
Abstract
Objective
To investigate the cytokine release profile and histological response of human cartilage after exposure to autologous conditioned serum (ACS) and freeze-dried allogenic conditioned serum (FD-CS).
Design
Cartilage explants were collected from 6 patients undergoing total knee arthroplasty. ACS and FD-CS were created from patient serum samples. Cartilage samples were divided into 6 groups: (1) untreated control, (2) ACS, (3) FD-CS, (4) untreated interleukin (IL)-1β (5 ng/ml), (5) IL-1β + ACS, and (6) IL-1β + FD-CS. After 12 days, cartilage samples were analyzed with glycosaminoglycan (GAG) concentration normalized to wet weight while comparing cytokine concentrations, and histological scoring.
Results
There was a significant decrease in pathology scoring for ACS (P = 0.0368) and FD-CS (P = 0.0368) in the IL-1β injury groups compared with the untreated IL-1β insult group. ACS and FD-CS significantly mitigate the IL-1β induced increase in basic fibroblast growth factor (bFGF) (P = 0.0009 and P = 0.0002, respectively). FD-CS showed a significant decrease in IL-1β concentration in the presence of IL-1β insult compared with the untreated IL-1β group (P < 0.0001). ACS-treated samples had significantly higher concentration of tumor necrosis factor (TNF)-α independent of IL-1β when compared with samples not treated with biologics (P = 0.0053).
Conclusions
Explanted osteoarthritic cartilage responds favorably and equivalently to treatment with ACS and FD-CS from a histological perspective. Both ACS and FD-CS were able to mitigate the IL-1β-induced increases in bFGF and FD-CS lowered IL-1β concentration while increasing interleukin-1 receptor antagonist (IL-1Ra) concentration. Although the cytokine profile of cartilage tissue explants treated with FD-CS appears to be different than that of ACS, this difference does not seem to affect biologic activity of FD-CS.
Keywords
Introduction
Osteoarthritis (OA) is a chronic orthopedic condition carrying significant morbidity, disability, reductions in quality of life, and financial burden affecting nearly 30 million people in the United States alone.1,2 The knee is the most common anatomical location affected, comprising 80% of the prevalence worldwide. 3 As a result, clinicians are continually striving to improve treatment and outcomes for this common disease. Prior to definitive surgical treatment including total knee arthroplasty (TKA) or unicompartmental knee arthroplasty (UKA), conservative measures serve as the mainstay of initial treatment. One of the most popular nonoperative treatment options is intra-articular injections, as they can be delivered at low risk to the patient in the clinic-based setting and provide short-term reductions in pain and improved joint functionality.4-7 Traditionally, injections have included corticosteroid with local anesthetic and hyaluronic acid (HA), but more recent investigations have delved into the potential benefits of biologic injections such as platelet rich plasma (PRP) and bone marrow aspirate concentrate (BMAC).
Another more recent biologic injection being studied is autologous conditioned serum (ACS). ACS is a blood-derived injectable product similar to PRP primarily used in Europe, as it is not currently approved for clinical use in the United States.8,9 Owing to its favorable anti-inflammatory cytokine profile, ACS has been shown to significantly decrease pathologic symptoms in OA affected knee joints in humans. 10 In 2 randomized control trials examining intra-articular injections for knee OA, ACS has shown superior patient-reported outcomes (PROs) compared with HA and saline injections, promoting both a reduction in OA symptoms and an improvement in quality of life.11,12 Furthermore, in a systematic review and meta-analysis of randomized control trials by Anil et al., 13 the authors examined a host of intra-articular knee injection types and found ACS demonstrated better pain and PROs compared with saline, HA, BMAC, and PRP.
Although positive clinical results have been seen with the clinical use of commercial ACS products, there are limitations currently precluding its widespread acceptance and use. These challenges include the preparation time and storage requirements, patient variability in both pro- and anti-inflammatory cytokine profiles, and lack of regulatory approval of a commercial product in the United States. Ideally, these needs could be met with the development of an allogenic freeze-dried ACS product with an unaltered cytokine profile that remains stable at room temperature and would allow for easy storage, transport, and delivery to clinical settings. ACS has been used extensively in veterinary medicine and the freeze-dried allogeneic conditioned serum has undergone in vitro 14 as well as testing 15 and a current equine clinical trial in knee joints is underway.
The purpose of this study is to (1) compare the cytokine release profile of human cartilage in response to treatment with freeze-dried allogenic conditioned serum (FD-CS) to fresh ACS and (2) to investigate the response of human knee cartilage after exposure to FD-CS and ACS to determine whether freeze-drying (lyophilization) affects the biological activity of conditioned serum products. We hypothesize that treatment with FD-CS results in a comparable anti-inflammatory cytokine profile of human cartilage when compared to treatment with fresh ACS and that FD-CS will provide similar protective effects to ACS in cartilage explants insulted with pro-inflammatory human recombinant interleukin-1β (IL-1β).
Methods
Study Overview
Cartilage explants were harvested from 6 consenting patients undergoing TKA and 4 mm diameter plug samples were cored out using a biopsy punch on the specimens for analysis. Autogenic ACS was created from patient serum samples. Allogenic FD-CS was created from 6 separate consenting patients at a different clinical site. Half of the cartilage explants were exposed to exogenous IL-1β to mimic the inflammatory environment synovium provides in a degenerative joint as the harvested cartilage is devoid of synovial inflammatory secretions such as IL-1β. Furthermore, cartilage samples were divided into 6 groups: (1) untreated control, (2) ACS, (3) FD-CS, (4) IL-1β (5 ng/ml) without biologic treatment, (5) IL-1β + ACS, and (6) IL-1β + FD-CS. After 12 days of incubation, samples were analyzed and compared for DNA normalized glycosaminoglycan (GAG) concentration, cytokine contents, and histological examination.
Participant Inclusion and Exclusion Criteria
Six patients scheduled to undergo TKA at Midwest Orthopedics at Rush (Chicago, IL) were recruited to participate in the study, which required specimen collection of cartilage explants and 50 ml of blood the day of surgery for autogenic ACS preparation. An additional 6 confirmed healthy patients at Colorado State University (Fort Collins, CO) were recruited only for 50 ml blood draws for the allogeneic FD-CS preparation. No further follow-up was required for any study participant. Each TKA patient met the following inclusion and exclusion criteria: age 18 to 70 years, scheduled for primary TKA (revision TKAs excluded), diagnosis of primary OA (history of inflammatory arthritis excluded), and a negative current smoking status.
Patient Consent
The study was approved by Institutional Review Board at both participating institutions at Rush University Medical Center and Colorado State University. Eligible candidates were identified regardless of race or gender from the surgical schedule of 2 fellowship-trained arthroplasty surgeons via review of electronic medical record (EMR) by trained study staff. Identified candidates were contacted by a member of the study team via phone at least 1 week prior to their TKA. A study staff member provided an explanation of the study, study expectations for candidates, and that study participation would not impact their care. Candidates who verbally then signed electronic consent forms prior to their surgery.
