateral femoral condyle; RTS = return to sports.
ACI
Details of the included variables for studies reporting on ACI procedure in pivoting sports are listed in Table 4. RTS and return to preinjury level was reported in 33% to 96% and 26% to 67% of the patients, respectively. The reported time to RTS was 10.2 months, and the mean defect size varied from 2.1 to 6.4 cm2. The most commonly reported location of cartilage injury was at MFC between 48% and 67%, and mean number of previous operations varied from 0.6 to 2.7 times.
Included Studies on RTS in Pivoting Sports Athletes after Autologous Chondrocyte Implantation (ACI) Procedure.
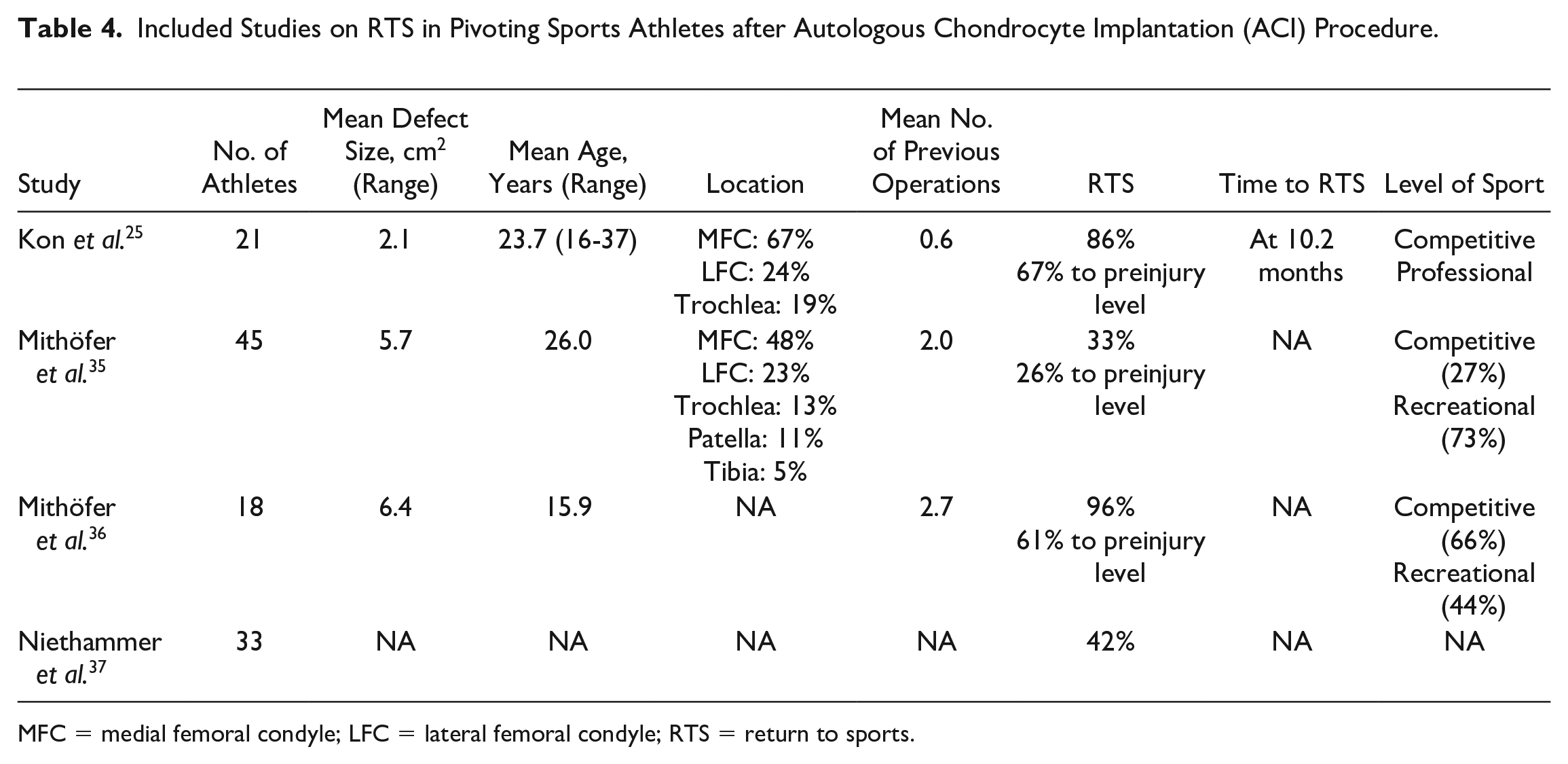
MFC = medial femoral condyle; LFC = lateral femoral condyle; RTS = return to sports.
