
Abstract
Objective:
Patients frequently use the internet as a source to obtain health information. The purpose of this study was to evaluate the quality and readability of online resources on the diagnosis and treatment of ankle osteochondral lesions (OCLs).
Design:
Three search terms (“ankle cartilage defect,” “cartilage injury,” “ankle cartilage damage”) were entered into 3 search engines (Google, Yahoo, and Bing). The first 20 websites from each search was collected excluding websites intended for health care providers. The quality of the websites were evaluated using the DISCERN instrument, JAMA benchmark, and a Quality rating criteria specific to ankle OCL. The readability was assessed using Flesch Reading Ease (FRE) and Flesch-Kincaid Grade Level (FKGL). Statistical analysis was performed using one-way analysis of variance.
Results:
A total of 41 websites were reviewed. The mean quality ratings were poor across the assessment tools: DISCERN = 38.5 ± 9.0 (range, 23.7-56.7) out of 80; JAMA = 1.0 ± 1.1 (range, 0-3.3) out of 4; and Quality rating criteria = 11.3 ± 4.6 (range, 4-20.7) out of 24. The mean FRE and FKGL were 40.7 ± 32.0 (range, −152.3 to 60.2) and 13.5 ± 10.8 (range, 8.4-80.7), respectively; higher than the recommended reading level for patients (fifth grade).
Conclusions:
The quality and readability of credible sources for ankle OCL were poor, which could lead to misinformation. This study should guide the improvement of online information on ankle OCL.
Introduction
As of April 2019, four billion unique users have internet access on their phones, making access to health-related information easier than ever. 1 Up to 80% of internet users utilize search engines to look up their symptoms, diagnosis, prognosis, and treatment options. 1 Although the internet allows physicians to access the latest guidelines and most up-to-date studies, it also provides patients with an easy way to access health-related information; it can contain incorrect information that can be inaccurate and biased.2,3 Several studies evaluated the quality and readability of websites on a variety of orthopedic topics; however, none were done for ankle osteochondral lesions (OCLs).
OCLs are common, with cartilage injuries occurring in up to half of all ankle sprains. Furthermore, cartilage repair and restoration procedures are becoming more prevalent with an increase in the number of patients presenting with isolated cartilage lesions. 4 An untreated ankle OCL can lead to chronic ankle pain and osteoarthritis.5-7 There are numerous management methods available for ankle cartilage defects, and choosing the form of management can be difficult for patients, and they may refer to online information for assistance.4,8-10 Unfortunately, the plethora of inaccurate information online makes the surgeons’ life so much harder because patients develop inaccurate expectations. Furthermore, the term “cartilage injury/defects” is often confusing to patients, especially those who do not understand the difference between focal cartilage defect and arthritis. It is important for physicians to critically evaluate online resources discussing OCL in the ankle to help guide patients toward high-quality and readable information.
The purpose of this study was to review the quality and readability of online resources on the topic of ankle OCL. We hypothesized that the material online would not differentiate between osteoarthritis and ankle OCL, would be of poor quality, and would be at a higher level than what is recommended for patient education materials by The Joint Commission (fifth-grade level), 11 further contributing to patient misinformation. We also hypothesized that the quality of websites would vary with the different search terms, and may even vary based on the frequency they appear among the different search terms.
Methods
Three search terms were defined: “ankle cartilage injury,” “ankle cartilage defect,” and “ankle cartilage damage.” Since Google, Yahoo, and Bing are the search engines used by 92% of surfers, all 3 search engines were used. 12 The search was done in April 2020, clearing the cache, cookies, and search histories before each search. The first 20 search results were included, excluding sponsored advertisements and websites intended for health care providers. According to Forbes, the first 5 results on the first page receive 67.6% of clicks, whereas the next 5 receive 3.73%. In addition, 92% of click occur on the first page. In light of that, and considering that the range of links displayed on each page is 9 to 10, the websites beyond the first pages (past 20) are rarely accessed and it would increase the risk of reporting inaccurate results. An overview of the search methodology and the inclusion/exclusion criteria are shown in Figure 1 .