Patient Documentation and Anonymity
Each participating patient was assigned a unique code for anonymity and identification. The following information was extracted from the EMR: age, body mass index (BMI), date of service, diagnosis, medical comorbidities, and history of injection therapy for ipsilateral knee OA. The macroscopic description of the area of explanted articular cartilage was documented. Data were linked to the corresponding blood and cartilage specimens via the unique patient identifier.
Blood Draws for Autologous and Freeze-Dried Allogenic Conditioned Serum
Preoperatively, each of the 6 study subjects had 50 ml of blood drawn using a 14-gauge needle to minimize hemolysis during surgical preparations using aseptic processes according to standards of care. Each blood sample was placed into a commercially available interleukin-1 receptor antagonist (IL-1Ra) kit (ART-BIO, LLC., Fort Collins, CO), which contained treated medical glass beads prepared using a proprietary method embedded with agents intended to stimulate cytokine production including IL-1Ra production. The specimens were then processed according to manufacturer’s instructions. The blood was then cultured at 37 °C for 24 hours and the serum harvested following centrifugation. The serum was pooled and lyophilized for at least greater than 48 hours.
All identifying information was removed from each sample before it was transferred to the lab (CSU) for further processing and ACS preparation. At a separate clinical site, 50 ml of blood was drawn from 6 different allogeneic healthy control subjects and placed into a commercially available IL-1Ra kits (ART-BIO, LLC.) and processed according to manufacturer’s instructions as outlined previously using the same methodology. These samples were then later processed to generate FD-CS. Freeze-dried samples were reconstituted with Insulin-Transferrin-Selenium (ITS) Media Supplement. The ITS Media Supplement contains optimized concentrations of human insulin, human transferrin, and selenite without saline affecting osmolality.
Conditioned Serum Preparation
For each sample, blood was transferred to sterile IL-1Ra kits (ART-BIO, LLC.) and processed according to manufacturer’s instructions. One additional tube was prepared in the absence of the glass beads to act as controls. Tubes were incubated for 24 hours at 37 °C in a horizontal position. Following incubation, each conical tube was centrifuged for 10 minutes at 4,000 rotations per minute. Approximately 10 ml of conditioned serum was harvested from each tube, filtered using a 0.22 µm pore size syringe filter, and stored in 15 ml conical tubes. These steps were performed in a class 100 laminar flow hood using sterile technique to prevent sample contamination. The samples intended for the FD-CS group were then dehydrated and frozen to form FD-CS. All ACS and FD-CS samples were then frozen at −80 °C prior to further testing.
Cartilage Harvesting
Intraoperatively, for each TKA, 12 uniform cartilage explants were collected from articular surface following standard osteotomy cuts of the 6 different donors (2 explants per patient) undergoing TKA. As much tissue as possible was harvested only from macroscopically smooth surfaces, avoiding severe macroscopic osteoarthritic changes per surgeon judgment. Explants originated from both femoral and tibial surfaces, including medial and lateral locations based on the above parameters. Cartilage explants were placed in a sterile specimen cup filled with saline and transported to the lab on wet ice. Following transport, explants were cored out into 4 mm plugs using a punch biopsy washed in ITS media then plated in a 24-well culture dish with 500 µl of the same serum free culture media and allowed to stabilize for 48 hours at 37 °C prior to study testing. The same media stock (ITS media) was prepared and added to all culture wells ensuring the samples were matched with regards to pH and osmolality.
In Vitro Cartilage Bioassay
All of the 4 mm explants cored from cartilage specimens were cultured and analyzed in the exact same manner. For each individual TKA donor, we had 6 treatment groups as outlined in Figure 1 , and experiments were run in duplicate. For each treatment group, four 4 mm explants from each specimen were analyzed per well, and as the analysis was run in duplicate, eight 4 mm explants were analyzed per treatment group for each donor. For each well, each experiment consisted of one 4 mm explant used for histology and three 4 mm explants that were digested and utilized for GAG and DNA analysis and biochemical analysis. Importantly, the cultured media from each well was utilized in the enzyme-linked immunosorbent assay (ELISA) analysis. Therefore, biochemical analysis was performed on six 4 mm explants per donor for each of the 6 donors and the final cytokine data represent the averages from six 4 mm explants from 6 different donors. At day 2, half of the cartilage explants were exposed to 5 ng/ml of human recombinant IL-1β added to the culture media. After 48 hours of stimulation (day 4), all samples were treated with one of the 3 conditions: control media, ACS, or FD-CS. ACS and FD-CS samples were diluted in culture media at 1:1 concentration. Control media was undiluted (DMEM + F12 1:1 ratio was used with 1% miniITS supplement). An “Untreated Control” group was only exposed to control media, and had no exposure to IL-1β, ACS, or FD-CS. Media was harvested and changed every 48 hours until day 12 of incubation. At the end of the study, cartilage explants were collected, with 1 cartilage explant from each condition used for biochemical analysis whereas the other was processed for histological analysis.
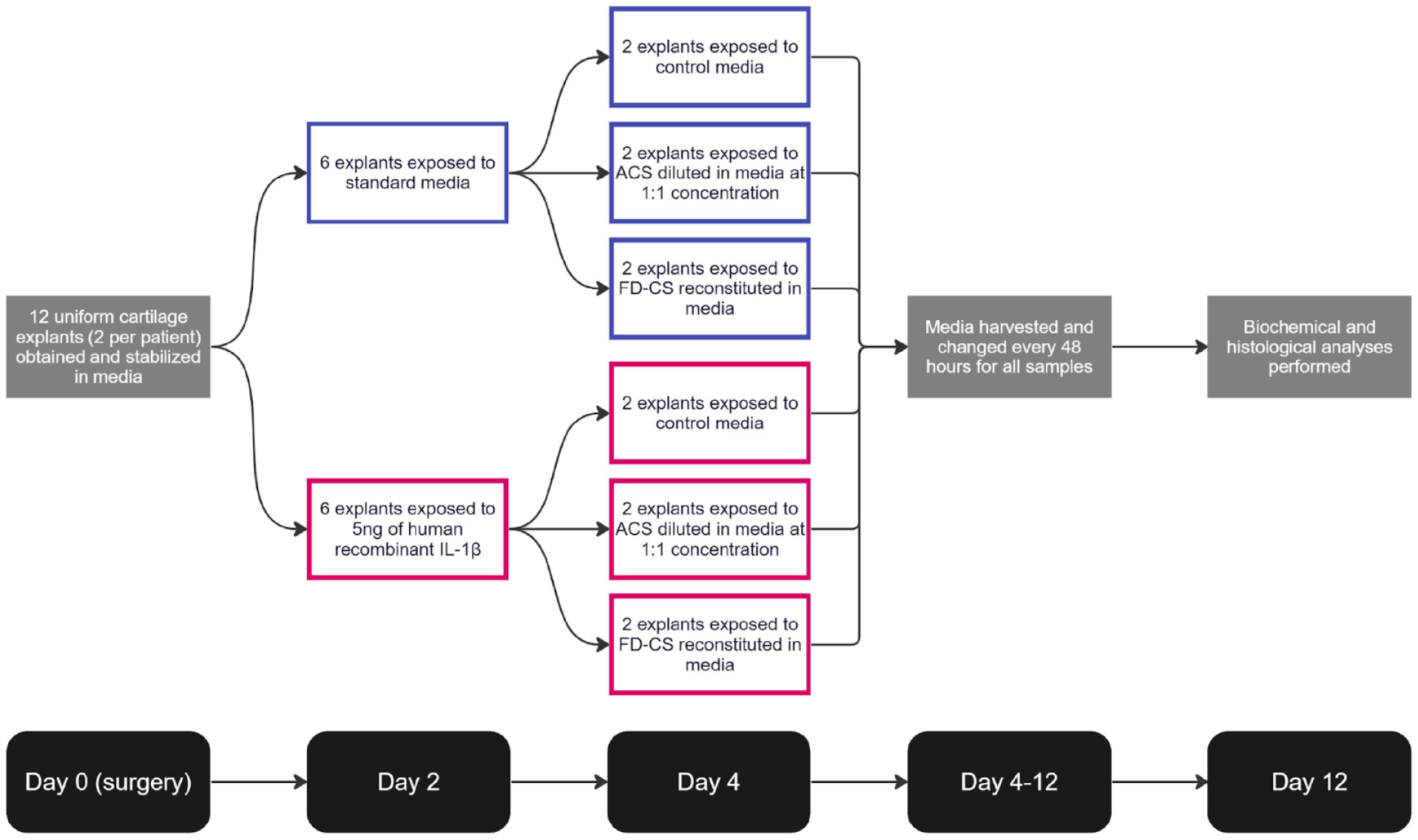
Twelve uniform cartilage explants (2 per patient) were obtained after TKA and evenly divided into treatment groups prior to biochemical and histological analysis.