Discussion
This scoping review provides an overview of reported rates of RTS for pivoting sports athletes after undergoing the most common cartilage procedures. There was a high range in terms of rates of RTS and return to preinjury level for all procedures in the included studies. Most studies reported high rates of RTS; however, return to preinjury level was lower. RTS with microfracture in pivoting sports was not higher compared with other techniques and OAT is expected to have the highest RTS in pivoting sports. There was a high heterogeneity in regard to age, chondral lesion size, location of cartilage injury, number of previous surgeries, and level of sports, which may explain the variations in outcome.
Microfracture has been available to patients for several decades and has become one of the main first-line treatments for cartilage lesions.38 -40 It is performed by puncturing holes in the subchondral layer to allow for release of precursor cells that can reorganize to form fibrocartilage. The advantage of this technique is its low cost and technical ease. Other advantages are that the patient can return to competition relatively quickly, in 8 to 9 months, and does not require comprehensive postoperative rehabilitation.12,13 The main disadvantage of microfracture is a lack of restoration of hyaline cartilage, which is best suited for handling typical joint forces. Relatively large lesions, larger than 2 cm2 and lesions in the subchondral bone have been reported to have poor postoperative outcomes. 12 Another concern is that despite good short-term results including International Knee Documentation Committee (IKDC), Lysholm, and Tegner scores, long-term results beyond 5 years have been reported to deteriorate.41,42
A systematic review including 529 athletes after microfracture participating in all sports activities reported that the RTS and return to preinjury level was 75% and 69%, respectively. 12 The mean defect size was relatively small (2.9 cm2), and the average time to RTS was 8.1 months. Similarly, a meta-analysis including 858 athletes after microfracture on all sports reported a 58% RTS. 13 The mean defect size was 3.1 cm2, and the average time to RTS was 9.1 months. In this study limited to athletes participating in pivoting sports, the RTS rates after microfracture varied, ranging from 44% to 83%, and RTS to preinjury level were reported in 25% to 75% of the patients. Studies that included professional basketball players reported RTS rates of 58%, 27 79%, 22 82%, 29 and 83% 24 after microfracture for chondral lesions. Interestingly, Schallmo et al. 29 reported that in basketball and football, 18% and 29% of players were unable to RTS, while in baseball, 100% of players returned to sports. This may be due to the game difference in those sports where a baseball athlete is exposed to less jumping, running, and cutting movements compared with basketball and soccer athletes.
The OAT techniques involve harvesting a plug of cartilage from the patient’s own joint, usually the knee, and transplanting that plug into the defect site. This can be performed as 1 single circular plug or as multiple circular plugs known as a mosaicplasty.43,44 The advantage of this technique is that OAT has a high healing potential because it uses the patient’s own tissues, allowing bone to integrate immediately. In addition, the joint surface can be covered with hyaline cartilage instead of fibrocartilage as obtained after microfracture. However, these techniques are limited to small defects given the risk of donor site morbidity. 43
A systematic review among all sports activities of 139 athletes found that the RTS for OAT was 89%, and 70% returned to the preinjury level. 12 The mean defect size was relatively small (2.6 cm2), and the average time to RTS was 7.1 months. Similarly, a meta-analysis including 261 athletes after OAT among all sports reported a 93% RTS rate. The mean defect size was 2.6 cm2, and the average time to RTS was 5.2 months. 13 In this study limited to pivoting sports, we found RTS rates ranging from 87% to 100% and RTS to preinjury level were from 67% to 93%. This suggests that the OAT procedure may offer acceptable results for high-demand athletes. Werner et al. 31 reported that 100% of the patients with OAT returned to pivoting sports. One of the reasons for this high rate of RTS in their study might be the size of cartilage defects (mean: 1.34 cm2) which was the smallest in the literature of this review. In the study conducted by Pánics et al. 32 examining soccer players undergoing OAT, the average lesion size in athletes who returned to soccer was significantly smaller than in those who were unable to return (2.2 vs. 3.0 cm2). Based on these results, the size of the chondral lesion may play an important role in the prognosis and rates of RTS after OAT procedures.
