
Abstract
Objective
The hip joint can be affected by extraspinal diffuse idiopathic skeletal hyperostosis (DISH). This study aimed to compare the clinical characteristics of hips with DISH to those with mixed-type femoroacetabular impingement symptoms (FAIS). In addition, patient-reported outcome (PRO) scores were reported among patients with DISH involving the hip joint who underwent arthroscopic treatment.
Methods
A retrospective analysis was performed using data from patients who underwent hip arthroscopy between 2017 and 2021. Patients who had a preoperative diagnosis of extraspinal DISH of the hip joint and postoperative Hip Outcome Score–Activities of Daily Living (HOS-ADL), Hip Outcome Score–Sports Subscale (HOS-SSS), International Hip Outcome Tool 12-component form (iHOT-12), modified Harris Hip Score (mHHS) and visual analog scale (VAS) for pain scores were enrolled in the study. The patients’ characteristics were compared with those of a control group (1:2) consisting of mixed-type patients with FAIS. The control group was matched in terms of age, sex, body mass index (BMI), and symptom duration.
Results
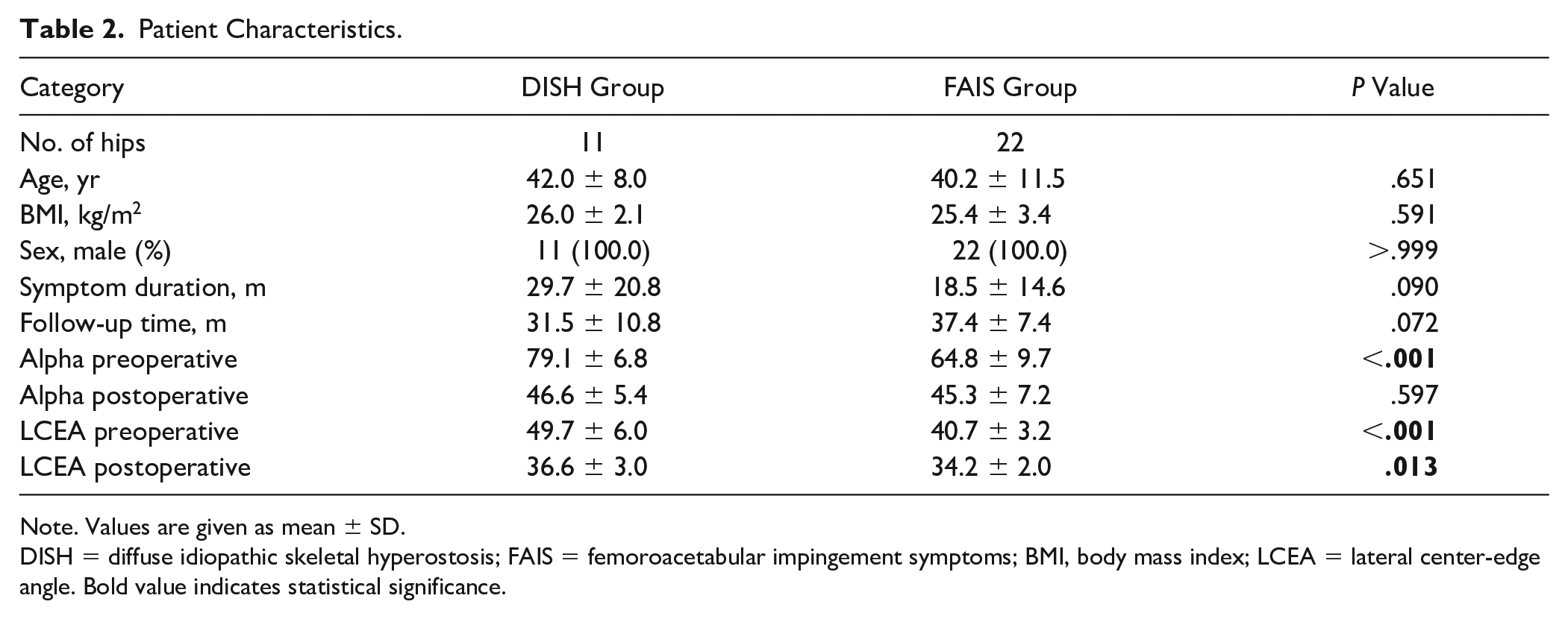
Eleven hips (0.87%) with extraspinal DISH (study group) were matched to 22 FAIS hips (control group). All the patients were male. The mean age of patients was 42.0 ± 8.0 in the study group. The study group was characterized by a larger preoperative alpha angle (79.1 ± 6.8 vs 64.8 ± 9.7, P < .001), lateral center-edge angle (LCEA) (49.7 ± 6.0 vs 40.7 ± 3.2, P < .001), and postoperative LCEA (36.6 ± 3.0 vs 34.2 ± 2.0, P = .013). In addition, a higher proportion of acetabular (81.8% vs 31.8%, P = .007) and femoral head chondral lesions (45.5% vs 9.1%, P = .016). Cartilage damage has the potential to affect the prognosis of arthroscopic treatment. Nevertheless, at the final follow-up, patients with DISH experienced a significant increase in range of motion (ROM), notable enhancements in all PROs, and favorable rates of minimal clinically important difference (MCID) for the PROs.
Conclusion
The occurrence of DISH in the hip joint is considerably infrequent, characterized by hip pain and limited ROM. Despite increased alpha angle and LCEA, and more acetabular and femoral head chondral damage noted at the time hip arthroscopy, patients with DISH observed a significant improvement in ROM, notable enhancements in all PROs, and favorable rates of MCID for the PROs.