Biochemical Analysis of Cartilage Explants and Media
Cartilage explants were weighed, lyophilized, and digested with papain at 60 °C. The concentration of the papain used for digestion was 20 µg/ml. Cartilage explants and media were analyzed for total GAG concentration using a modified method of the dimethyl-methylene blue (DMMB) assay. In brief, the digested samples were added to a dye/buffer solution and read against a standard curve created by purified chondroitin sulfate C from shark cartilage (Sigma, Japan). The change in color was analyzed using spectrophotometry on a plate reader (Multi-label Counter-Wallac, PerkinElmer, Waltham, MA). Similarly, cartilage DNA content in cartilage explants was determined using a fluorescent dye–based assay (Hoechst 33258) and read against a standard curve using calf thymus DNA. All samples and standards were run in duplicate. Finally, ELISA assays (RayBiotech, Peachtree Corners, GA) were used to evaluate the concentrations of basic fibroblast growth factor (bFGF), IL-1β, IL-1Ra, IL-6, IL-10, tissue inhibitor of metalloproteinase-1 (TIMP-1), and tissue necrosis factor alpha (TNF-α) in cultured media. These assays were run at RayBiotech laboratories (Norcross, GA) providing raw mean values for the preselected protein targets. Cytokine concentrations were reported for the medium of cartilage explants after their assigned treatment with the experimental agents. No cytokine concentrations were available for the medium itself without being exposed to the cartilage explants.
Histological Analysis of Cartilage Explants
Cartilage explants were fixed in formalin 10% for 48 hours and were paraffin embedded. Five micrometer thick sections were created, and tissue was placed on histology slides. One slide from each cartilage explant was stained with hematoxylin & eosin (H&E), and the other slide was stained with safranin-O fast green. A representative histological sample from the experimental FD-CS is shown in Figure 2 . A Nikon Eclipse E800 (Nikon Inc., Garden City, NY) microscope with imaging software: NIS-Elements D Version 5.02.00 for 64-bit edition was used for acquiring images at 4×, 10×, and 20× objectives. Safranin-O slides were evaluated using individual parameters from a modified Mankin scoring system based on the histological–histochemical grading system originally introduced by Mankin et al. and modified for use in several following studies.16-19 The criteria for histology scoring include subscores for cellularity and safranin-O staining with a total score from 0 (normal cartilage) to 7 (hypocellular cartilage with no safranin-O staining). Examples of modified Mankin scores based on experimental histological samples are shown in Figure 3 . The explants sectioned for histology were taken at a single depth of cartilage and lacked a superficial layer, so cellular structure and tidemark integrity were not analyzed. Scoring was performed by a single grader blinded to treatment groups (T.J.E.).
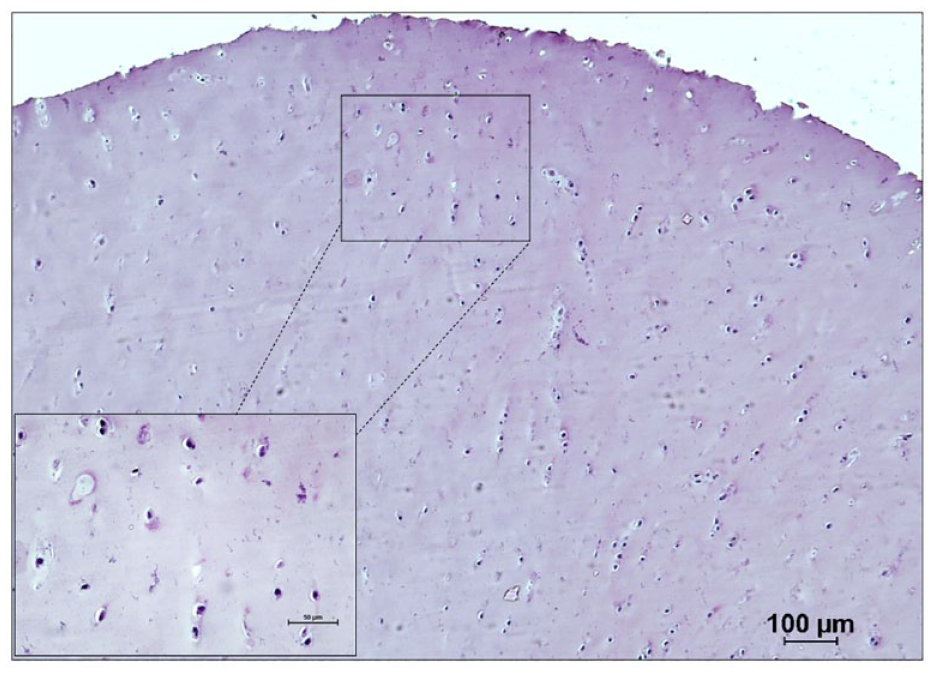
Hematoxylin & eosin (H&E) stained cartilage explant from the FD-CS group examined with microscopy at 4× magnification and enlarged area at 20× magnification.
