
Abstract
Objective
To assess the current treatment of osteochondral lesions of the ankle (OCLA) by German-speaking foot and ankle surgeons, focusing on the management of postoperative care and rehabilitation.
Design
A questionnaire was created by a panel of 4 experienced foot and ankle surgeons on behalf of the “Clinical Tissue Regeneration” (CTR) working group of the German Society of Orthopaedics and Trauma Surgery (DGOU), and distributed electronically to members of the CTR, participants of the German Cartilage Registry (Knorpelregister DGOU©), and members of 6 German-speaking orthopedics or sports medicine societies. Results were classified depending on the consensus within the answers (agreement ≥75% “strong tendency,” 50%-74% “tendency,” 25%-49% “weak tendency,” <25% “no tendency”).
Results
A total of 60 participants returned the questionnaire. The main results are as follows: regarding the frequency of surgical procedures for OCLA, refixation of the fragment, retrograde drilling, and bone marrow stimulation with or without using a matrix were performed by at least 75% of the surgeons and was considered a strong tendency. There was a strong tendency to stabilize the ankle (76.7%) and perform corrective osteotomies (51.7%). In total, 75.5% and 75% of the surgeons performed bone marrow stimulation with and without using a matrix, respectively. Corrective osteotomy and ankle stabilization were performed in 64.5% and 65.2% cases, respectively. Most participants included published recommendations on postoperative rehabilitation and the return to sports activities in their postoperative management. The main surgical procedures were considered the most critical factor in influencing the postoperative management by 81% of the participants (strong tendency). Adjunct surgical procedures such as corrective osteotomy and stabilization of the ankle were considered important by 67.8% of the respondents (tendency).
Conclusions
The management of OCLA varies among German-speaking foot and ankle surgeons. Therefore, guidelines remain essential to standardize the management of OCLA, to achieve improved and stable results. This survey will assist clinicians and patients with rehabilitation to return to sports after treating the ankle’s cartilage injury.
Introduction
Osteochondral lesions of the ankle (OCLA) are mainly posttraumatic injuries. 1
According to a recent study, the majority of OCLA are located on the talus, that is, osteochondral lesions of the talus (OLT), whereas osteochondral lesions of the tibial plateau (OLTP) are reported to occur in about 6% of OCLAs. 2
The main treatment goal is revascularizing the bony lesion and restoring the osteochondral defect. 3 Only symptomatic lesions with persistent symptoms require surgical treatment. There are 5 main surgical strategies available, that is, (1) reduction and fixation of osteochondral fragments, (2) bone marrow stimulation techniques, (3) articular cartilage replacement techniques, (4) regenerative cell therapy techniques, and (5) metal implants. 3 Adjunct treatment strategies include corrective osteotomies in patients with axial malalignment.3,4 Moreover, OCLA can be associated with an acute ligament injury and chronic ankle instability.5-10 In such cases, the treatment strategy should include stabilization procedures for the ankle. 11 A treatment algorithm for OCLA has recently been proposed by the “Clinical Tissue Regeneration” (CTR) working group of the German Society of Orthopaedics and Traumatology (DGOU). 12
The CTR working group of the DGOU published some observational studies based on data from the German Cartilage Registry (www.knorpelregister-dgou.de).11,13-16 As per one study, the surgical technique, postoperative care, and specific rehabilitation protocol might influence the outcome. The primary focus of rehabilitation after treating an OCLA should be returning to the pre-injury activity level. Van Eekeren et al.17,18 have proposed a particular algorithm for a staged return to sports activity. However, published literature on ankle cartilage repair is based on low levels of evidence, forcing surgeons to regularly render treatment decisions based on clinical experience and expert opinion.19,20
This survey aimed to assess the current treatment of OCLA by German-speaking foot and ankle surgeons, focusing on the management of postoperative care and rehabilitation.
Materials and Methods
A questionnaire was created in May and June 2019 based on expert discussion by 4 experienced foot and ankle surgeons (A.M., C.B., C.P., M.W.) to assess the rehabilitation management of surgically treated OCLA (Supplement 1). All 4 surgeons are certified members of the German Orthopaedic Foot and Ankle Society (Deutsche Assoziation für Fuß und Sprunggelenk, DAF) and/or the German Society for Foot and Ankle Surgery (Gesellschaft für Fuß- und Sprunggelenkchirurgie, GFFC). Of the 36 questions, questions 1 to 7 referred to the surgeon’s experience, 8 to 12 to the lesion’s characteristics, indication for surgery, and type of approach. Questions 13 to 25 referred to the postoperative care and rehabilitation protocol and recommendations for returning to sports activities. Questions 26 to 36 covered follow-up issues and adjunct treatments.
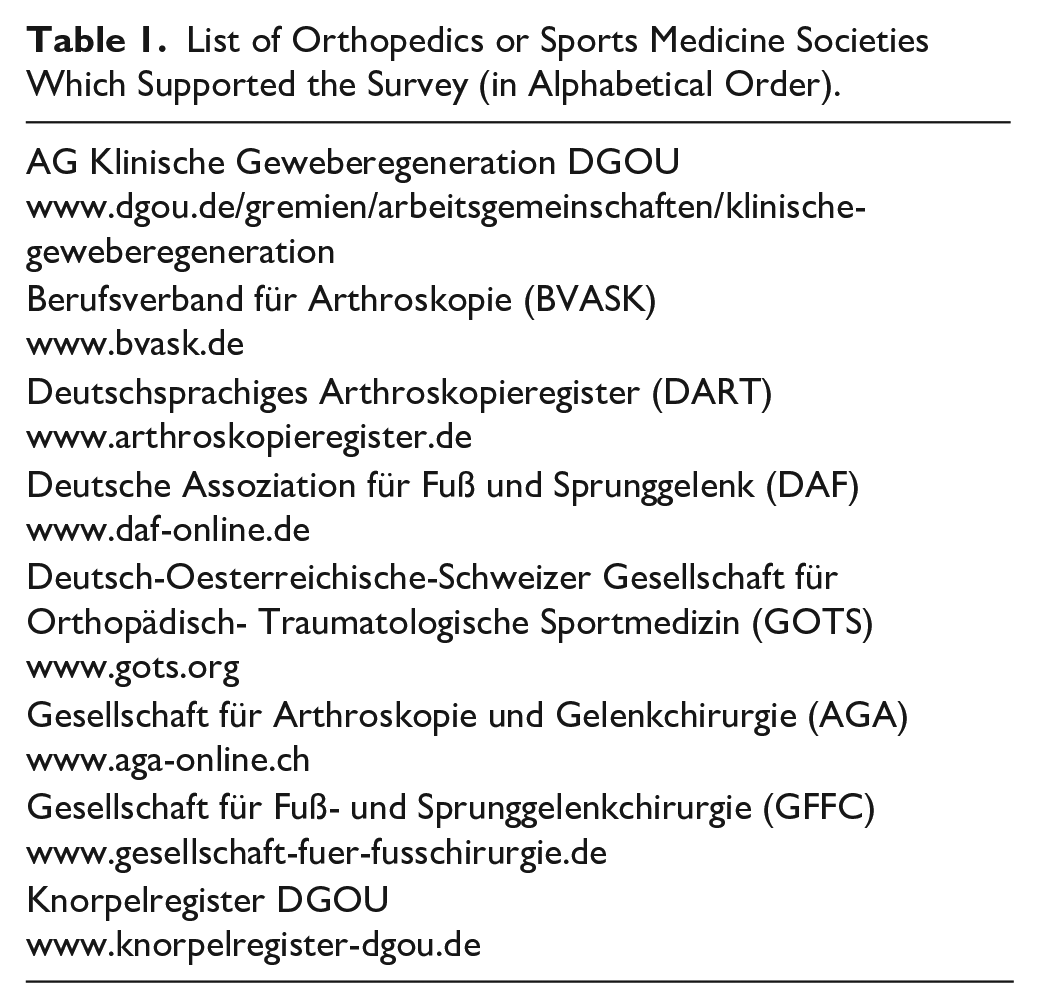
The questionnaire was sent electronically as a PDF file to members of the CTR of the DGOU and the participants of the German Cartilage Registry (Knorpelregister DGOU©). In addition, 6 German-speaking orthopedics or sports medicine societies supported the survey by distributing the questionnaire via their membership database ( Table 1 ).