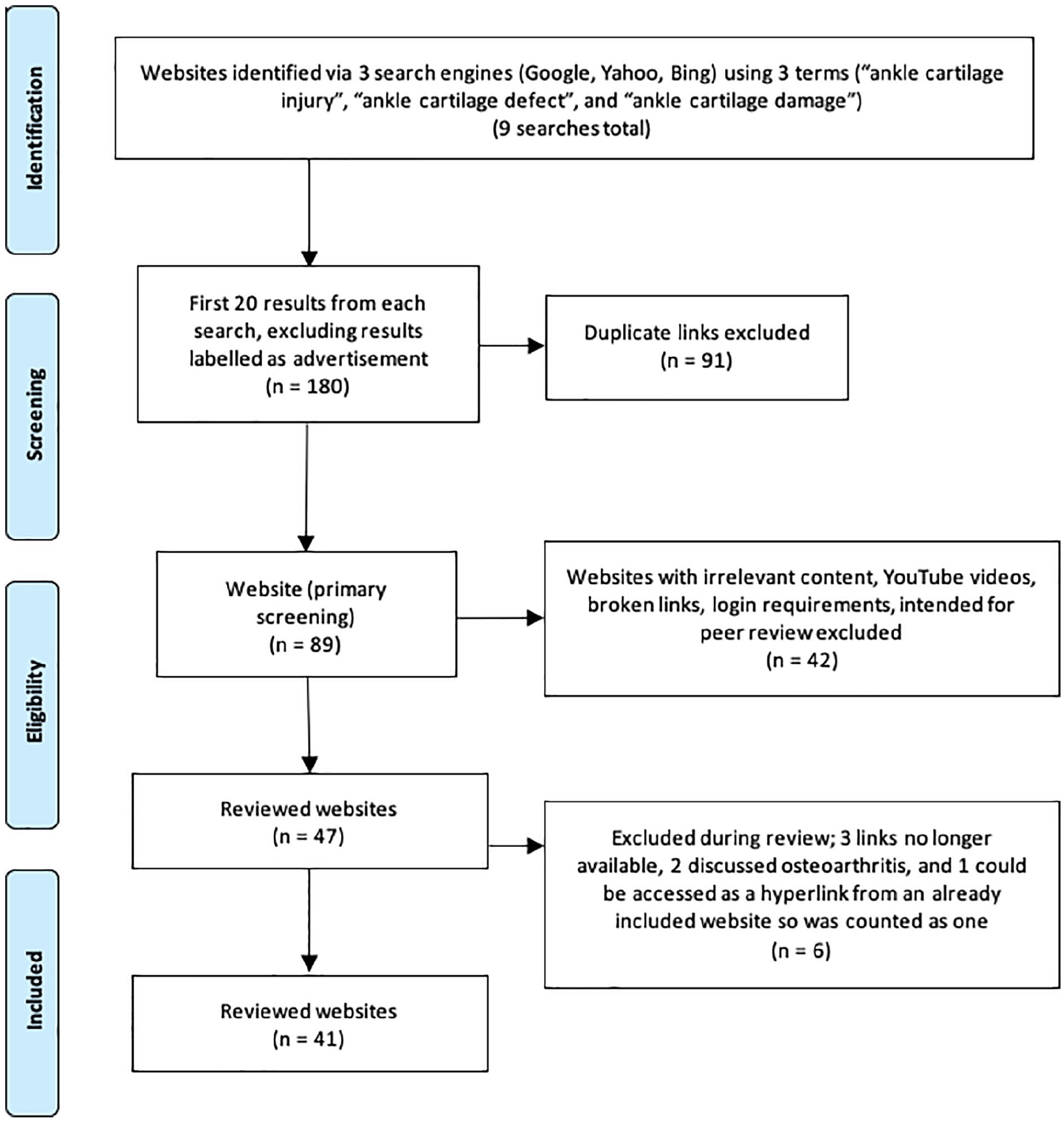
Search algorithm for online health-related material on ankle cartilage defects. Forty-one websites were identified for review, after the stepwise exclusion criteria.