Keywords
Introduction
Diffuse idiopathic skeletal hyperostosis (DISH) is a noninflammatory condition characterized by abnormal ossification and calcification of entheses and ligaments, most commonly in the spine; patients with DISH often exhibit a largely asymptomatic presentation, although the typical symptoms include back pain and spinal stiffness. 1 While Forestier and Rotes-Querol first described the condition in 1950—calling it “senile ankylosing hyperostosis”2,3—DISH to this day remains understudied. However, as a systemic bone-forming disease, this disorder can spread to multiple extraspinal joints. The involvement of the peripheral skeleton prompted researchers to coin the name DISH. 4
Imaging is currently the most widely used approach to diagnose DISH; plain radiographs and computed tomography (CT) scans are the most frequently used methods. 2 The most frequently employed diagnostic criteria for DISH typically include the presence of continuous anterolateral (AL) osseous formations spanning at least four thoracic vertebral segments, maintenance of intervertebral disk spaces, and the absence of degenerative changes in apophyseal joints or sacroiliac inflammation. 1 Nonetheless, in patients with DISH, a range of extraspinal symptoms and radiographic manifestations can be observed, even in the absence of radiographs of the axial skeleton.5 -7 These reports have also suggested that the radiographic presentation in the peripheral skeleton can exhibit distinctive features that are indicative of DISH, even in cases where radiographs of the axial skeleton are unavailable. Several extraspinal sites, characterized by the presence of bony outgrowths at the points where tendons, ligaments, or capsules attach to the bone, can potentially be affected. 8 These include the pelvis, hip, knee, elbow, shoulder, foot, ankle, hand, and wrist. It is noteworthy that such manifestations can occur bilaterally and exhibit symmetrical involvement. 1 Extraspinal DISH is most commonly found in the pelvis and hip: such pelvic abnormalities are characterized by bone proliferation, ligamentous ossification, and calcification. 7 Osteophytes are most commonly found in the sacroiliac joint, acetabulum, and superior pubic margins. 5 The majority of radiographic findings of extraspinal DISH involving the pelvis are asymptomatic and do not necessitate surgical intervention. 1 However, extraspinal DISH involving the anterior superior acetabulum and periarticular bone of the hip joint can cause hip pain and restricted range of motion (ROM). Abnormal ossification in the hips of individuals with DISH can lead to the development of femoroacetabular impingement symptoms (FAIS). Patients may experience sensations similar to cam and pincer lesions of FAIS. 9 Lee et al. 10 described a patient with extraspinal DISH involving the bilateral hip joint who experienced severe hip joint motion restriction. Meloxicam 15 mg used orally for 2 months reduced the pain but did not improve hip joint ROM.
To the best of our knowledge, there have been few studies on extraspinal DISH involving the hip joint, and there is no literature to report its incidence. 11 Extraspinal ossification and calcification primarily occur at the acetabular articular edge and the area of the femoral head and neck junction, which is similar to cam and pincer impingement in FAIS hips. Hip arthroscopy represents a promising approach for the treatment of these conditions by means of arthroscopic decompression. However, the existing body of evidence does not offer definitive information about potential differences in the clinical characteristics between FAIS and DISH in the hip joint, nor does it establish a clear link between arthroscopic decompression of ossification and calcification and favorable clinical outcomes. This study aimed to assess the clinical characteristics of FAIS and DISH in the hip joint, as well as patient-reported outcome (PRO) scores, in individuals with extraspinal DISH who underwent arthroscopic treatment. We hypothesized that extraspinal DISH of the hip joint would respond effectively to hip arthroscopic therapy, aiming to alleviate hip pain and improve joint mobility.
Methods
Patient Selection
This study was approved by the Ethics Committee of Peking University Third Hospital (grant no. M2019193). All patients provided informed consent to participate in this study. We used data retrospectively collected from patients who underwent hip arthroscopic surgery at our hospital between January 1, 2017, and January 1, 2021. The inclusion and exclusion criteria employed for the selection of participants in both the DISH and non-DISH groups were as follows. The patient inclusion criteria comprised of individuals with persistent groin pain; limitation in ROM (flexion, adduction, and abduction); a clinical sign of FAIS with a flexion, adduction and internal (FADIR) test, or flexion, abduction, and external rotation (FABER) test; periacetabular hyperostosis or enthesopathy without affecting the joint space or surface on plain radiography and CT of the hip joint; blood tests for erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP); and with minimum 2-year follow-up. The patient exclusion criteria comprised of individuals with a surgical history of ipsilateral hip; osteoarthritis (Tönnis grade ≥2); ankylosing spondylitis; and incomplete radiographs and medical records.
The primary distinction between DISH and FAIS in the hip joint lies in the location of abnormal ossification growth. FAIS bone spurs specifically develop at the junction of the acetabular rim and femoral head junctions. In contrast, DISH can result in abnormal ossification and calcification not only in these areas but also in the tendons, ligaments, or capsules that are attached to the bones of the hip joint ( Table 1 ). Furthermore, despite the higher incidence of cartilage injury compared to the FAIS group, DISH typically does not impact the joint space. A reliable differentiation between these two conditions can be achieved by a combination of X-ray and CT imaging, as well as intraoperative arthroscopy observations. 12
Locations of Radiographic Abnormalities of the Pelvis and Hip.