List of Orthopedics or Sports Medicine Societies Which Supported the Survey (in Alphabetical Order).
The survey commenced on July 4, 2019, and was closed on August 30, 2020. The questionnaire was distributed via e-mail using the databases of the professional organizations. One remainder e-mail was sent. A total of 60 participants returned the questionnaire. Surveys partially completed were included and analyzed for the responses given.
Research Ethics and Patient Consent
This article does not contain any studies with human participants performed by any of the authors. The manuscript conforms to the ICMJE Recommendations for the Conduct, Reporting, Editing, and Publication of Scholarly Work in Medical Journals.
Statistics
The data were analyzed using SigmaPlot 11.0 (SPSS Inc., Chicago, USA). Data are presented as mean ± standard deviation (SD), minimum (min) and maximum (max) value, and the median.
The data were analyzed for normality using the Shapiro-Wilk test. Subsequently, the Student t test (parametric test) or the rank-sum test (non-parametric test) was used. The 1-way analysis of variance was used for multiple comparisons. The Kruskal-Wallis 1-way analysis of variance on ranks was performed in case of a failed normality test, followed by the Tukey test as an all pairwise multiple comparison procedure. Correlations were assessed using Spearman’s rank correlation coefficient; P20-values ≤0.05 were considered significant. Results were classified depending on the consensus within the answers (agreement ≥75% “strong tendency,” 50%-74% “tendency,” 25%-49% “weak tendency,” <25% “no tendency”), as described by Guelfi et al. 20
Results
Questions 1 to 7: Information on the Experience of the Surgeons
Figure 1
shows the different surgical procedures performed by the participants between 2016 and 2018. Refixation of the fragment, retrograde drilling, and bone marrow stimulation with or without using a matrix were performed by at least 75% of the surgeons and was considered a strong tendency. The participants used retrograde cancellous bone graft, osteochondral autologous cylinder transplantation, and autologous chondrocyte transplantation in 43.3%, 45.0%, and 26.7%, respectively; these were considered a weak tendency. The use of osteochondral allograft transplantation and small metal implants was below 25% (15% each), considered as no tendency. There was a strong tendency to stabilize the ankle (76.7%) and perform corrective osteotomies (51.7%). Participants were asked to estimate the number of individual procedures performed (
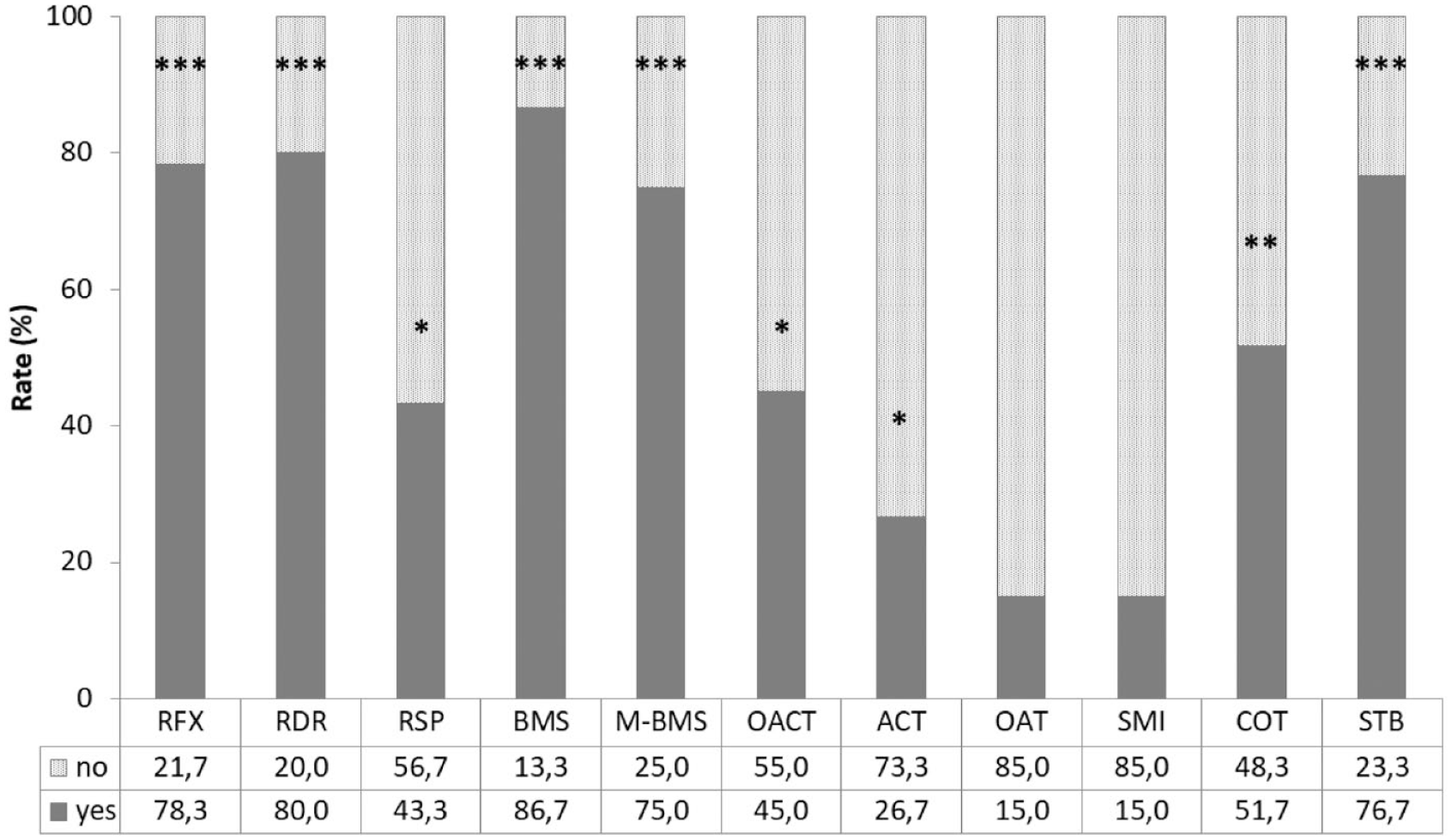
Surgical procedures performed between 2016 and 2018. Data shown as relative amount in percent of all 60 respondents. RFX = refixation of the fragment; RDR = retrograde drilling; RSP = retrograde spongioplasty; BMS = bone marrow stimulation; M-BMS = matrix-associated BMS; OACT = osteochondral autologous cylinder transplantation; ACT = autologous chondrocyte transplantation; OAT = osteochondral allograft transplantation; SMI = small metal implants; COT = corrective osteotomy; STB = stabilization. Answers with a prevalence of at least 75% of respondents were considered a “strong tendency” (***), while a prevalence of at least 50% is a “tendency” (**). Prevalence below 50% but of at least 25% is considered “weak tendency” (*), and below 25% is “no tendency” (no star).