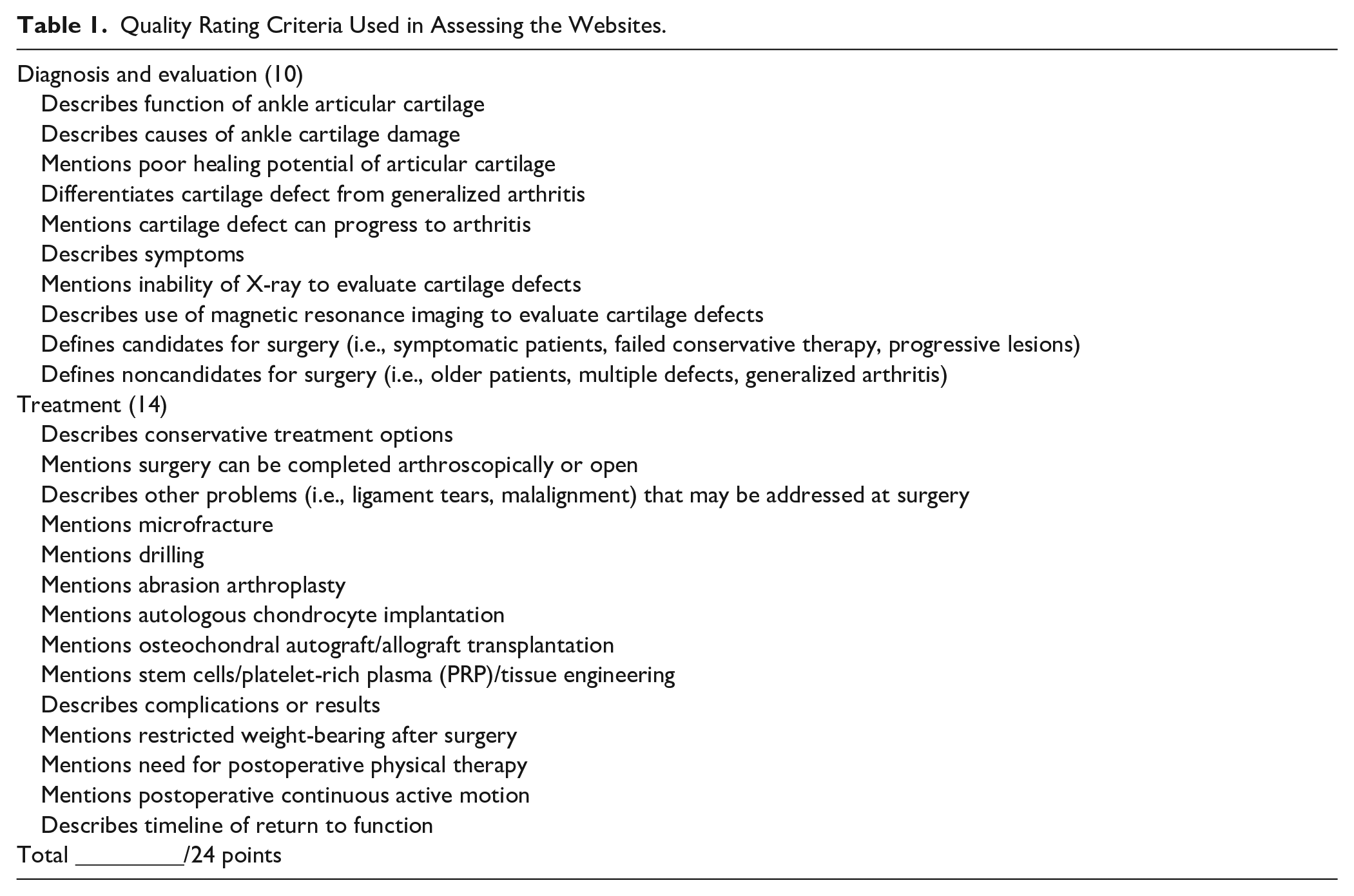
The quality was assessed using methods similar to previous published studies in orthopedics.4,8,10,13,14 The websites were collected by a single researcher (LA) who did not evaluate the quality. They were then randomized and provided to 3 orthopedic surgeons (YS, HU, and JFD) to assess their quality. Quality was assessed using 3 tools: DISCERN instrument score (Suppl. Appendix 1), JAMA score, and a Quality rating criteria ( Table 1 ). Psychometrics were not assessed in this article.
Quality Rating Criteria Used in Assessing the Websites.
The DISCERN instrument score (Suppl. Appendix 1) is composed of 3 sections scored out of a maximum of 80 points. The first evaluates the reliability (40 points), the second assesses the quality of the discussed treatments (35 points), and the third gives an overall rating of the source (5 points). The scores can be interpreted as follows: 63 to 80 points = excellent; 51 to 62 = good; 39 to 50 = fair; 27 to 38 = poor; 15 to 26 = very poor. 15 Each question is scored out of 5 where 1 = no = serious or extensive shortcomings; 3 = partially = potentially important but not serious shortcomings; 5 = yes = minimal shortcomings.