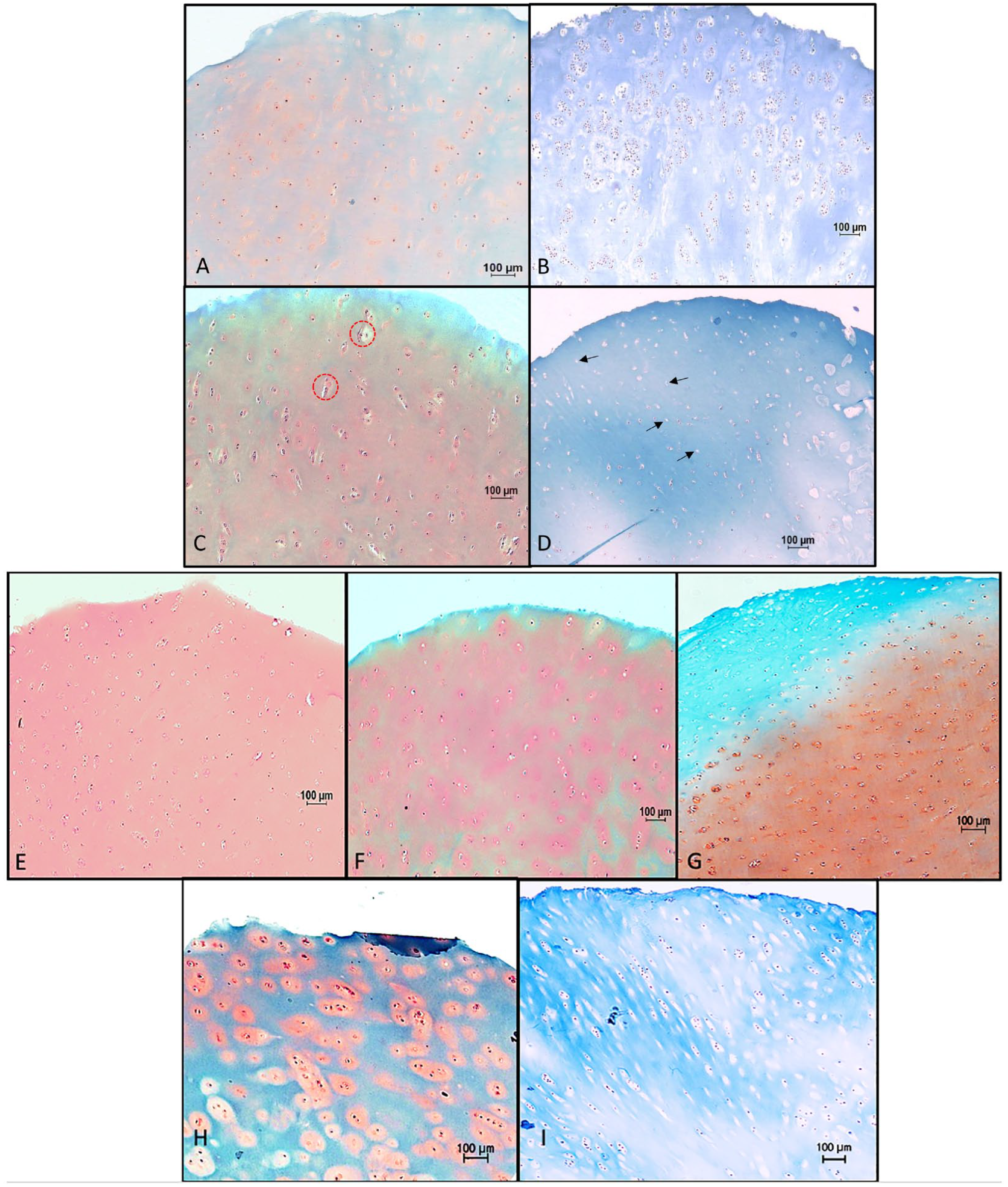
Histological assessment of the cartilage explants according to a modified Mankin scoring system assessing (with experimental group for each sample identified): Cellularity—(
Statistical Analyses
Statistical analyses were completed using SAS software (version 9.4, SAS Institute Inc., Cary, NC). All data were analyzed on day 12 of the study. The data were analyzed using a mixed model analysis of variance with presence or absence of IL-1β and biologic treatment groups as a fixed effect with the patient acting as a random effect. A protected F test was used to justify individual comparisons and control for multiple comparisons. When individual comparisons were made, a least square means estimate was used and reported along with the 95% confidence interval (CI). The highest significant order interaction was reported. Studentized residuals were used to check the assumptions of normality. Alpha level of <0.05 was considered significant.
Results
Biochemical Analysis of Cartilage Explants
DNA and wet weight normalization analysis
Independent of the presence of IL-1β, there was a significant reduction in DNA content observed in explants exposed to ACS (mean = 6.90, 95% CI = 5.63 to 8.17) versus TKA explants not receiving biologic treatment (mean = 7.92, 95% CI = 6.65 to 9.19) (P = 0.0056) (Appendix
Cytokine concentration analysis
Basic fibroblast growth factor
bFGF levels were significantly different based on both the presence of IL-1β and biologic treatment group (P = 0.0043). In the absence of IL-1β, no significant differences in FGF concentrations were demonstrated in the presence of either biologic treatment when compared with the untreated control (
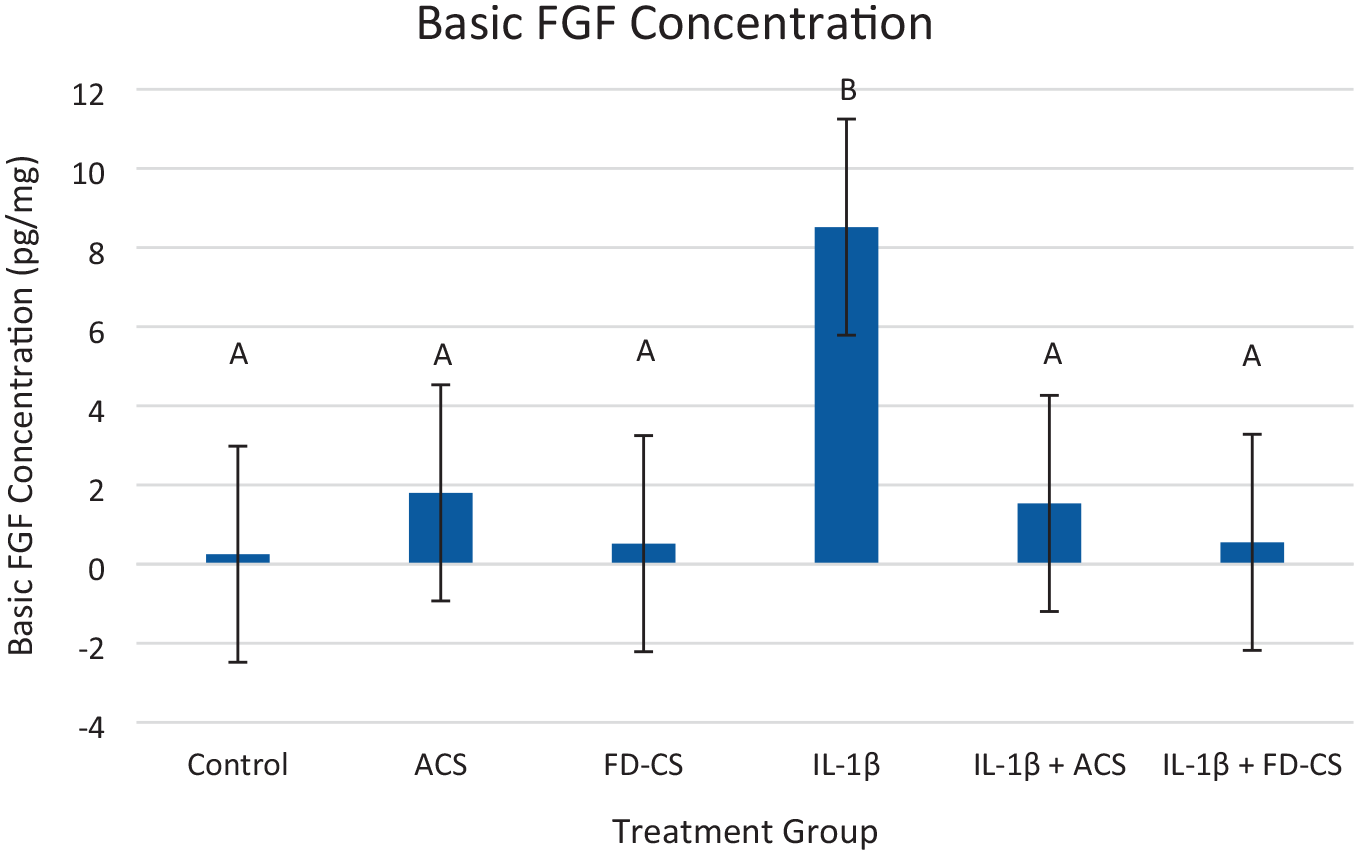
The chart above demonstrates the least square mean basic FGF concentrations (pg/mg) detected on day 12 for each of the respective groups with error bars representing the 95% confidence interval (CI). When comparing groups, the groups that have different letters indicate a statistical difference P < 0.05.