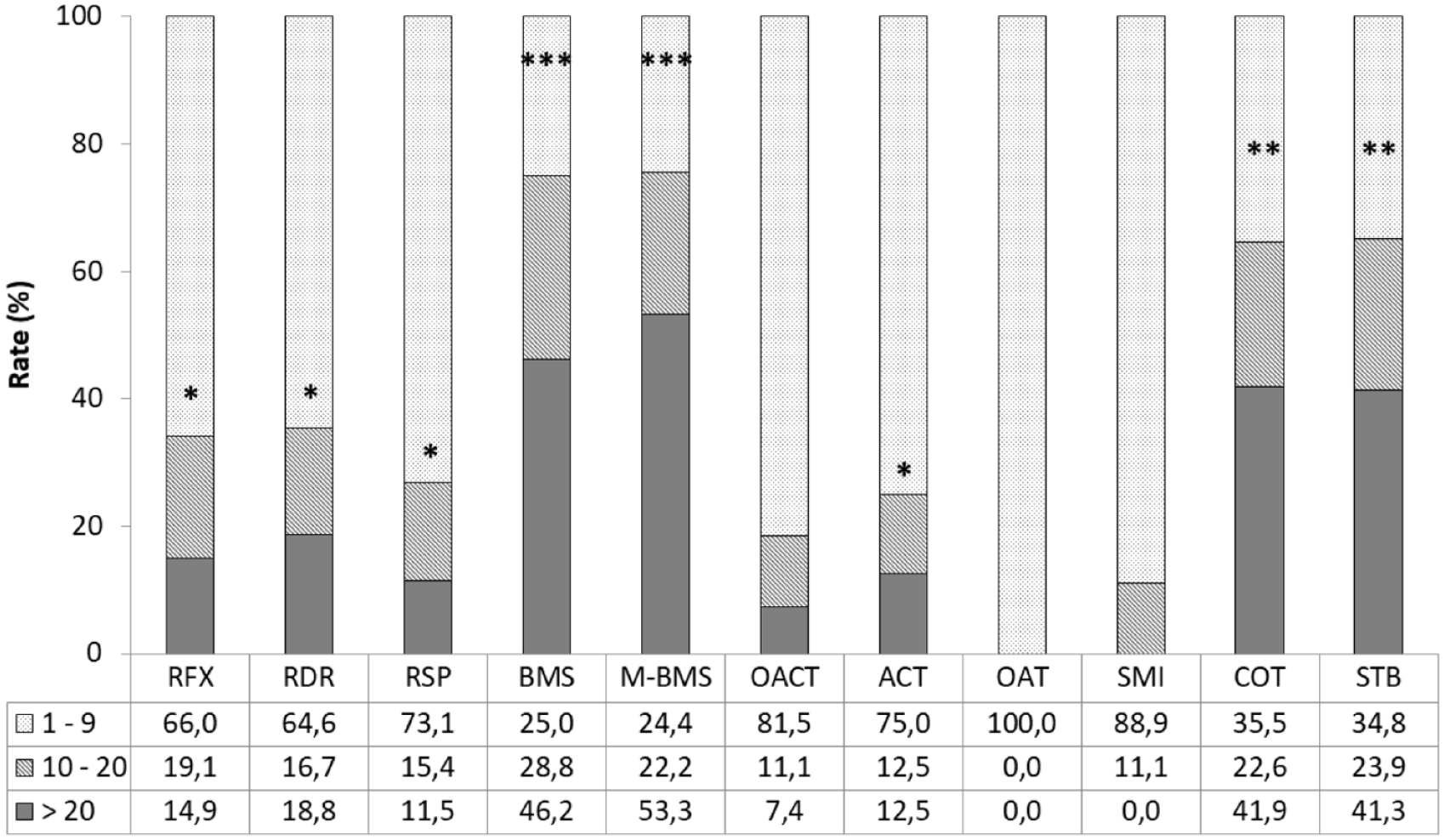
Amount of the surgical procedures in the categories 1 to 9, 10 to 20, and >20 procedures performed between 2016 and 2018. Data shown as relative amount in percent of the individually performed total amount. RFX = refixation of the fragment; RDR = retrograde drilling; RSP = retrograde spongioplasty; BMS = bone marrow stimulation; M-BMS = matrix-associated BMS; OACT = osteochondral autologous cylinder transplantation; ACT = autologous chondrocyte transplantation; OAT = osteochondral allograft transplantation; SMI = small metal implants; COT = corrective osteotomy; STB = stabilization. Considering at least 10 procedures as the threshold, answers with a prevalence of at least 75% of respondents were considered a “strong tendency” (***), while a prevalence of at least 50% is a “tendency” (**). Prevalence below 50% but of at least 25% is considered “weak tendency” (*), and below 25% is “no tendency” (no star).