OCA has been an important treatment option for larger cartilage lesions than OAT.45,46 In this technique, a size-matched plug graft of cartilage and bone is obtained from a cadaver specimen to treat the articular defect in the patients similar to the implantation of the OAT procedure. Similar to OAT, the immediate implantation of viable bone and cartilage surfaces offers significant advantages over other techniques. In addition, this technique avoids donor site morbidity and restores hyaline cartilage in large and deep chondral and osteochondral lesions. However, OCA grafts are expensive and in limited supply, and are restricted in many countries. In addition, there is increased concern about graft viability, matrix composition, and mechanical properties. Time constraints are another issue that may limit the use of osteochondral allografts because hypothermically stored cartilage grafts should be implanted within 14 to 21 days of graft harvest. 46
A systematic review among all sports activities of 43 athletes found that the RTS for OCA was 88%, where 79% returned to the preinjury level. 12 The mean defect size was relatively large (7.3 cm2), and the average time to RTS was 9.6 months. Similarly, a meta-analysis including 96 athletes after OCA among all sports reported an 88% RTS. 13 The mean defect size was 6.5 cm2, and the average time to RTS was 9.6 months. We found slightly lower reported RTS rates (77%-80%) among athletes participating in pivoting sports. Nevertheless, these results indicate that even with a large cartilage defect, a high rate of RTS can be expected with OCA procedures for a high-demand athlete.
ACI is a 2-stage technique for hyaline-like repair of full-thickness articular cartilage lesions. The native chondrocytes are harvested arthroscopically and cultured under standardized conditions.47,48 At a second open procedure, the cell suspension is implanted on cartilage defects. There ACI has been developed in multiple generations. First-generation technique was performed in a second open procedure under a periosteal patch acquired from the proximal tibia and sutured to the surrounding stable cartilage margins with the cambium layer facing toward the defect. In the second generation, the technique was using a bioabsorbable collagen membrane which was developed as a temporary cover of the treated defect instead of the autologous periosteal patch to avoid the frequent complication of graft hypertrophy and the associated risk from delamination or requirement for surgical chondroplasty of the hypertropic graft. The third-generation ACI techniques use biodegradable membranes or scaffolds to temporarily support the chondrocytes until they are replaced by neocartilage matrix components synthesized from the implanted cells. ACI can be used to deal with relatively large defects. The limitations of this technique are requiring 2-stage surgery, high cost, its invasiveness, and prolonged postoperative rehabilitation.47 -49
A systematic review among all sports activities of 259 athletes found that the RTS for ACI was 84%, returning to the preinjury levels was 76%. 12 The mean defect size was relatively large (5.1 cm2), and the average time to RTS was 16.0 months. Similarly, a meta-analysis including 1,334 athletes after ACI in all sports reported an 82% RTS. 13 The mean defect size was 4.5 cm2, and the average time to RTS was 11.8 months. This RTS result is high among every technique and the average time to RTS was long.12,13 We found that RTS after ACI varied between 33% and 96% 25 ,35 -37 and RTS to preinjury level were from 26% to 67% in high-demand pivoting athletes. This may be due to heterogeneity for patient characteristics and generation of surgical technics. Pivoting sports may have a lower expected return-to-play rate compared with other sports. Niethammer et al. 37 reported that RTS after third-generation ACI resulted in 96% in all sports, compared with 42% in pivoting sports. Pestka et al. 50 also reported that although there was 73% RTS after second-generation ACI across all sports, there was a small RTS to elite sports (0.8%). It seems that returning to sports with high activity levels is difficult.37,50 However, there was a tendency for the RTS to be higher when the players’ competition level was higher. Mithoefer reports that the overall return rate to soccer was 33%, but the return rate for professional players was significantly better at 83%, compared with 16% for recreational players. 51 This may be due to differences in patient adaptability to competition or compliance with rehabilitation protocols.