Interleukin-1 receptor antagonist
The concentrations of IL-1Ra required a natural log transformation to meet the assumptions of normality (
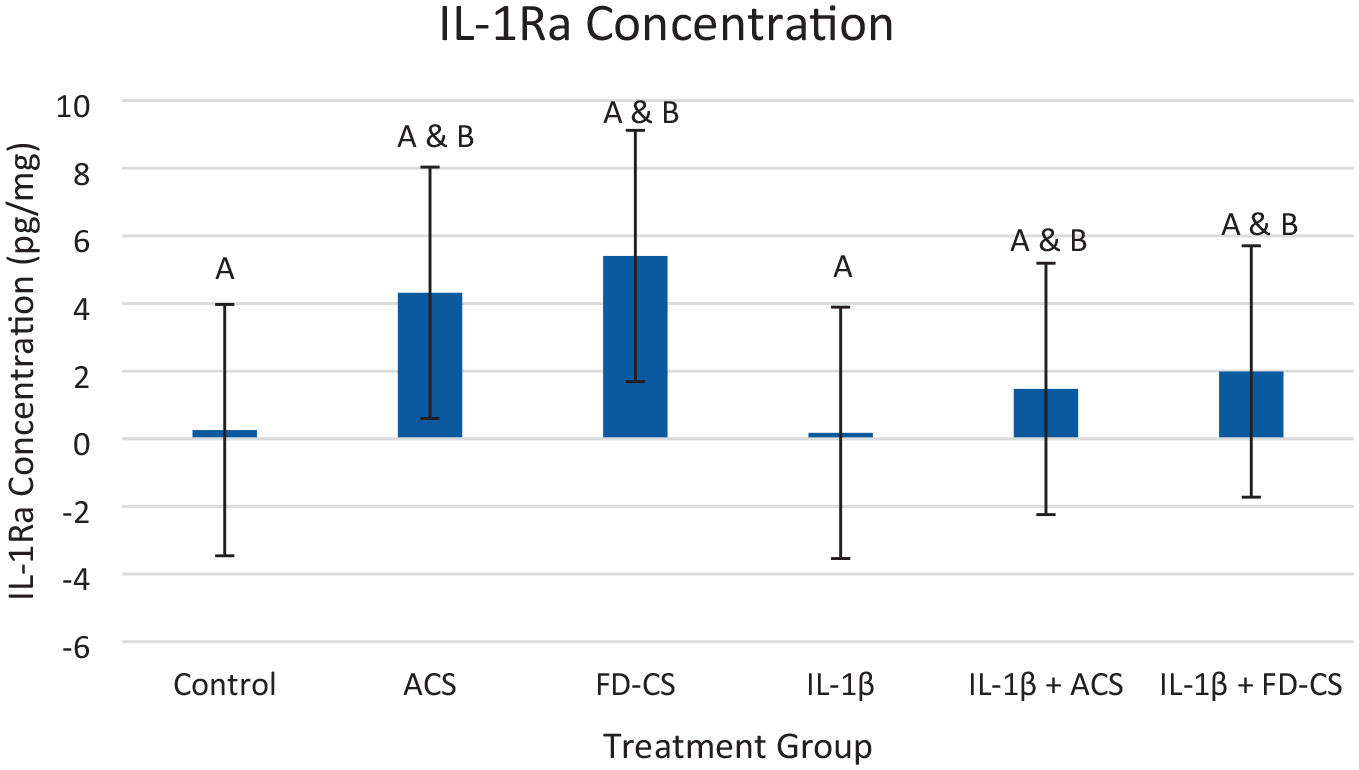
The chart above demonstrates the least square mean of IL-1Ra concentration (pg/mg) after a natural log transformation detected on day 12 for each of the respective groups with error bars representing the 95% CI. When comparing groups, groups that have different letters indicate a statistical difference P < 0.05.