Corrective osteotomy and ankle stabilization were performed in 64.5% and 65.2% cases, respectively. The surgeons saw no indications for small metal implants (0.0%), and only a few indications for osteochondral allograft transplantation (11.1%) and autologous osteochondral cylinder transplantation (18.5%). Refixation of the fragment, retrograde drilling, retrograde cancellous bone graft, and autologous chondrocyte transplantation were performed in 34.0%, 35.5%, 26.9%, and 25.0% cases, respectively.
Questions 8 to 12: Information About the Indication for Surgery, the Characteristics/Nature of the Lesion, and the Type of Approach
For recommending surgery, the published recommendations of the CTR were taken into account by 71.4% of the respondents (56 out of 60 = 56/60 = 93.3%).12 Moreover, the following criteria were considered: local pain at rest (96.2%), local pain at loading (94.9%), ankle joint locking (98.2%), and imaging (94.8%). Further criteria were (as free text) duration of pain, failed conservative treatment, instability, and positive SPECT. The rate by which certain imaging technologies were used to diagnose an OCLA is shown in Table 2 . Asked about the nature of the lesion, the respondents (58/60 = 96.7%) considered 28.5% as purely chondral and 68.6% as osteochondral. Regarding the surgical technique and approach, the respondents (60/60 = 100%) preferred arthroscopy (53.2%), arthrotomy (31.9%), and osteotomy (16.4%).
Information About the Indication for Surgery, Imaging, the Characteristics/Nature of the Lesion, and the Type of Surgical Technique/Approach.
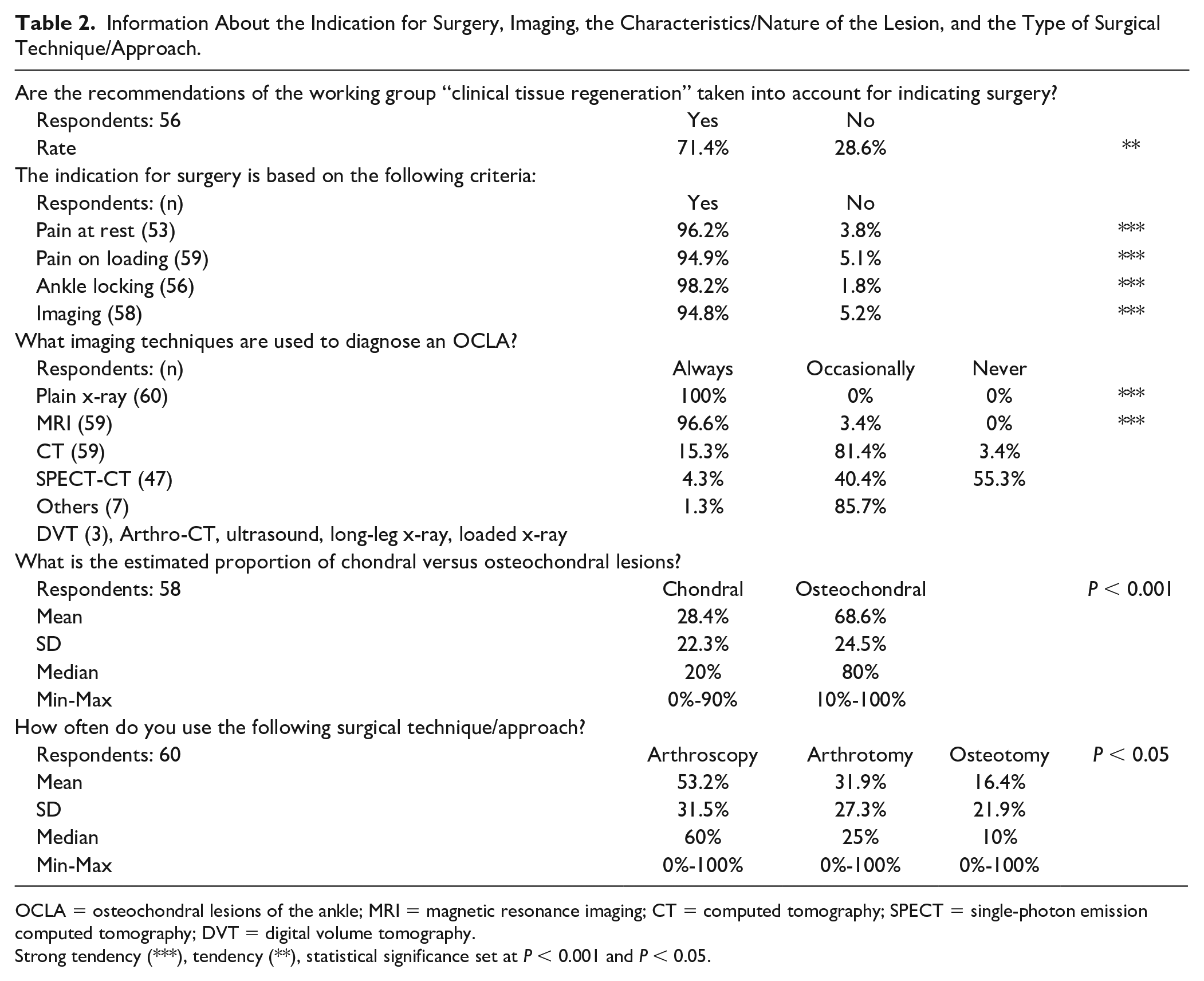
OCLA = osteochondral lesions of the ankle; MRI = magnetic resonance imaging; CT = computed tomography; SPECT = single-photon emission computed tomography; DVT = digital volume tomography.
Strong tendency (***), tendency (**), statistical significance set at P < 0.001 and P < 0.05.
Questions 13 to 25: Information About the Postoperative Care and Rehabilitation Protocol as Well as Recommendations for the Return to Sports Activities
Most participants included published recommendations on postoperative rehabilitation and the return to sports activities in their postoperative management17,21 ( Table 3 ).
Rehabilitation and Return to Sports.