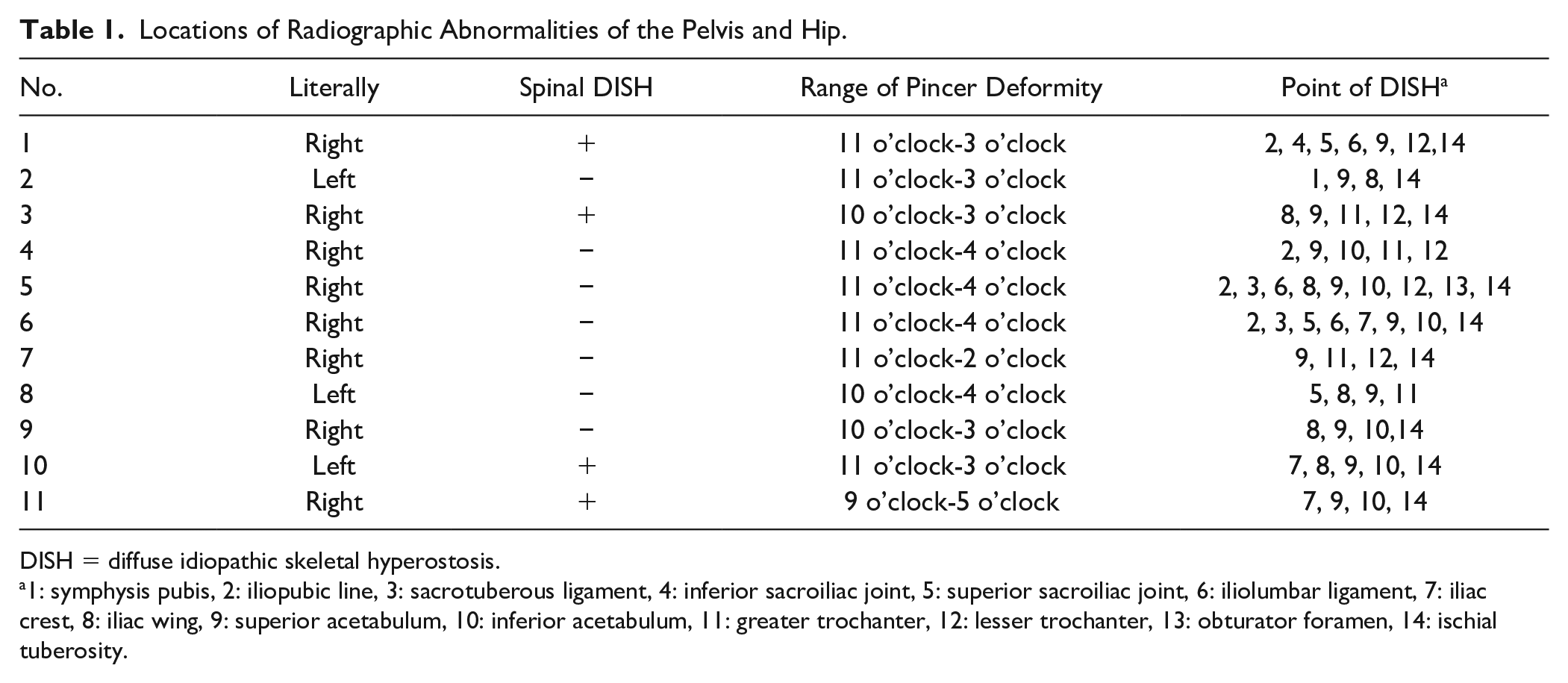
DISH = diffuse idiopathic skeletal hyperostosis.
1: symphysis pubis, 2: iliopubic line, 3: sacrotuberous ligament, 4: inferior sacroiliac joint, 5: superior sacroiliac joint, 6: iliolumbar ligament, 7: iliac crest, 8: iliac wing, 9: superior acetabulum, 10: inferior acetabulum, 11: greater trochanter, 12: lesser trochanter, 13: obturator foramen, 14: ischial tuberosity.
Imaging Evaluation
A senior author performed all radiographic analyses, evaluated preoperative patient history, and conducted a physical examination. The patients underwent anteroposterior (AP) pelvis, 45° Dunn lateral radiography, unilateral hip CT, and magnetic resonance imaging (MRI). Chondral damage and hip labral tears were determined by MRI (3.0 T). The patients underwent CT scans before surgery and 1 day later to evaluate the postoperative state of the acetabuloplasty and femoroplasty. The CT scan was performed at 120 kV, 250 mA, 0.6 mm slice thickness, a 512 × 512 acquisition matrix, and a 1 × 1 mm in-plane resolution. A radiologist recorded the findings of his radiographic measurements on picture archiving and communication system (PACS) (GE Healthcare). We did not specifically assess reliability of the radiographic parameters of interest as previous literature has consistently reported high intrarater reliability when assessing these parameters in patients with FAIS.13,14 The joint space and the lateral center-edge angle (LCEA) were calculated using AP pelvic radiographs. The alpha angle was measured using 45° Dunn lateral radiography. The diagnosis of hip DISH primarily relies on a comprehensive evaluation of symptoms, signs, and imaging. The specific symptoms and signs indicative of DISH are thoroughly described in the “patient selection” section. Radiographic examination serves as the primary diagnostic modality for DISH, revealing either profound periarticular hyperostosis on plain radiographs or ring-like enthesophytes involving the acetabular rim on CT scans. Although imaging findings in the spine can be supportive in establishing the diagnosis, they are not obligatory. Fourteen extraspinal DISH points on pelvis were recorded on the plain radiography, including the symphysis pubis, iliopubic line, sacrotuberous ligament, inferior and superior sacroiliac joints, iliolumbar ligament, iliac crest and wing, superior and inferior acetabulum, greater and lesser trochanter, obturator foramen, and ischial tuberosity, as suggested by Haller and colleagues. 7
Surgical Interventions and Rehabilitation
All hip arthroscopies were performed by a senior author. Patients were placed in the modified supine position with standard hip traction (Smith & Nephew). The advanced labrum ossifications or bony overhang of the acetabular rim do not permit direct access to the central compartment for all hips. We adopted the peripheral compartment approach. The AL portal was first established using a 30° arthroscope, and the mid-anterior portal (MAP) was fluoroscopically localized. Two processing methods were adopted. One approach is the longitudinal capsulotomy (outside-in) described by Forster-Horvath et al.