Interleukin-1β
There was a significant interaction with the addition of the IL-1β insult and biologic treatment group (P = 0.0037). The presence of the IL-1β insult increased the IL-1β concentration measured in all groups (P < 0.0001), but FD-CS showed a significant decrease in the IL-1β concentration (327, CI = 287 to 367) in the presence of the IL-1β insult compared with the control (447, CI = 407 to 486, P < 0.0001) and ACS treatment (418, CI = 379 to 458, P = 0.0006) groups (
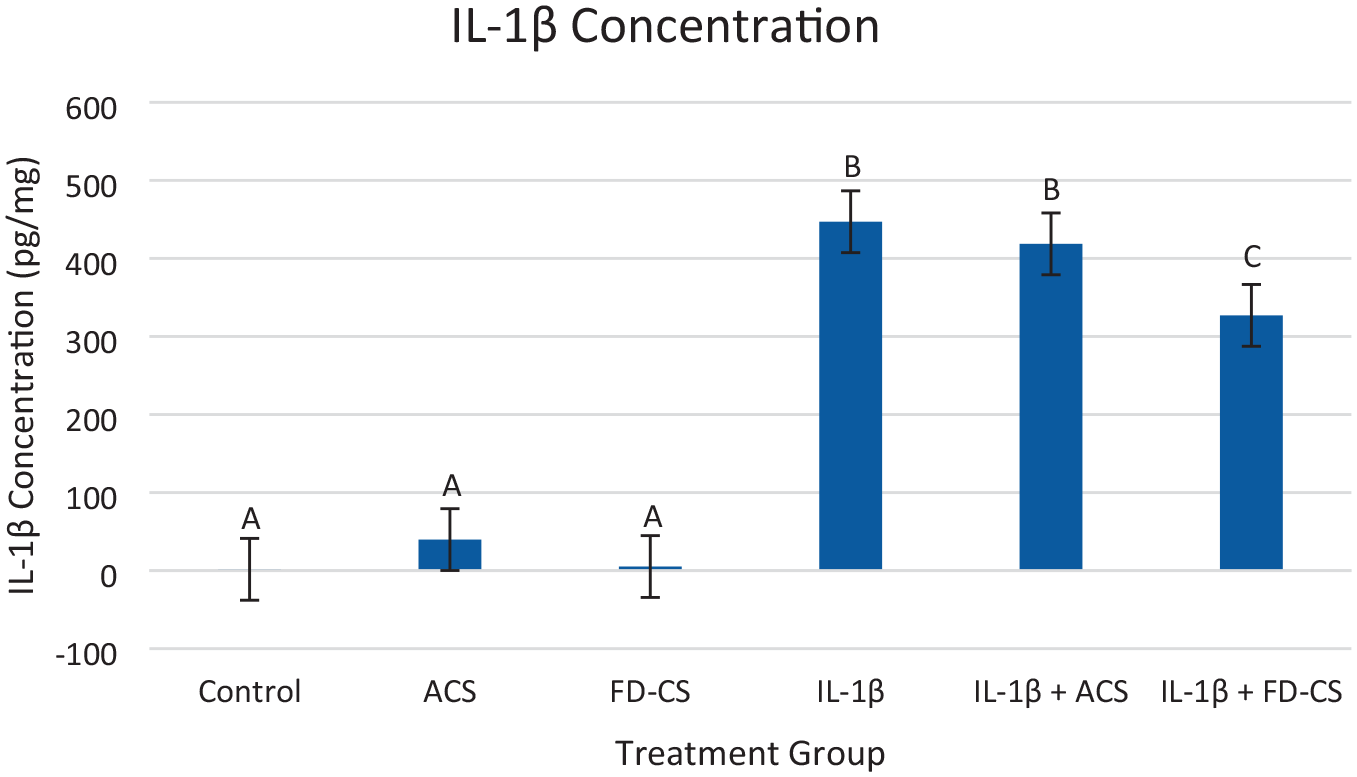
The chart above demonstrates the least square mean IL-1β concentrations (pg/mg) detected on day 12 for each of the respective groups with error bars representing the 95% CI. When comparing groups, the groups that have different letters indicate a statistical difference P < 0.05.
Interleukin-6
Exposure of the TKA explants to biologic treatment in the absence of IL-1β, IL-1β in isolation, or IL-1β concomitantly with either biologic treatment resulted in significant increases in IL-6 concentrations compared with the untreated control (P < 0.0001) (
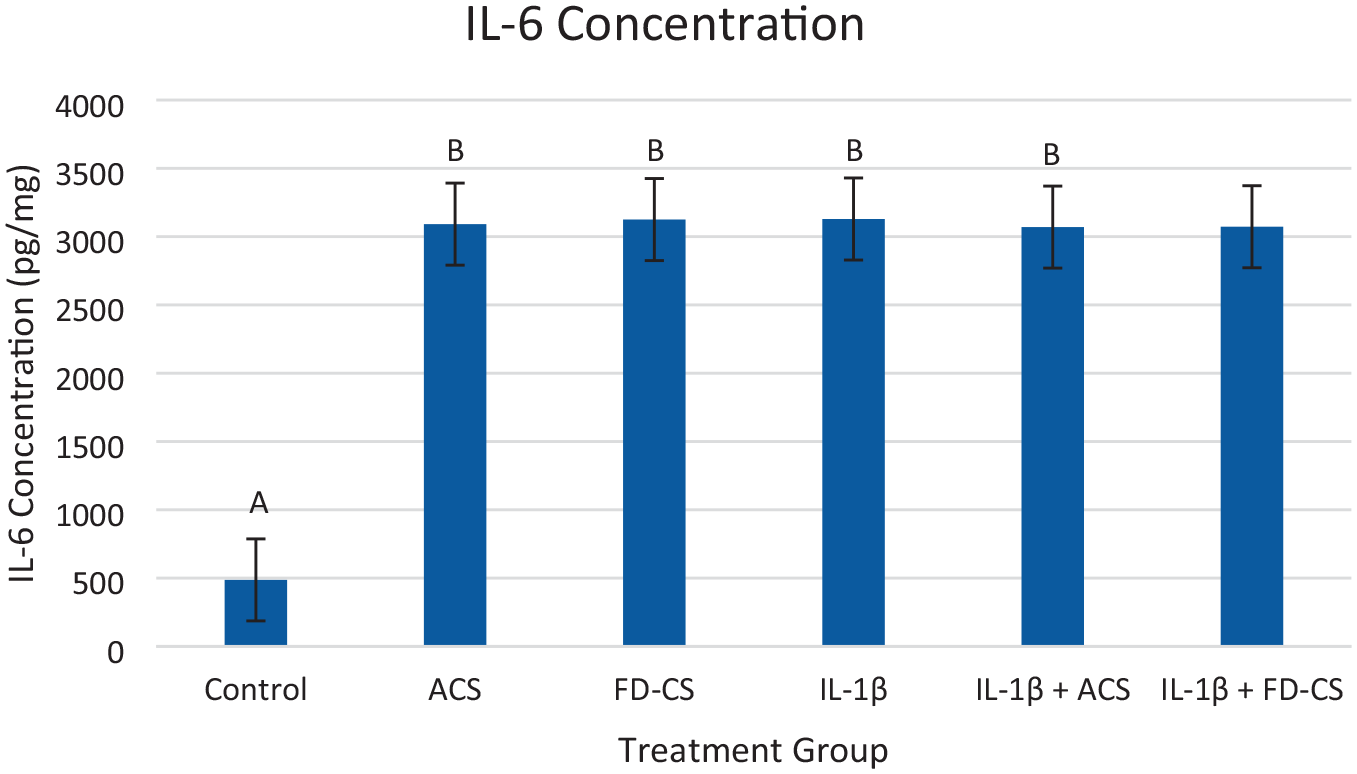
The chart above demonstrates the least square mean IL-6 concentrations (pg/mg) detected on day 12 for each of the respective groups with error bars representing the 95% CI. When comparing groups, the groups that have different letters indicate a statistical difference P < 0.05.