RTS is a critical variable for patients who are involved in playing sports. For clinicians and athletes, these data are used as a basis for selecting treatment and making prospective predictions. However, simultaneously, RTS is a complex and ambiguous variable throughout the literature. In cartilage repair treatment, there are few situations in which all patients are involved in playing sports preoperatively, and a few studies collect only athletes. Not only are the disciplines in which they participate not consistent, but the definition of what level constitutes an RTS is also not well defined. It would be useful for both clinicians and athletes to have a report of RTS under a few defined conditions. 11
Based on this scoping review, RTS with microfracture in pivoting sports was not higher compared with other techniques similar to what has been described in the literature previously for all sports. In contrast, our findings suggest that OAT is expected to have the highest RTS in pivoting sports. In addition, it has been reported that athletes RTS faster, especially, when the cartilage deficit is small. 32 In pivoting sports with large cartilage defects, OCA and ACI are treatments to consider. In clinical practice, ACI may be chosen in many cases, because OCA has many limitations in its use. There are still not enough data on the size of the lesion to decide between ACI and OAT. 52 In general, there is a paucity of randomized studies comparing this treatment technique. Although Horas et al. 52 and Bentley et al. 53 compared the postoperative results in both groups and reported that there was no significant difference in short-term results, there are 2 reports that the ACI outperforms the OAT in 10-year outcomes.54,55 There are no studies yet comparing OAT and ACI regarding RTS. Further investigation is needed in the future.
We found that the most common location of the cartilage procedure of the included studies was on the medial or lateral femoral condyle. Only 5 included studies reported on RTS after procedures to the patellofemoral joint and tibial plateau, and the proportion of those patients were small. In a systematic review, Donoso et al. 56 reported on the results of cartilage treatment for patellofemoral lesion. Two of the studies reported RTS for all sports, and almost all of the athletes reported being able to return to the same level. The meta-analysis by Hinckel et al. 57 reported that OAT may be an optimal technique for small patellofemoral lesions and ACI may be better for large lesions. For tibial lesion, Melugin et al. 58 reported that the results were good for treatments except for microfracture.
This scoping review has some limitations. First limitation of this study was the restricted data available for each treatment, which limits the conclusions. For some cartilage procedures, there was only one reference paper. Second, there was no information on concomitant procedures for meniscus, alignment, or ligament in this study. These procedures could affect the RTS of the study. Based on these limitations, prospective comparative studies about RTS in pivoting sports are desirable in the future.
In this review, the RTS in pivoting sports was evaluated. RTS is an ambiguous variable that is confounded by many factors. Future research should take into account other factors that may have influenced the timing of RTS, such as what level of sport the athlete returned to, whether participation in the sport is still enjoyable, economic motivation, and whether it is a team sport or an individual sport.
Conclusion
There was a high heterogeneity and range in rates of RTS in athletes participating in pivoting sports. Most studies reported high rates of RTS; however, return to preinjury level was lower. RTS with microfracture in pivoting sports was not higher compared with other techniques, and OAT is expected to have the highest RTS in pivoting sports. These data may be important to clinicians in shared decision making on the type of procedure to be performed and counseling pivoting sports athletes on prognosis and expected RTS rates.
Footnotes
Author Contributions
S.T. and L.E. were responsible for the conception of the study and along with G.M. developed the search strategy. S.T. and G.M. executed the search strategy and independently reviewed records, assessed the methodological quality of included studies, and extracted data. S.T. was responsible for the first draft of the manuscript. All authors contributed to the interpretation of the findings, critical revision of the manuscript, and reviewed the document prior to submission.
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Not required.
Patient Involvement
No
Data Sharing Statement
Authors can confirm that all relevant data are included in the article.