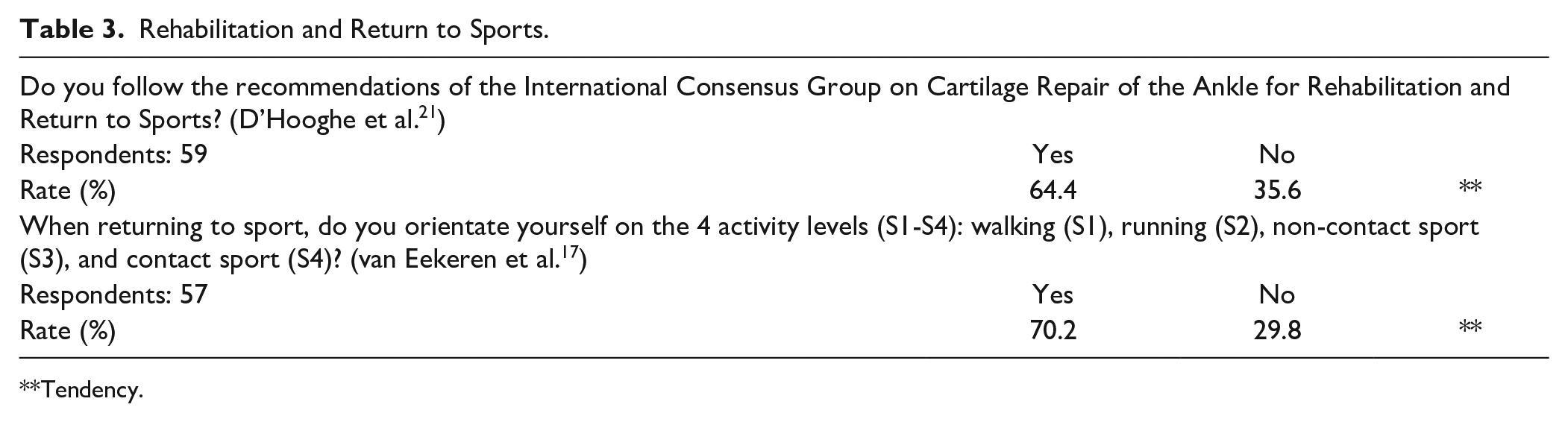
Tendency.
The postoperative management differed depending on the categories, as shown in Figure 3 . The main surgical procedures (regarded as category A) were considered the most critical factor in influencing the postoperative management by 81% of the participants (strong tendency). Adjunct surgical procedures (regarded as category B) such as corrective osteotomy (COT) and stabilization of the ankle (STB) were considered important by 67.8% of the respondents (tendency). The main and adjunct surgical procedures were further analyzed. The results are shown in Table 4 .
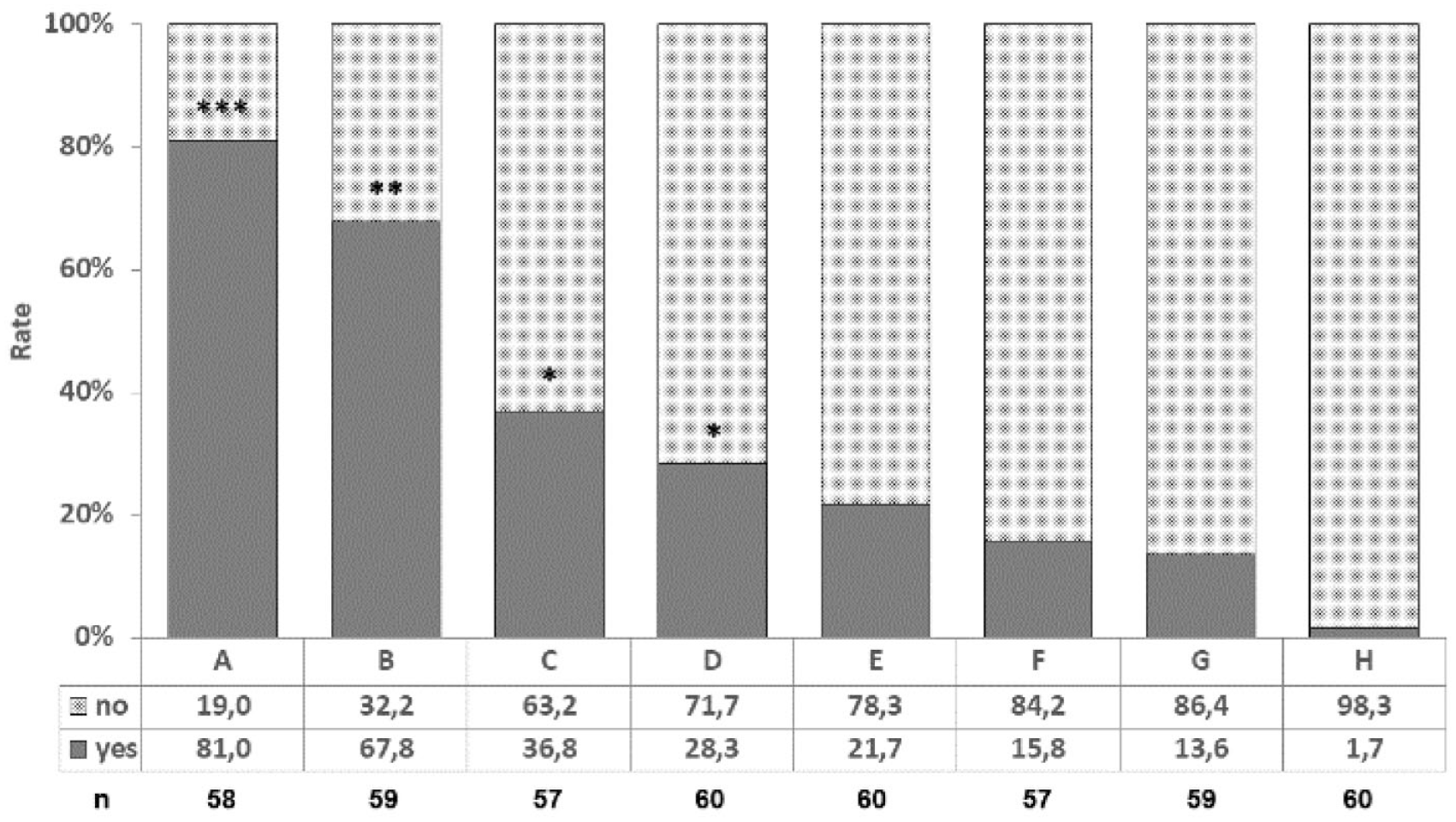
The postoperative management differs depending on the following categories: (
Analysis of the Surgical Procedures Regarding the Postoperative Management.