Interleukin-10
Independent of whether the TKA explants received biologic treatment or no treatment, IL-1β overall significantly increased IL-10 levels from a mean of 41.5 (CI = −3.28 to 86.3) to a mean of 136 (CI = 91.3 to 181) (P < 0.0001). No other significant effects were demonstrated (
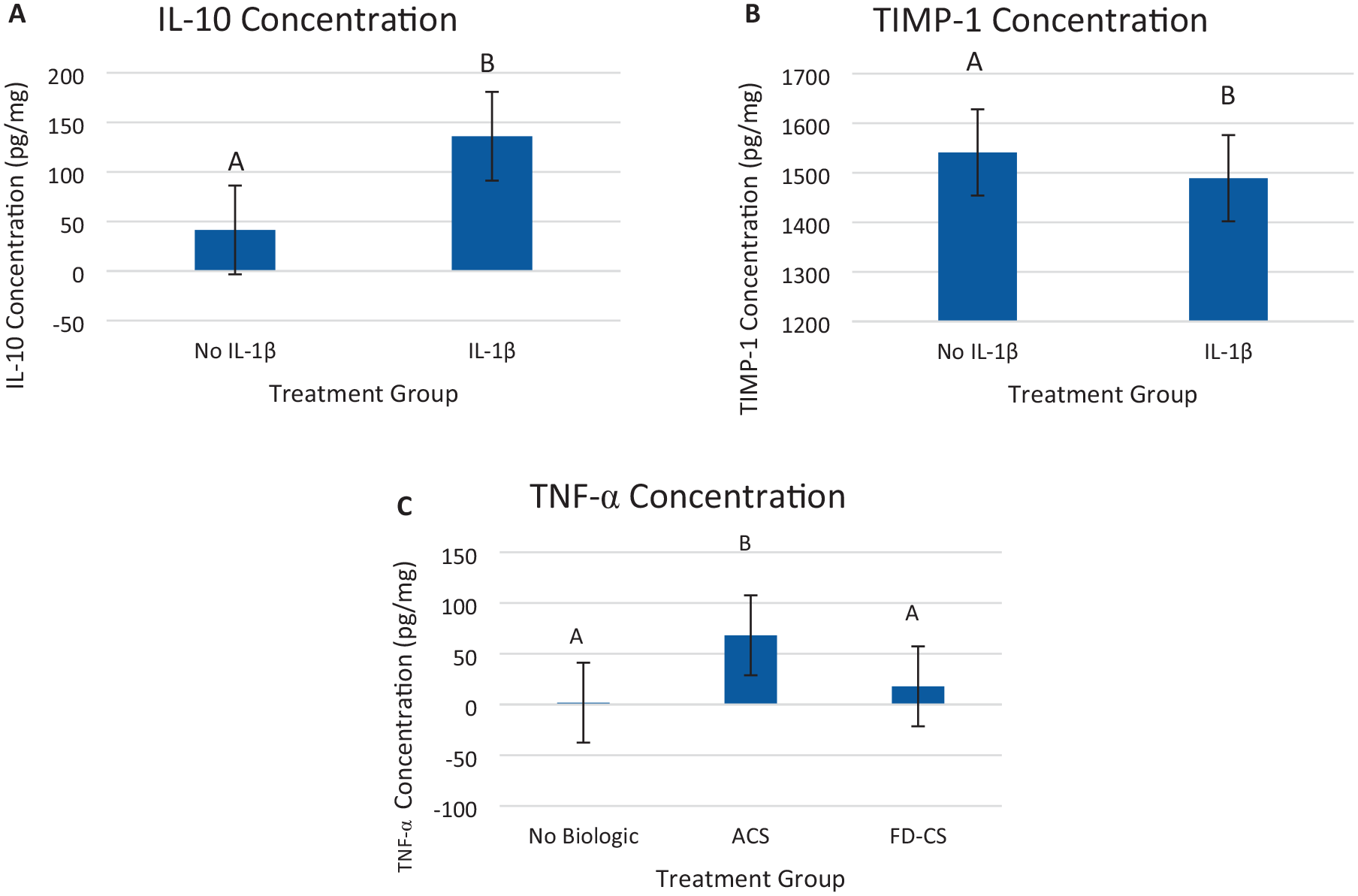
The chart above demonstrates the least square means for (
Tissue inhibitor of metalloproteinase-1
The only variable that had a significant effect on TIMP-1 levels was IL-1β. IL-1β decreased the concentration of TIMP-1 independent of treatment group from 1,541 (CI = 1,454 to 1,629) to 1,489 (CI = 1,401 to 1,576), respectively (P = 0.0297;
Tumor necrosis factor-α
Biologic treatment had a significant effect on the TNF-α concentrations (P = 0.0141) independent of the presence of IL-1β. Specifically, ACS-treated samples had significantly higher concentration of TNF-α (68.2, 28.7 to 107) compared with explants not receiving biologic treatment (1.8, −37 to 41, P = 0.0053) and FD-CS groups (17.8, −21 to 57, P = 0.0292) independent of IL-1β (
Modified Mankin Histological–Histochemical Scoring
Although the protected F test did not show significant differences, individual comparisons of the presence of IL-1β and treatments demonstrated a significant decrease in overall pathology score for ACS (mean = 3.50, 95% CI = 1.91 to 5.09, P = 0.0368) or FD-CS (mean = 3.50, 95% CI = 1.91-5.09 P = 0.0368) in the presence of IL-1β when compared with the IL-1β control alone (mean = 5.00, CI = 4.11 to 5.89) (
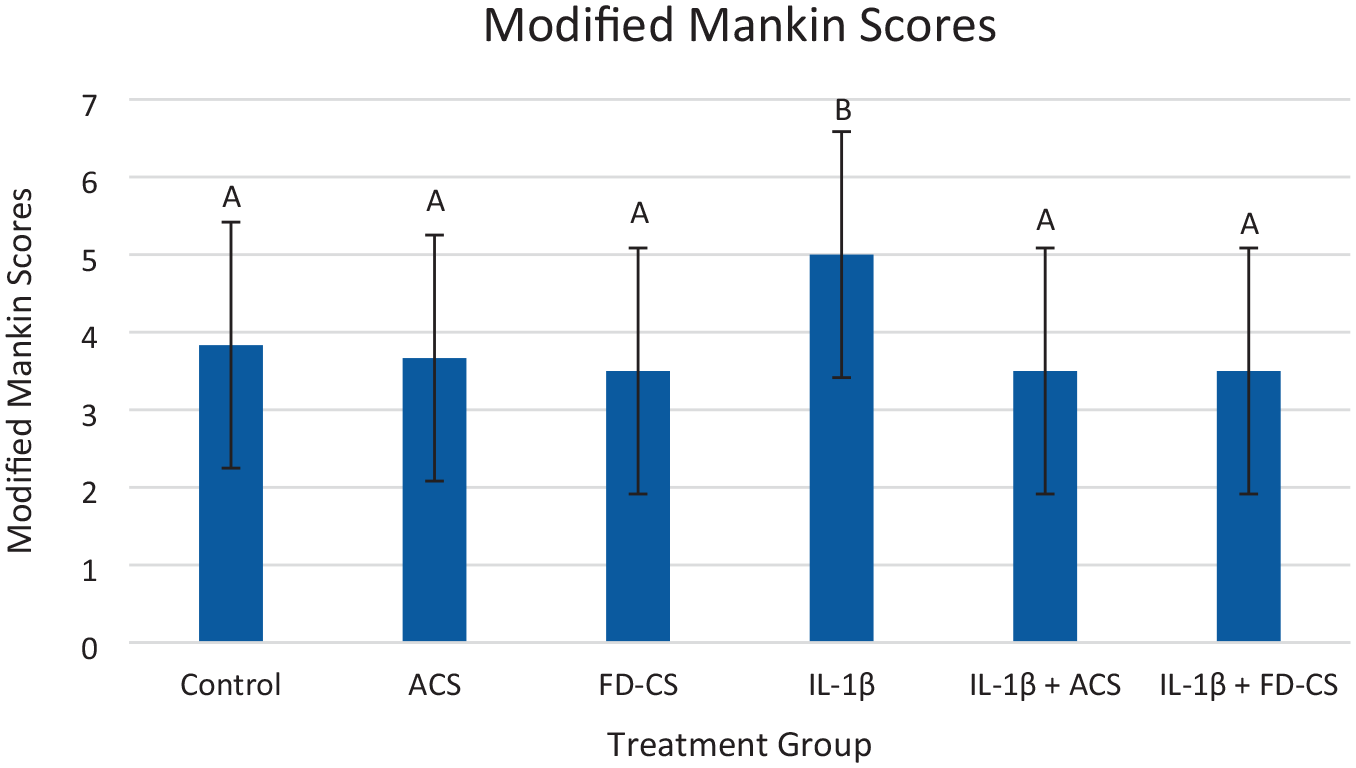
The chart above demonstrates the least square mean modified Mankin scores scored on day 12 for each of the respective treatment groups with error bars representing the 95% CI. When comparing groups, the groups that have different letters indicate a statistical difference P < 0.05.