The JAMA score is composed of 4 core components. Authorship was awarded if the author’s credentials and affiliations were provided. Attributions was awarded if the information was referenced. Disclosure was awarded if sponsorship or conflicts of interest were disclosed. Currency was awarded if the issue date, and any updates were documented. 16 Each component was awarded 1 point, giving each website an overall score out of 4.
The Quality rating criteria ( Table 1 ) was modified from a previous study 4 to address the ankle. It is composed of 24 criteria—each awarded a point—addressing the anatomy, diagnosis, treatments, and rehabilitation based on the American Academy of Orthopedic Surgeons guidelines. 17
The readability of the websites was assessed by LA using a preprogramed online calculator. 18 The calculator was used to generate a Flesch Reading Ease score (FRE) and a Flesch-Kincaid Grade Level (FKGL). A lower score corresponds to better readability as texts with high scores are more difficult to understand ( Table 2 ). The grade recommended for health care–related information is fifth-grade level or lower, which corresponds to an FKGL of 5 and below. The assessment tools used have different formulas but they all take into account the length of the sentences and words used, as well as the number of syllables. The number of syllables affects the FRE more than it does FKGL. There was an outlier scored −152.3 on FRE and 80.7 on FKGL, which is out of the FRE range and beyond the college level range 13 to 16 on the FKGL. The outlier was removed and the calculations were repeated.
Readability Scales Interpretation.
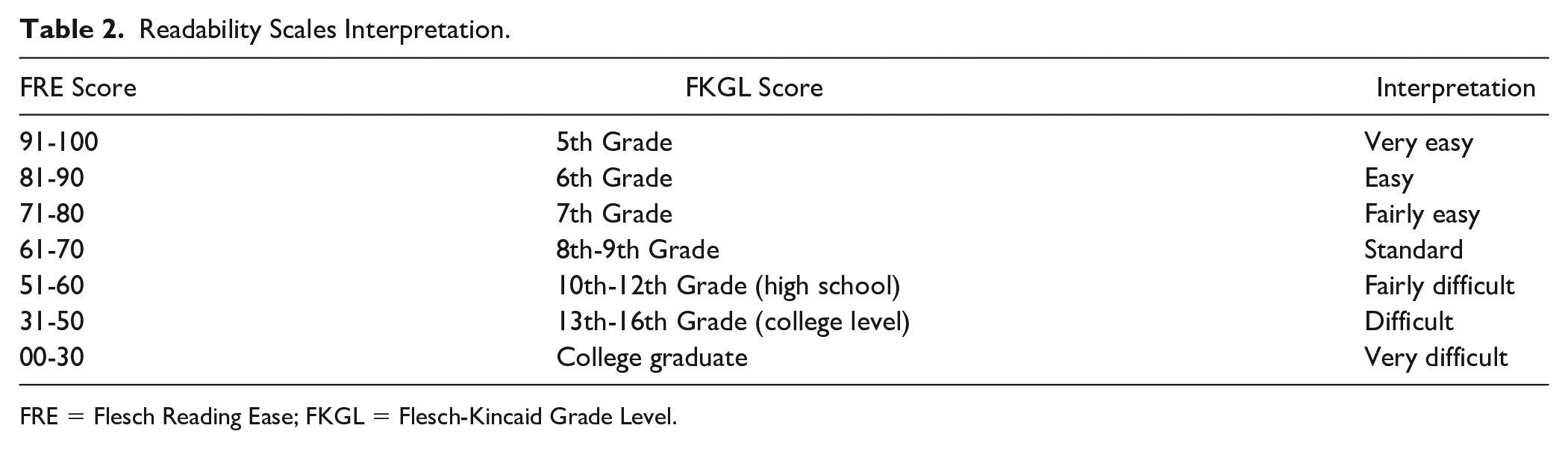
FRE = Flesch Reading Ease; FKGL = Flesch-Kincaid Grade Level.
Health care affiliation was determined for each website by LA. Any website containing hospital/health care provider affiliation was deemed health care–affiliated. The commercial bias was also assessed by 3 orthopedic surgeons (YS, HU, and JFD). The website was considered commercially biased if there were advertisements on the page, irrespective of the type of advertisement displayed.
Statistics
The average and standard deviation of the DISCERN, JAMA, Quality criteria, FRE, and FKGL scores were calculated for all the websites. The websites were sorted into 3 groups based on search term, and the average and standard deviation were calculated. The one-way analysis of variance (ANOVA) was used to compare the scores of the 3 groups. The websites were then sorted based on the number of search terms that retrieved each website. The same process was repeated.