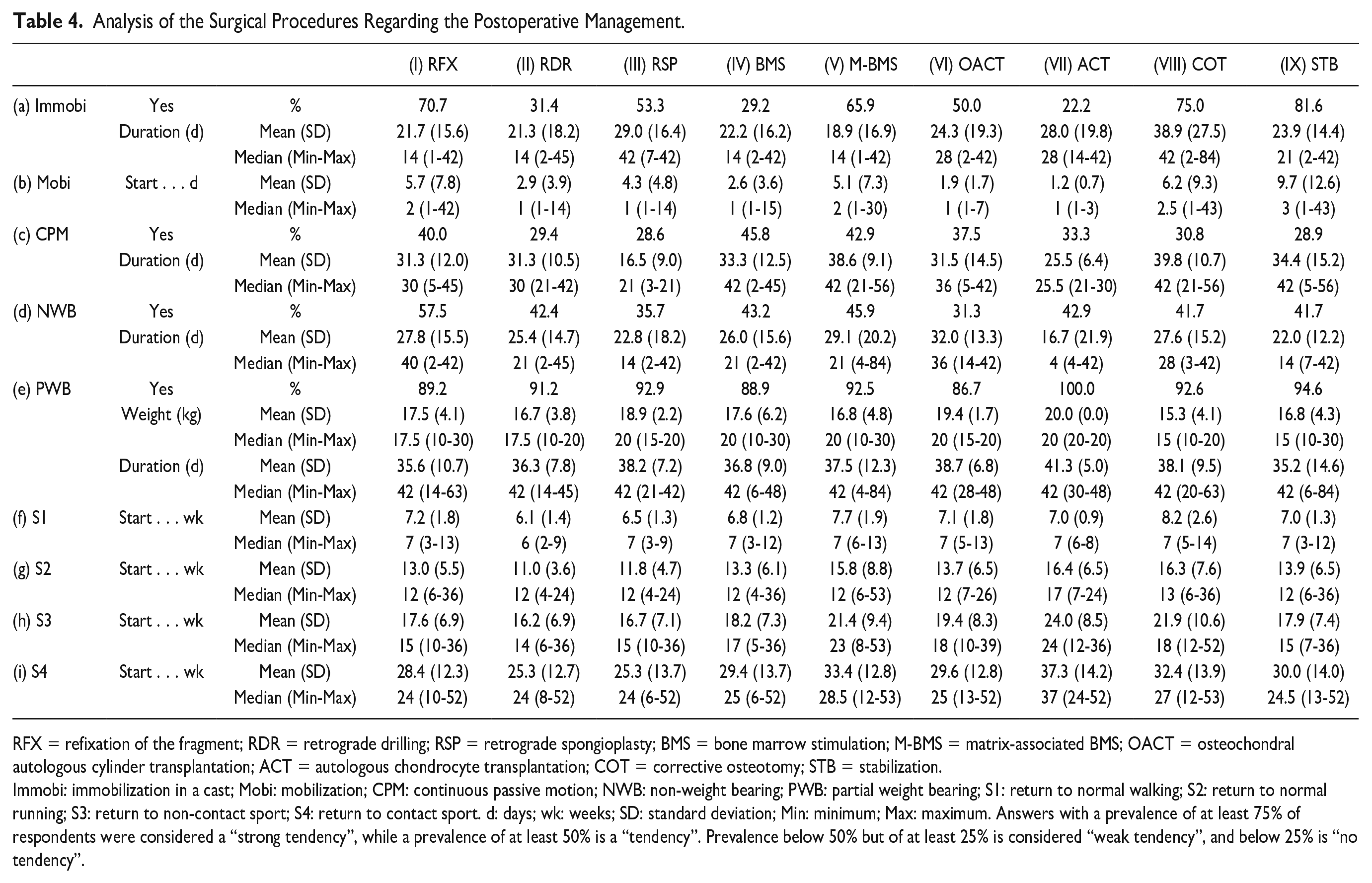
RFX = refixation of the fragment; RDR = retrograde drilling; RSP = retrograde spongioplasty; BMS = bone marrow stimulation; M-BMS = matrix-associated BMS; OACT = osteochondral autologous cylinder transplantation; ACT = autologous chondrocyte transplantation; COT = corrective osteotomy; STB = stabilization.
Immobi: immobilization in a cast; Mobi: mobilization; CPM: continuous passive motion; NWB: non-weight bearing; PWB: partial weight bearing; S1: return to normal walking; S2: return to normal running; S3: return to non-contact sport; S4: return to contact sport. d: days; wk: weeks; SD: standard deviation; Min: minimum; Max: maximum. Answers with a prevalence of at least 75% of respondents were considered a “strong tendency”, while a prevalence of at least 50% is a “tendency”. Prevalence below 50% but of at least 25% is considered “weak tendency”, and below 25% is “no tendency”.
Regarding immobilization, there was a strong tendency for COT and STB, and a tendency for OACT, M-BMS, RSP, and RFX. We found a weak tendency for RDR and BMS, and no tendency for ACT. The duration of immobilization (in days) was lowest for M-BMS (mean ± SD: 18.9 ± 16.9) and highest for COT (mean ± SD: 38.9 ± 27.5). The start of mobilization ranged from 1.2 ± 0.7 days (mean ± SD) for ACT to 9.7 ± 12.6 days (mean ± SD) for STB. Continuous passive motion (CPM) was only a weak tendency in all procedures. For those who use CPM, the duration (in days) was lowest for RSP (mean ± SD: 16.5 ± 9.0) and highest for COT (mean ± SD: 39.8 ± 10.7). There was only a weak tendency in all procedures for NWB mobilization, except for RFX (tendency 57.5%). The duration of NWB (in days) was lowest for ACT (mean ± SD: 16.7 ± 21.9) and highest for OACT (mean ± SD: 32.0 ± 13.3). There was a strong tendency in all procedures for PWB mobilization. The weight (in kg) for PWB was lowest for COT (mean ± SD: 15.3 ± 4.1) and highest for ACT (mean ± SD: 20.0 ± 0.0). The duration of PWB (in days) was lowest for STB (mean ± SD: 35.2 ± 14.6) and highest for ACT (mean ± SD: 41.3 ± 5.0). The time to return to normal walking ranged from 6.1 ± 1.4 weeks (mean ± SD) for RDR to 8.2 ± 2.6 weeks (mean ± SD) for COT. The return to running ranged from 11.0 ± 3.6 weeks (mean ± SD) for RDR to 16.4 ± 6.5 weeks (mean ± SD) for ACT. The return to non-contact sports ranged from 16.2 ± 6.9 weeks (mean ± SD) for RDR to 24.0 ± 8.5 weeks (mean ± SD) for ACT. The return to contact sports ranged from 25.3 ± 12.7 weeks (mean ± SD) for RDR to 37.3 ± 14.2 weeks (mean ± SD) for ACT.
The categories B to H were answered as free text entries by various respondents. In summary, the most important statements regarding the question “Does your postoperative management differ depending on the following categories?” were as follows: ligament surgery and osteotomy determine the follow-up treatment; more restrictive postoperative management for osteotomy than arthrotomy or arthroscopic approach; the larger the lesion, the longer the period for partial load; athletes can exercise earlier if they are pain-free; more rapid loading if good containment of the lesion; and younger patients are allowed to exercise quickly because healing is faster. No entry was made regarding the gender of the patient.
Further details are listed in Supplement 2.
Questions 26 to 36: Issues of Follow-Up and Adjunct Treatments
A summary is shown in Table 5 . In addition, some important free text entries are as follows.
Follow-Up and Adjunct Treatments.