15
and Thaunat et al.,
16
which was employed in five hips. The capsulotomy was parallel and lateral to the longitudinal fibers of the iliofemoral ligament and preserved the ligament continuity. The other method was interportal capsulotomy, which involves direct puncture into the peripheral compartment via the AL portal with the hip in 30° flexion, and subsequent introduction of arthroscope. The MAP was established under arthroscopic guidance to allow for interportal capsulotomy. The proximal mid-anterior portal (PMAP) was employed in global acetabuloplasty. The central compartment was then accessed using traction. Cartilage damage was evaluated using outerbridge and acetabular labrum articular disruption (ALAD) categorization systems. All hip joints exhibited profound labral damage and underwent thorough debridement of the ossified and calcified acetabular labrum (
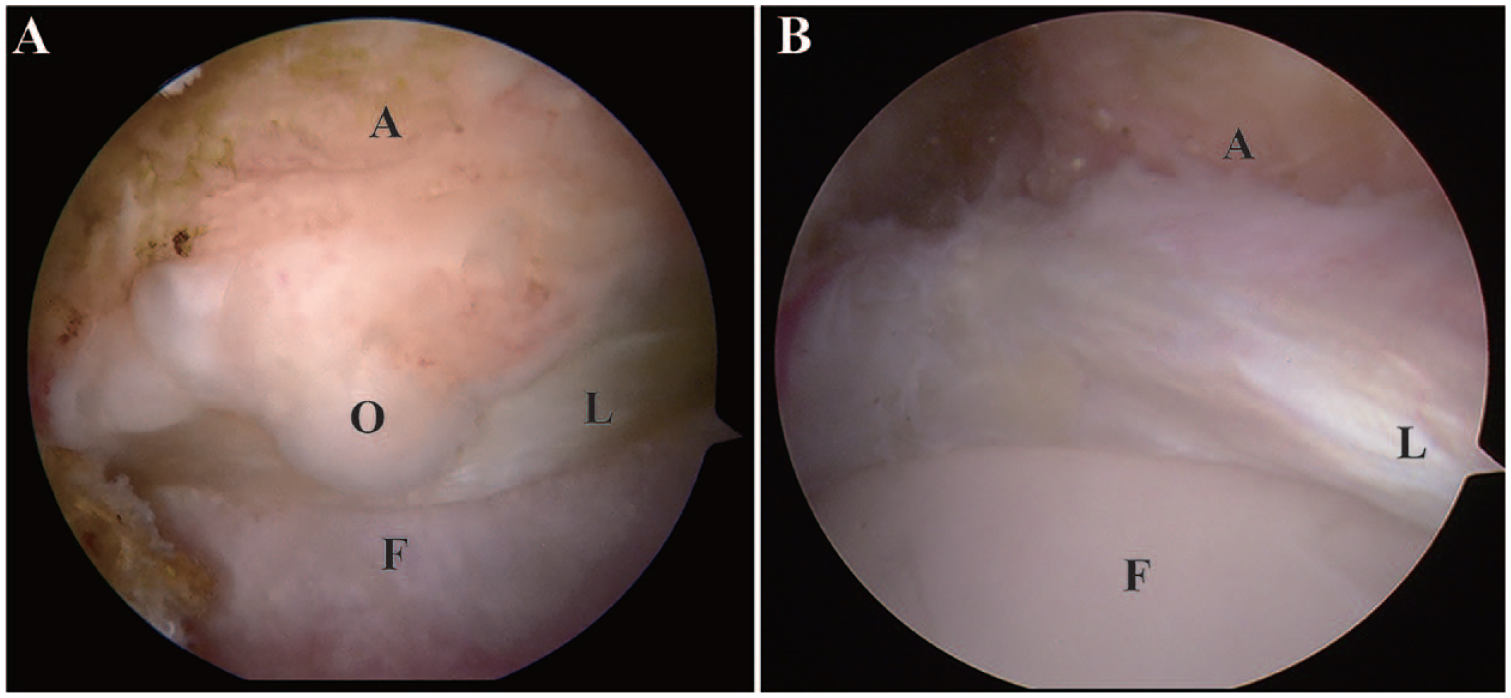
Arthroscopic views captured through the anterolateral portal depict a DISH hip (
Clinical Evaluation
The Hip Outcome Score–Activities of Daily Living (HOS-ADL), 18 Hip Outcome Score-Sports Subscale (HOS-SSS), 19 International Hip Outcome Tool 12–component form (iHOT-12), 20 and modified Harris Hip Score (mHHS) were incorporated into PROs. 21 A Visual Analog Scale (VAS) was administered to allow patients to estimate their pain levels. Furthermore, differences in preoperative and postoperative scores were calculated. The minimal clinically important difference (MCID) was determined by dividing the standard deviation of the preoperative PROs by 2. 22 The MCID thresholds for mHHS, HOS-ADL, HOS-SSS, iHOT-12, and VAS were 5.3, 7.0, 6.7, 6.3, and 1.1 respectively.
Statistical Analysis
Patients were subjected to propensity score matching in a 1: 2 ratio to mixed-type FAIS hips without DISH based on age, sex, body mass index (BMI), symptom duration before surgery, and follow-up time. The R software (Version 4.1.0; R Foundation for Statistical Computing) was used to match propensity scores. A caliper width of 0.20 was used in the algorithm to minimize the influence of confounding variables. The Shapiro–Wilk’s test was used to determine normalcy. Differences in continuous demographic characteristics between the two groups were evaluated using a two-tailed unpaired Student’s t-test. Preoperative and postoperative PROs were compared using a paired test. Categorical variables were compared using the chi-square test or Fisher’s exact test. Statistical analyses were performed with SPSS (version 26, IBM, Armonk, NY); results with P values less than .05 denoted statistical significance.