Results
Forty-one websites were included: 27 appeared under “ankle cartilage defect,” 19 under “ankle cartilage injury,” and 24 under “ankle cartilage damage,” with some websites overlapping (Suppl. Appendix 2). The websites were then sorted into 3 groups based on the number of search terms that retrieved them; 23 appeared in one search, 7 appeared in two, and 11 appeared in all three. Six website contained commercial bias (15%), and 4 had no health care affiliation (10%).
The surgeons scoring the quality of sites were in agreement for the most part. In instances where the surgeons’ scores varied considerably, a secondary evaluation was done by the surgeon whose score was farthest away from the other two (without sharing the other surgeon’s marking).
The mean DISCERN instrument score for all websites was 38.5 ± 9.0 (range, 23.7-56.7) out of 80 points. The subscale scores for reliability, quality of treatment, and overall rating are shown in Table 3 . The questions under reliability with mean scores below 2 out of 5 were questions 4 and 5 (1.7 and 1.8 points), also question 8 (1.8 points). As for the quality of treatment component, the highest score (3.8 points) was earned by question 14. The questions scoring below 2 were questions 11, 12, 13, and 15 (1.8, 1.6, 1.7, 1.9 points, respectively; Suppl. Appendix 3).
Summary of Quality and Readability Results.
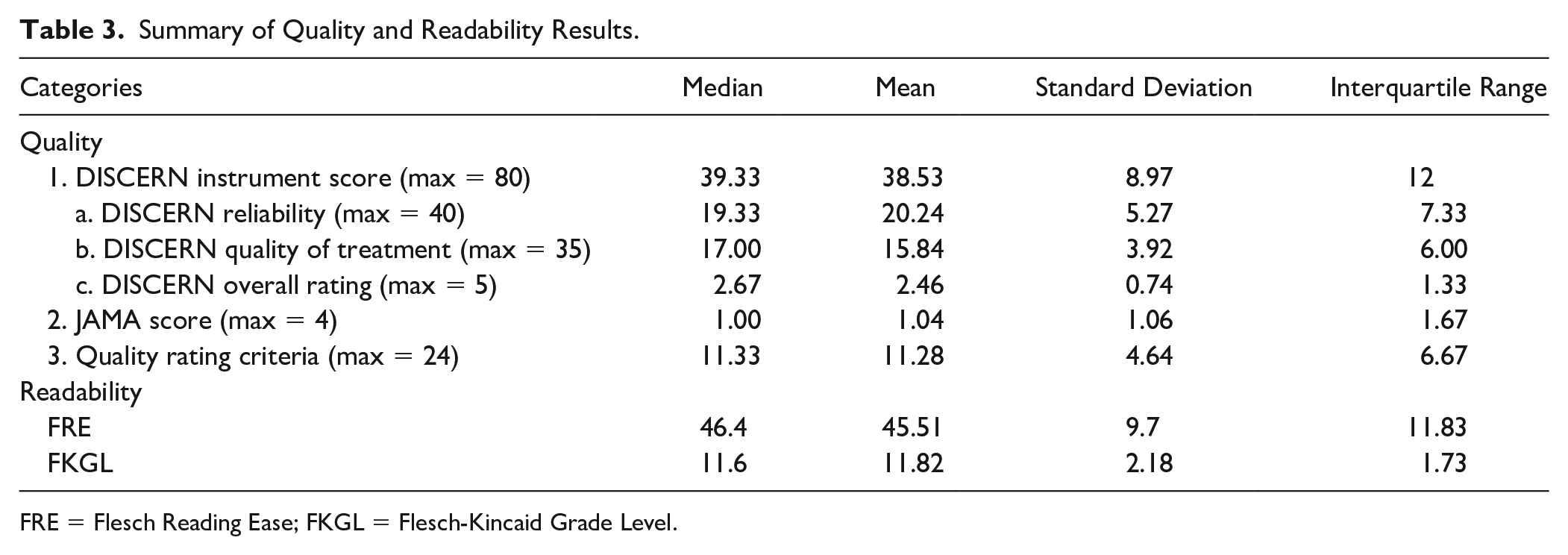
FRE = Flesch Reading Ease; FKGL = Flesch-Kincaid Grade Level.
The mean JAMA score for all websites was 1.0 ± 1.1 (range, 0-3.3) out of 4 points. There were only 2 websites which earned all 4 points. The percentage of websites earning each point were 38% in Authorship, 35% in Currency, 24% in Attribution, and only 9% in Disclosure. The 2 points most frequently earned were the authorship and currency points. Contrarily, the least earned point was the disclosure.