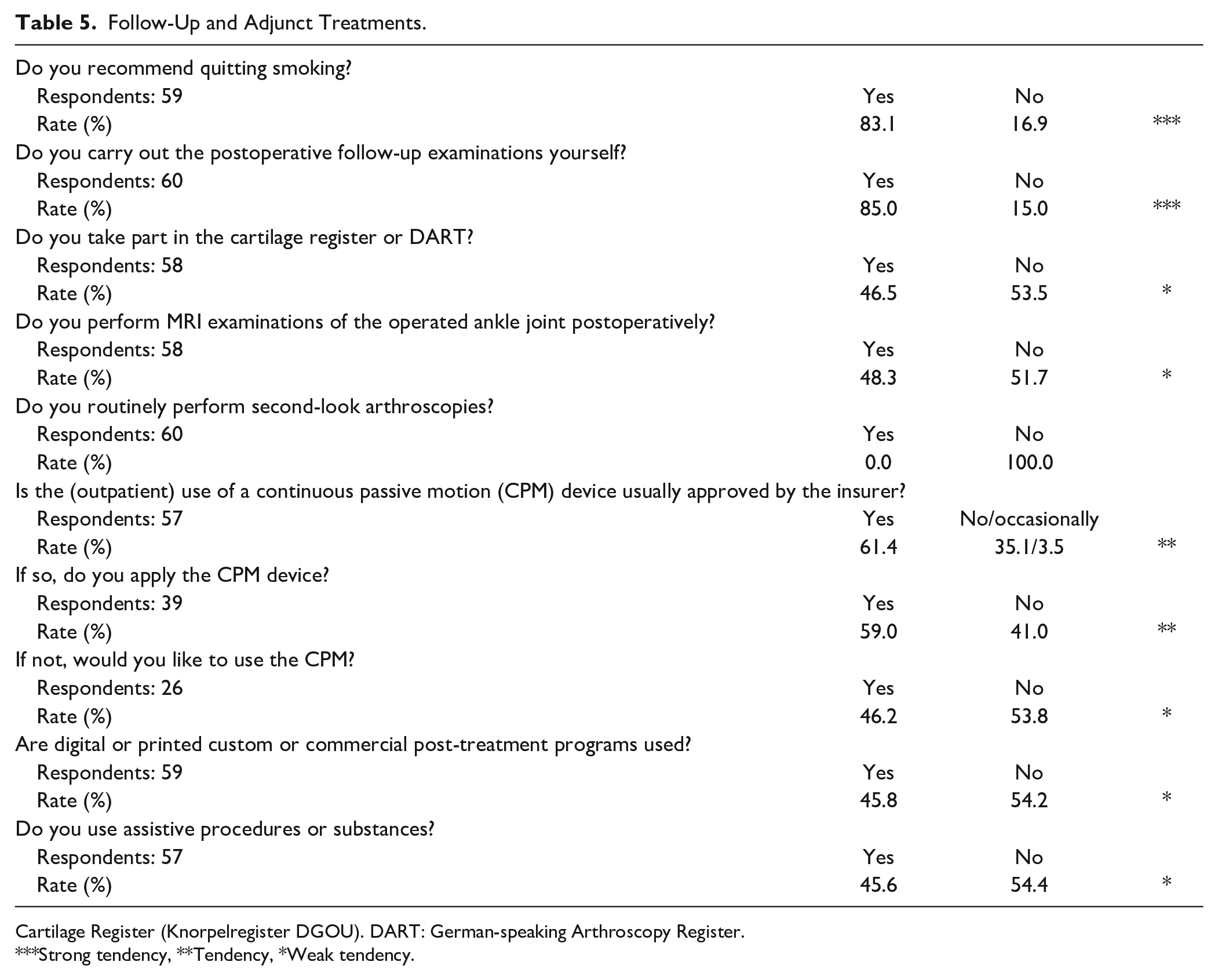
Cartilage Register (Knorpelregister DGOU). DART: German-speaking Arthroscopy Register.
Strong tendency, **Tendency, *Weak tendency.
“At what intervals do the clinical controls take place and for how long?” The answers ranged from “2 and 6 weeks, 3, 6, and 12 months, then annually” and “variable” to “none.”
“Please indicate at what intervals MRI or CT scans take place and up to what point in time postoperatively.” The answers ranged from “. . . imaging utilizing MRI and CT only in the event of clinical abnormalities or abnormal x-rays . . .” to “. . . annually up to 3 years, then individually . . .”
Further details are listed in Supplement 3.
Discussion
In this survey, the main surgical procedure was the most important factor for determining the postoperative management in over 80% of the participants, which is considered a strong tendency. Adjunct surgical procedures (COT, STB) showed agreement in 68% of respondents, which is considered a tendency. The surgical approach and the size of the OCLA showed agreement in 37% and 28% of respondents, respectively, which is considered a weak tendency.
The International Consensus Group on Cartilage Repair of the Ankle reached a strong consensus that rehabilitation is limited by the procedure that requires the most protection, which is often the cartilage repair procedure. 21
In contrast to our findings, the ICRS (International Cartilage Repair Society) states that concomitant procedures typically have no impact on return to sport after cartilage repair of the ankle. 21 Nevertheless, the rehabilitation program may need to address procedure-specific impairments related to the concomitant procedure. For example, in a patient who receives an arthroscopic BMS with realignment osteotomy, the osteotomy is the limiting factor in rehabilitation. Therefore, in osteotomy cases, weight-bearing may be delayed, allowing time for bone healing.
In a worldwide survey on OCLA treatment with over 1800 participants, 20 OCLA surgery was frequently augmented by lateral ligament reconstruction (79%), suggesting a strong link between symptomatic OCLA and ankle instability. 22
Despite this, the impact of ankle stabilization on the outcome of OCLA surgery remains unclear.11,15 A recent comparative study showed similar clinical outcomes in patients treated for OLT with and without chronic ankle instability, but increased failure rates and inferior performance in sports and recreational activities were observed in patients with instability. 23 The postoperative management and rehabilitation process for an ankle cartilage injury requires a multidisciplinary and comprehensive approach. Ideal postoperative protocols are still controversial, and clear evidence is lacking regarding when the patients can progress with weight-bearing or return to activities of daily living or sport. Delay in weight-bearing for approximately 4 to 6 weeks post-surgery has often been recommended to limit shear forces and facilitate biological healing, although current literature recommends a variable timeframe, spanning 2 to 6 weeks depending on the lesion’s characteristics and the nature of the surgical procedure. 24 Such variability is similarly corroborated by the worldwide survey, as no tendencies were recorded: 38% of respondents permitted weight-bearing between 4 and 6 weeks, 25% between 2 and 4 weeks, and 28% waited until after reaching at least 6 weeks of the postoperative period. Moreover, the lesion’s characteristics were typically not considered in formulating this decision, perhaps explaining response heterogeneity. 20 OCLAs can substantially affect the overall quality of life and athletic performance, resulting in the delay or inability of an athlete to train or compete.25-27 The rehabilitation’s primary goal is to return the patient to pre-injury activity level without pain, which is particularly important for athletes. Concerning athletes, the time to return to high-impact sports after operative treatment of OCLA ranges from 3 to 6 months and is dependent mainly on the type of lesion and specific treatment strategy employed. 28
To our knowledge, no objective criteria exist to assist clinicians with progressing rehabilitation activities after cartilage repair of the ankle. There is a strong consensus among international foot and ankle experts that the general concepts of rehabilitation to consider in returning patients to activities of daily living, recreational, and/or elite athletic activities after cartilage repair of the ankle are (1) allowing biological healing by limiting shear forces and (2) progression of activities based on a clinical evaluation. 21
The progress of the rehabilitation activities can be adjusted according to the following aspects: (1) pain, (2) proprioception, (3) stability, and (4) swelling.