Results
Patient Characteristics and Radiographic Findings
During the study period, 1,265 patients underwent hip arthroscopic surgery, including 11 individuals (0.87%) with evidence of extraspinal DISH in the hip joint. All patients were male. The mean patient age and follow-up period were 42.0 ± 8.0 years and 31.5 ± 10.8 (range: 12-51) months for the DISH group. ESR and CRP values were normal in all cases. All patients exhibited extraspinal DISH in multiple locations around the pelvis and hip joint. Imaging revealed spinal DISH in 3 (27.3%) of the 11 patients ( Table 1 ). Eleven hips with extraspinal DISH were successfully matched to 22 patients who did not have extraspinal DISH involving the hip joint. There was no significant difference between the two groups in terms of age, sex, BMI, or symptom duration before surgery ( Table 2 ).
Patient Characteristics.
Note. Values are given as mean ± SD.
DISH = diffuse idiopathic skeletal hyperostosis; FAIS = femoroacetabular impingement symptoms; BMI, body mass index; LCEA = lateral center-edge angle. Bold value indicates statistical significance.
All hips were categorized as cam and pincer impingement in both groups. Patients with extraspinal DISH of the hip joint exhibited a larger preoperative alpha angle (79.1 ± 6.8 vs 64.8 ± 9.7, P < .001), preoperative LCEA (49.7 ± 6.0 vs 40.7 ± 3.2, P < .001), and postoperative LCEA (36.6 ± 3.0 vs 34.2 ± 2.0, P = .013). The postoperative LCEA in the DISH group showed a significant decrease compared to the preoperative values (36.6 ± 3.0 vs 49.7 ± 6.0, P < .001).
Intraoperative Findings
A summary of intraoperative findings and performed procedures are presented in
Table 3
. Patients with extraspinal DISH involving the hip joint were characterized by a higher proportion of acetabular (81.8% vs 31.8%, P = .007) and femoral head chondral lesions (45.5% vs 9.1%, P = .016). The peripheral compartment first technique was adopted in all hips in the study group due to the impossibility of directly accessing the central compartment. Longitudinal capsulotomy (outside-in) was employed in five hips. Interportal capsulotomy was employed in the left six hips, which involves direct puncture into the peripheral compartment via the AL portal with the hip in 30° flexion, and subsequent introduction of arthroscope. The MAP was established under arthroscopic guidance to allow for interportal capsulotomy. All hips affected by DISH exhibited a significant extent of Pincer deformity and large cam deformity, necessitating thorough decompression. The duration of the surgical procedure averaged 196.1 ± 44.0 (range: 133-272) minutes (
Intraoperative Findings.
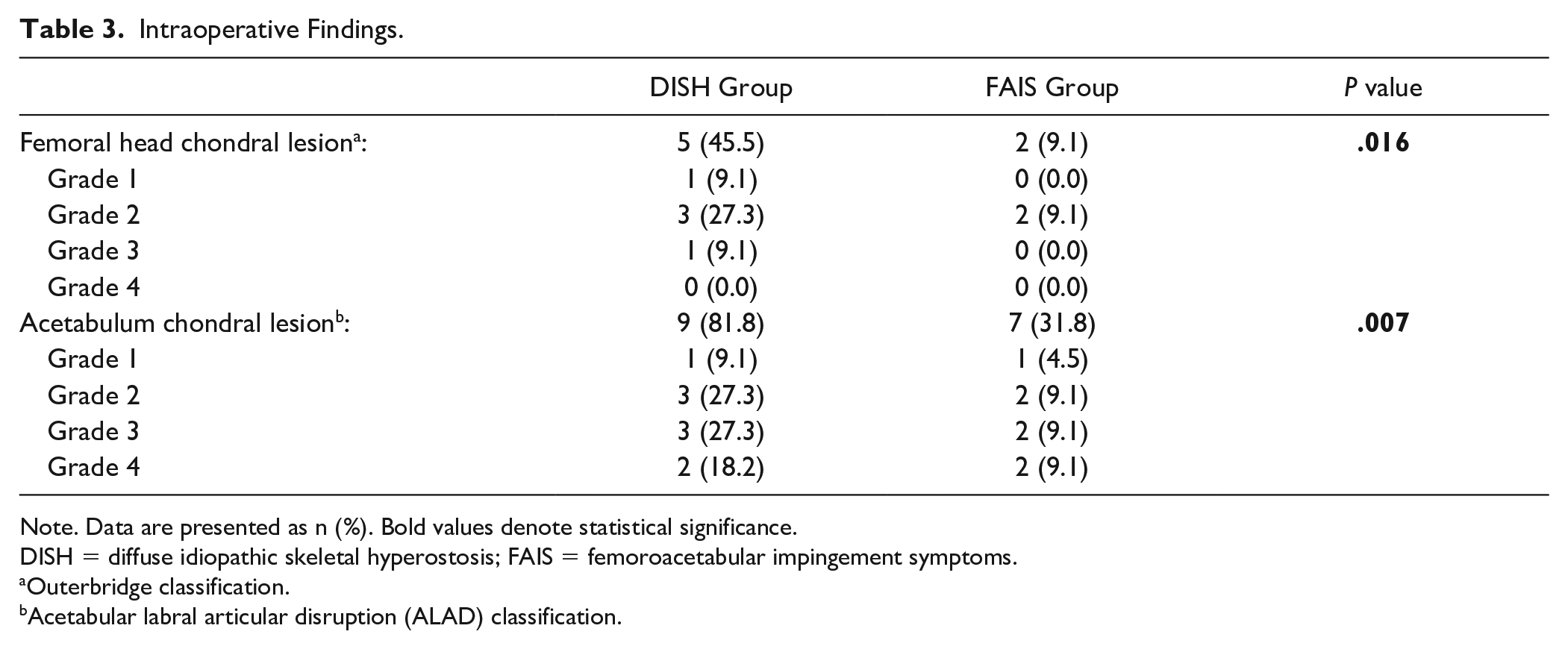
Note. Data are presented as n (%). Bold values denote statistical significance.