Discussion
This study had multiple important findings. First, explanted osteoarthritic cartilage seems to respond favorably and equivalently to treatment with ACS and FD-CS after an IL-1β insult from a histological perspective. Second, the beneficial effects of the ACS and FD-CS treatments are likely secondary to both similarities and differences in their effect on injured cartilage cytokine profiles. Both ACS and FD-CS were able to mitigate the IL-1β induced increase in bFGF, which is an inflammatory cytokine released after cartilage injury that stimulates matrix metalloproteinases (MMPs) expression. 20 Furthermore, the addition of the IL-1β insult led to an expected increase of IL-1β in these groups. IL-1β is a known potent pro-inflammatory cytokine,21,22 and despite the additional IL-1β insult, FD-CS was able to decrease the levels of IL-1β by 26.8% by day 12 compared with the IL-1β control that was not treated with a biologic. FD-CS also significantly increased the levels of IL-1Ra, an endogenous antagonist to the cell surface receptors of potent pro-inflammatory cytokines IL-1β and IL-1a,21,22 in the absence of IL-1β, while ACS only led to nonsignificant increase in IL-1Ra levels. Third, the effects of ACS and FD-CS on the cartilage cytokine profiles were similar except for these mentioned effects and the increases in TNF-α another pro-inflammatory cytokine that increases cartilage degradative processes, synovial inflammation, and osteophyte production, 23 seen after treatment with ACS independent of receiving an IL-1β injury insult. However, these differences in cytokine profiles do not seem to impact the biologic activity of FD-CS when compared with ACS. This is important as the freeze-drying process may increase the availability of conditioned serum products to patients without impacting its efficacy.
Furthermore, the addition of an IL-1β insult significantly increased IL-10 and IL-6 and decreased TIMP-1. IL-10 is an immunosuppressive cytokine that was been shown to alleviate arthritis, cartilage degradation, and joint destruction in experimental models.24,25 IL-6 is an inflammatory cytokine that has been shown to degrade cartilage by increasing production of MMPs and eliciting an inflammatory cascade. 26 IL-6 concentrations in synovial fluid may be predictive of OA development as increased concentrations have been observed in OA patients.27,28 In osteoarthritic and damaged cartilage, there is an imbalance between TIMP-1 and MMPs. Specifically, in OA, there is a marked decrease in production of TIMP-1.29,30 When treatment groups were added to the explants in the setting of IL-1β insult, both ACS and FD-CS did not affect IL-6 and IL-10 concentrations. In addition, although low TIMP-1 concentrations were observed in the presence of IL-1β, both ACS and FD-CS treatments did not significantly affect TIMP-1 concentrations. Therefore, the beneficial mechanism of action for ACS or FD-CS is unlikely to involve IL-10, IL-6, or TIMP-1.
It is more likely that the beneficial biologic effects of ACS or FD-CS are related to their ability to mitigate increases in bFGF and the ability of FD-CS to impact the IL-1Ra/IL-1β ratio. bFGF plays a significant role in regulating normal cellular function in the joint for synovial cells, osteogenic cells, and importantly chondrocytes.31,32 In adults, aberrant bFGF signaling can lead to the development of articular cartilage degeneration.33,34 Thus, new research is being aimed at the modulation of bFGF signaling in the treatment of cartilage injury and OA. In our study, the mitigation of bFGF increases after an IL-1β insult is the mechanism common to the biologic activity of ACS and FD-CS. Another contributing mechanism may be an increased IL-1Ra/IL-1β ratio seen after the administration of FD-CS or ACS. IL-1Ra has previously been postulated to be responsible for beneficial effects of ACS,8,9 and in general, an IL-1Ra/IL-1β ratio of 10:1 to 100:1 has been suggested to provide effective therapy and sufficiently block IL-1 receptors.35,36 Both FD-CS and ACS increased IL-1Ra concentration and decreased in IL-1β concentration; however, these changes were only statistically significant in the FD-CS treatment groups. Therefore, this mechanism is more likely an important contributor to the biologic activity of FD-CS rather than ACS.
Conclusions
Explanted osteoarthritic cartilage responds favorably and equivalently to treatment with ACS and FD-CS from a histological perspective. Both ACS and FD-CS were able to mitigate the IL-1β-induced increases in bFGF and FD-CS lowers IL-1β concentration while increasing IL-1Ra concentration. Although the cytokine profile of the FD-CS was slightly altered when compared with ACS, it does not affect its biologic activity.
Limitations
This study is not without limitations. First, cartilage explants were collected from patients with known end-stage OA undergoing TKA. Despite best efforts to target macroscopically smooth cartilage for collection, it may be assumed that the articular surface was already interacting with an inflammatory environment. In addition, there is room for variability in the baseline cartilage damage and how each specimen responds to the IL-1β inflammatory insult and treatment with either ACS or FD-CS. Furthermore, from a histological perspective, the retrieval of cartilage samples from an osteoarthritic arthroplasty explant resulted in the sections being placed on the histology slides without orientation to the surface and deeper layers. Owing to this, a full Mankin score could not be completed including analysis of the structure (including irregularities in the surface, transitional, radial, and calcified zones) and tidemark integrity. 19 To address these differences, the authors used a modified Mankin score focusing on cellular composition and safranin-O staining. These criteria were predetermined and kept consistent throughout scoring to translate the cellular qualities to quantitative data for analysis. To best determine the full extent of the histopathological changes in osteoarthritic tissue and its response to ACS or FD-CS, future research should aim to section cartilage samples so that the slide will depict the full-depth changes of each sample.
Footnotes
Appendix
Authors’ Note
This study was performed at Midwest Orthopedics at Rush (Chicago, IL).
Acknowledgments and Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded through the Colorado State University-Translational Medicine Institute Fund; a combined partnership between Midwest Orthopedics at Rush (Chicago, IL) and Colorado State University (Fort Collins).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by our institutional review board.