There is a strong consensus among international foot and ankle experts that early weight-bearing is beneficial, so long as the shear forces are minimized and should be utilized after the ankle’s cartilage repair. Early weight-bearing is defined as beginning at 4 weeks postoperatively. The same is true for early motion that can begin within 1 week following surgery and include a free, active motion. Maneuvers such as forced passive movements that extend the patient beyond their available range of motion should be avoided. 21 Studies show that early weight-bearing can be used in postoperative protocols without causing apparent adverse effects in the setting of arthroscopic bone marrow stimulation.29,30 The rehabilitation course in more extensive or secondary lesions depends on the specific operative technique but generally involves more prolonged periods of partial weight-bearing.
Procedures involving malleolar osteotomy or other bony fixation require 6 weeks of non-weight-bearing. 31 Rehabilitation should follow the biological phases of healing. Full range of motion (ROM), a regular running pattern without pain, and a 90% preinjury score on functional tests are considered the minimal requirements for return to play (RTP). 28
A continuous passive motion (CPM) device was used by less than 50% of respondents. In about 40%, the CPM was not approved by the health care insurance, which might explain the weak tendency to use CPM. Almost 50% of the attendees would have liked to use the CPM if the health care insurance had approved it. Previous animal studies have revealed that CPM demonstrated faster healing and thicker cartilage with an increased concentration of proteoglycans compared to cast immobilization.32,33 Moreover, published literature shows that CPM started immediately after surgery seems to be an effective method for allowing complete and quick recovery of the ankle’s range of motion, reducing the risk of early degenerative joint disease.34-36
Regarding assistive procedures or substances, biological treatments (e.g., hyaluronic acid, platelet-rich plasma) comprise an additional topic of frequent debate without formal evidence-based treatment guidelines. Although several high-quality in vitro and in vivo studies have demonstrated the potential effects of biological products on cartilage repair, relatively few comparative and randomized controlled clinical trials exist to assess these therapies’ role in the management of cartilage lesions of the ankle.37-39 In this regard, the type of therapy, timing of use, and biological composition (e.g., cellular vs. acellular) of specific treatments remain primarily based on expert opinion, with limited high-level evidence available in the literature.
In summary, due to the insufficient evidence of the postoperative management and rehabilitation of surgically treated OCLA, this survey provides helpful information to support the individual professional judgment and resulting clinical decision.
However, the study’s limitation is that the survey has been developed based on expert opinion rather than through a validated methodology. Another important issue is the absence of case load and surgeon experience information, as well as the individual clinical setting. Moreover, detailed information regarding the reason for certain procedures has not been questioned because the main issue of this survey is to obtain quantitative information, and not necessarily answering the question “why” something was performed or not performed. Nonetheless, the lack of high-quality clinical evidence to date in this field encouraged us to seek alternative methods for developing best practice guidelines in conjunction with specialized foot and ankle surgeons. Further high-level studies are required to substantiate the results of this survey.
The questionnaire was distributed via e-mail using the membership databases of the professional organizations, which have several thousand members altogether. It was stated in the cover letter that only those members who specialized in the treatment of OCLAs should return the questionnaire. Based on this information, it is not possible to calculate a response rate.
Conclusion
The management of OCLA varies among German-speaking foot and ankle surgeons and is based on a low level of evidence. Therefore, guidelines remain essential to standardize the management of OCLA, to achieve improved and stable results. This survey will assist clinicians and patients with rehabilitation to return to sports after treating the ankle’s cartilage injury.
Supplemental Material
sj-docx-1-car-10.1177_19476035231213184 – Supplemental material for Postoperative Management of Osteochondral Lesions of the Ankle: A Survey Among German-Speaking Foot and Ankle Surgeons
Supplemental material, sj-docx-1-car-10.1177_19476035231213184 for Postoperative Management of Osteochondral Lesions of the Ankle: A Survey Among German-Speaking Foot and Ankle Surgeons by Aurich Matthias, Christoph Becher, Sarah Ettinger, Oliver Gottschalk, Daniel Guenther, Kajetan Klos, Marc-Daniel Ahrend, Daniel Körner, Christian Plaass and Markus Walther in CARTILAGE
Supplemental Material
sj-docx-2-car-10.1177_19476035231213184 – Supplemental material for Postoperative Management of Osteochondral Lesions of the Ankle: A Survey Among German-Speaking Foot and Ankle Surgeons
Supplemental material, sj-docx-2-car-10.1177_19476035231213184 for Postoperative Management of Osteochondral Lesions of the Ankle: A Survey Among German-Speaking Foot and Ankle Surgeons by Aurich Matthias, Christoph Becher, Sarah Ettinger, Oliver Gottschalk, Daniel Guenther, Kajetan Klos, Marc-Daniel Ahrend, Daniel Körner, Christian Plaass and Markus Walther in CARTILAGE
Supplemental Material
sj-docx-3-car-10.1177_19476035231213184 – Supplemental material for Postoperative Management of Osteochondral Lesions of the Ankle: A Survey Among German-Speaking Foot and Ankle Surgeons
Supplemental material, sj-docx-3-car-10.1177_19476035231213184 for Postoperative Management of Osteochondral Lesions of the Ankle: A Survey Among German-Speaking Foot and Ankle Surgeons by Aurich Matthias, Christoph Becher, Sarah Ettinger, Oliver Gottschalk, Daniel Guenther, Kajetan Klos, Marc-Daniel Ahrend, Daniel Körner, Christian Plaass and Markus Walther in CARTILAGE
Footnotes
Acknowledgments and Funding
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This article does not contain any studies with human participants performed by any of the authors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.