DISH = diffuse idiopathic skeletal hyperostosis; FAIS = femoroacetabular impingement symptoms.
Outerbridge classification.
Acetabular labral articular disruption (ALAD) classification.
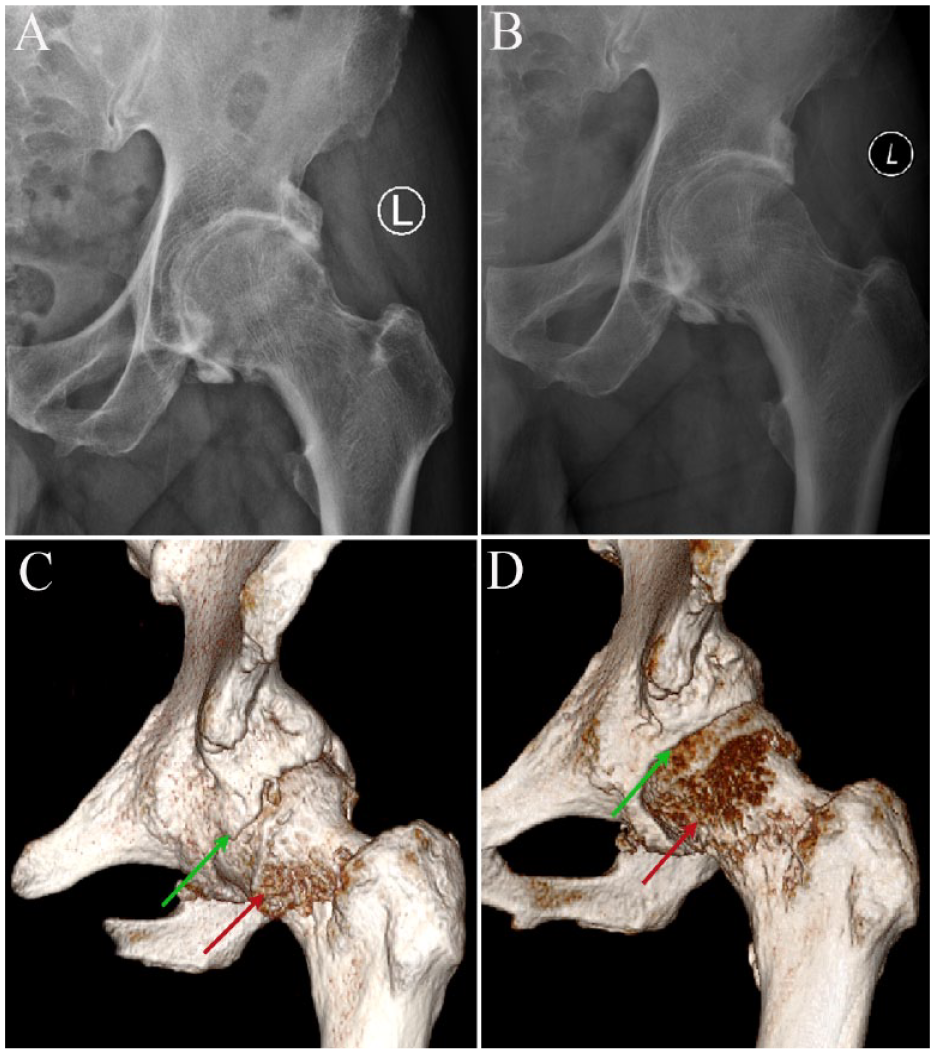
A 50-year-old man presented with pain and limited motion in the left hip for 2 years. (
Clinical Outcomes
When compared to preoperative levels, patients with DISH demonstrated significant improvements in PROs at the final follow-up. The VAS score decreased from 6.3 (5.4-7.1) to 2.3 (1.7-2.9), the HOS-ADL score increased from 66.7 (63.0-70.5) to 83.4 (78.6-88.8), the HOS-SSS score increased from 41.7 (38.2-45.1) to 70.8 (60.9-80.8), the iHOT-12 score increased from 41.5 (33.8-49.2) to 76.57 (74.40-78.75), and the mHHS score increased from 60.6 (55.4-65.9) to 81.5 (76.5-86.5) (P < .001 for all) (
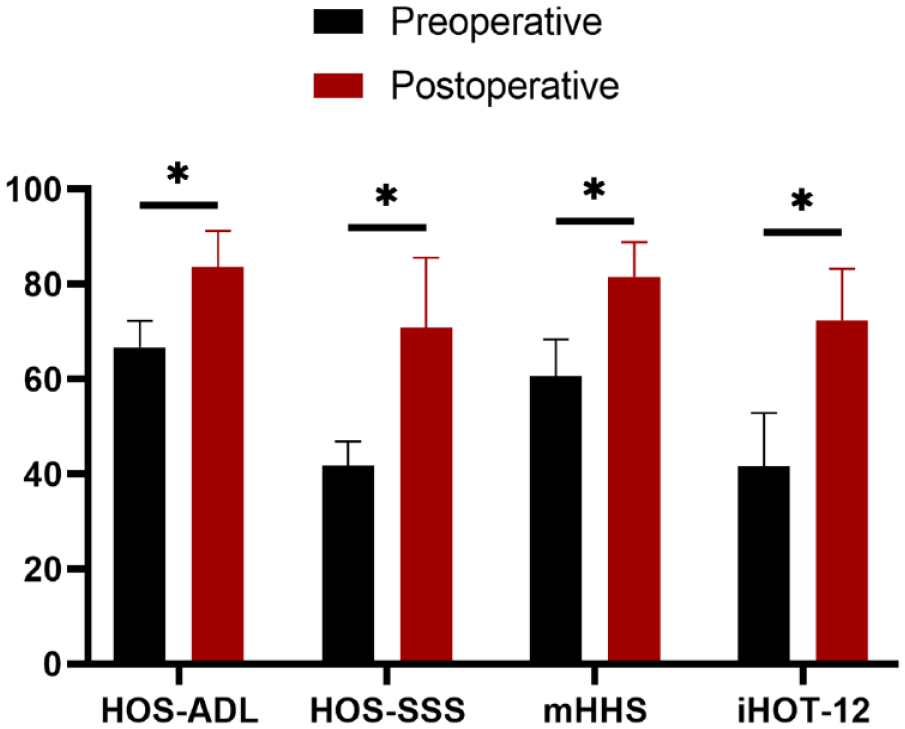
Box plot showing results of patient-reported outcome scores for the study group. HOS-ADL = Hip Outcome Scored–Activities of Daily Living; HOS-SSS = Hip Outcome Score—Sport-Specific Subscale; mHHS = modified Harris Hip Score; IHOT-12 = International Hip Outcome Tool 12 component form.
Clinical Presentation of Patients With DISH Involving the Hip.
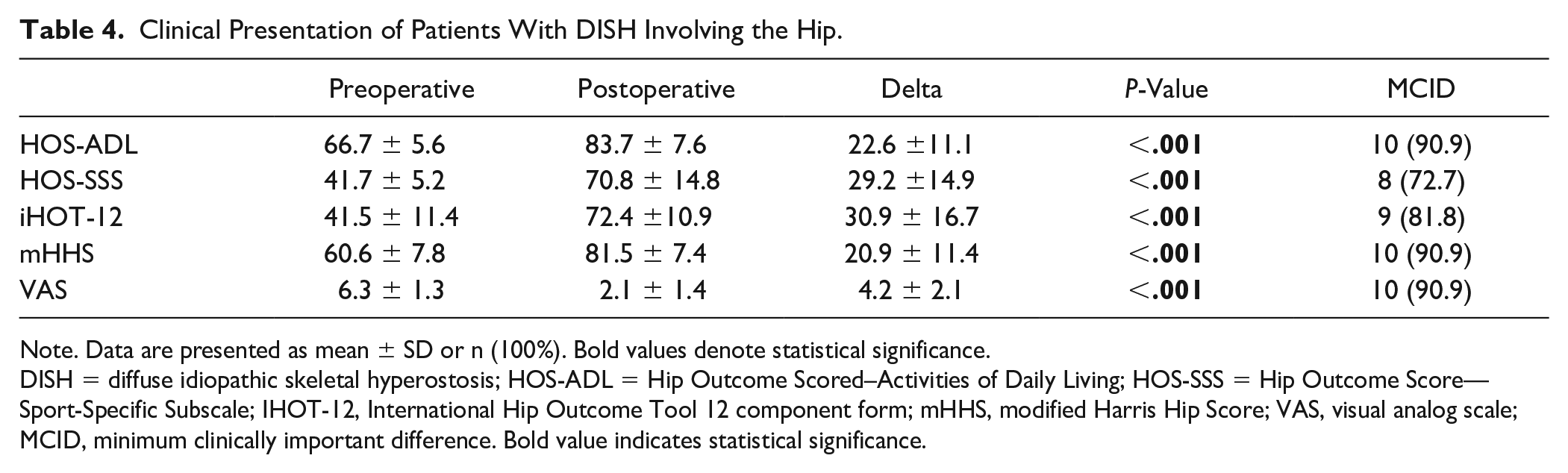
Note. Data are presented as mean ± SD or n (100%). Bold values denote statistical significance.
DISH = diffuse idiopathic skeletal hyperostosis; HOS-ADL = Hip Outcome Scored–Activities of Daily Living; HOS-SSS = Hip Outcome Score—Sport-Specific Subscale; IHOT-12, International Hip Outcome Tool 12 component form; mHHS, modified Harris Hip Score; VAS, visual analog scale; MCID, minimum clinically important difference. Bold value indicates statistical significance.
The ROM in the hip joints of the study group patients improved significantly at the final follow-up. Hip flexion and adduction improved significantly from 94.3° ± 6.0° to 118.6° ± 5.0° (P = .041) and 8.6° ± 1.6° to 15.5° ± 1.4°(P = .032), respectively; abduction also improved nonsignificantly, 27.4° ± 1.7° to 35.5° ± 1.0° (P = .605). In terms of complications and secondary surgeries, one patient in the DISH group experienced transient lower extremity nerve palsy, which resolved spontaneously within 2 weeks without any additional interventions. There were no other complications, and no patient required revision surgery or conversion to total hip arthroplasty (THA).
Discussion
The main findings of this study indicate that the prevalence of DISH involving the hip joint is notably rare in comparison to hip joints with FAIS. In addition, patients with extraspinal DISH affecting the hip joint exhibited higher alpha angle and LCEA, restricted ROM, and greater chondral damage in the acetabulum and femoral head. Following hip arthroscopic surgery, patients experienced a significant increase in ROM, notable enhancements in all PROs, and favorable rates of MCID for the PROs.
The findings of this study suggest that patients receiving hip arthroscopy for extraspinal DISH involving the hip joint showed favorable outcomes after 31.5 months of follow-up. These data concur with previous findings. Hwang et al. 11 reported the clinical outcomes of arthroscopic treatment in 12 patients with extraspinal DISH involving the hip joint over 2 years. The findings revealed that postoperative PROs, including VAS, mHHS, and HOS-ADL, improved significantly when compared with the baseline. Moreover, patients exhibited improved hip flexion from 97.7° to 117.1° and improved internal rotation from 7.9° to 18.2°. Yukizawa and colleagues 12 also reported satisfactory clinical outcomes of hip arthroscopy in 14 hips with extraspinal DISH (9 patients). Despite minimal advances in ROM, the Nonarthritic Hip Score (NAHS) increased from 47 to 56, the iHOT-12 score improved significantly from 43 to 71, and the VAS satisfaction score improved significantly from 21 to 72. The mHHS and VAS pain scores improved, although not significantly (65 to 92 and 45 to 78, respectively).
In the current investigation, the peripheral compartment first approach was employed in all hips, with the surgical approach. In the investigation of Hwang et al., 11 the central compartment could be accessed first in all cases due to adequate joint space via traction. Yukizawa et al. 12 also used a transverse, capsulotomy first approach in all hips owing to the difficulty in applying appropriate traction caused by excessive ossification at the acetabular rim. Given that DISH predominantly affects the acetabular edges in the hip joint, achieving adequate traction distance (8-10 mm) poses a significant challenge. In order to mitigate potential damage to delicate structures such as cartilage, it is recommended to adopt a peripheral compartment-first approach.
All patients had ossified or degenerative labrum with circumferential involvement. In this study, the labral was treated with debridement in 11 hips. The joint space was extremely small in the debridement patients to perform labral reconstruction following decompression of the global pincer lesion. Although Hwang et al. 11 did not specify labrum treatment, it remains the most effective procedure. Yukizawa and colleagues 12 repaired labral damage by selective debridement in four hips and reconstruction using the iliotibial band in nine hips. However, in this study, patients with labral debridement showed satisfactory short-term clinical outcomes, comparable to the control patients who underwent labral repair. An intact labrum is vital for hip joint functionality in cartilage consolidation and joint stability through its suction seal effect. 23 Nonetheless, longer PROs assessment and imaging follow-up is warranted to verify these findings. Furthermore, it is whether calcification will reoccur on the reconstructed labrum.
The prevalence of articular cartilage damage in the acetabulum and femoral head was significantly elevated in DISH involving the hip joint. Yukizawa and colleagues 12 discovered defective weight-bearing femoral head cartilage in five hips (38.5%) with DISH. They found an International Cartilage Repair Society (ICRS) score of 1 in three joints and an ICRS score of 2 in two joints. The current investigation revealed that DISH hips were characterized by a significantly higher proportion of acetabular (81.8% vs 31.8% P = .007) and femoral head cartilage lesions (45.5% vs 9.1%, P = .016). In contrast to patients with osteoarthritis, individuals with DISH predominantly exhibit cartilage damage at the edge of the acetabulum, while the overall cartilage integrity in weight-bearing areas remains relatively unaffected. In addition, patients with DISH were relatively younger. The relatively young age of patients with hip DISH may be attributed to the fact that in spinal DISH, a significant majority of patients remain asymptomatic or experience symptoms at a later stage. However, the hip joint exhibits a greater degree of mobility, which can result in an earlier onset of symptoms subsequent to the development of osteophytes at the acetabular edge. These symptoms become more apparent during physical activity. Consequently, patients are more inclined to promptly seek medical attention, leading to earlier diagnosis and treatment. All these characteristics could have contributed to the positive clinical outcomes of arthroscopy in patients with extraspinal DISH of the hip joint. THA may provide pain relief and improved ROM in DISH patients. These patients, however, may be at a higher risk of heterotopic ossification postoperatively.1,24 The current investigation confirmed that hip arthroscopic preservation surgery hip is of great promise for individuals with extraspinal DISH of the hip joint.
While our study has several strengths, including providing imaging characteristics and PROs among patients with DISH and confirming of hip arthroscopic treatment is an efficient and reliable approach for the treatment. We should acknowledge that there are some drawbacks to this study. First, a retrospective study has an inherent bias, specifically, selection bias has the potential to yield distorted results and hinder the generalizability of the findings. Second, although cases of extraspinal DISH involving the hip joint are rare, the number of patients in this study was small. Third, because this is a short-term follow-up study, revision and conversion to THA cases may increase with extended follow-up.
Conclusion
The occurrence of DISH in the hip joint is considerably infrequent when compared to hip joints affected by FAIS. Furthermore, individuals with extraspinal DISH that affects the hip joint demonstrate elevated alpha angle and LCEA, limited range ROM, and more extensive chondral damage in the acetabulum and femoral head. Subsequent to undergoing hip arthroscopic surgery, patients observe a significant improvement in ROM, notable enhancements in all PROs, and favorable rates of MCID for the PROs.
Footnotes
Author Contributions
Fan Yang: performed the formal analysis, all data and discussed them, wrote the manuscript. Hongjie Huang: figure preparation, Yan Xu: revised the manuscript. Yuanyuan Shi: revised the manuscript. Jianquan Wang: conceived and supervised the project. Xiaodong Ju: conceived and supervised the project.
Acknowledgments and Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the funding from the Innovation & Transfer Fund of Peking University Third Hospital (BYSYZHKC2021110), Clinical Cohort Project Program of Peking University Third Hospital (BYSYDL2021014), Beijing Natural Science Foundation (7242167, L212052).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study and all experimental protocols were approved by the Ethics Committee of Peking University Third Hospital (IRB: M2019193).