The mean Quality rating score for all websites was 11.3 ± 4.6 (range, 4-20.7) out of 24 points ( Table 3 ). The majority of websites addressed the causes (86%) and the symptoms (88%). Some websites delved into details such as mentioning the poor healing potential of ankle OCLs (41%), differentiating localized OCLs from generalized arthritis (46%), and describing the possibility of progressing from OCLs to arthritis (43%). Although there were quite a few websites that defined the candidates for surgery (53%), there were much less that defined the noncandidates (17%). As for the treatment options, many websites addressed osteochondral autograft/allograft transplantation (72%). Almost half discussed drilling (57%) and microfracture (54%); however, a total of 77% of websites mentioned either drilling or microfracture. The less frequently mentioned treatments were autologous chondrocyte implantation (37%), and stem cells/PRP/tissue engineering (24%). Most websites did not address the postsurgical complications/outcomes (35%), the need for postoperative physical therapy (28%), or the timeline of return to function (27%).
There was an outlier in the data which was omitted and the mean FRE and FKGL scores were calculated accordingly. The mean FRE score for all websites was 45.5 ± 9.7 (range, 10.1-60.2), falling in the range 30 to 49, which is “difficult” to read. The mean FKGL score for all websites was 11.8 ± 2.2 (range, 4-18.8), which is an 11th grade level in the United States ( Table 3 ).
The websites were sorted based on the search term that retrieved them: “ankle cartilage injury,” “ankle cartilage defect,” and “ankle cartilage damage.” There was no significant difference between the average quality and readability of different search terms. The results are shown in Table 4 .
Results of Different Search Terms.
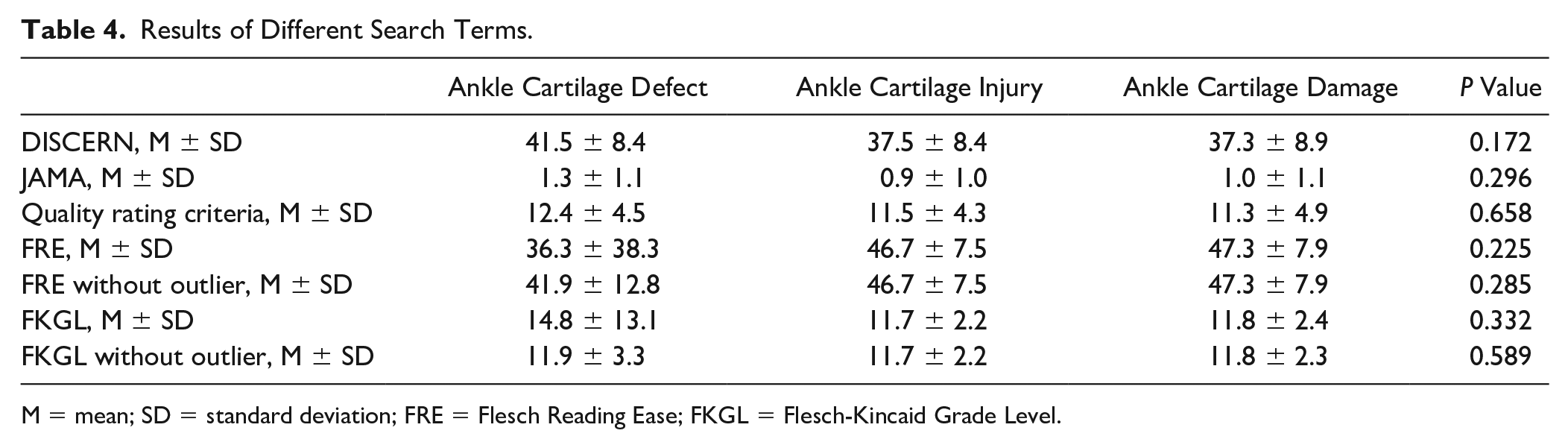
M = mean; SD = standard deviation; FRE = Flesch Reading Ease; FKGL = Flesch-Kincaid Grade Level.
The websites were also sorted based on the number of search terms they appeared under: 1 out of 3, 2 out of 3, and 3 out of 3. There was no significant difference among those 3 categories. The results are shown in Table 5 .
Mean and Standard Deviations of Websites Based on the Number of Search Terms Yielding Them.
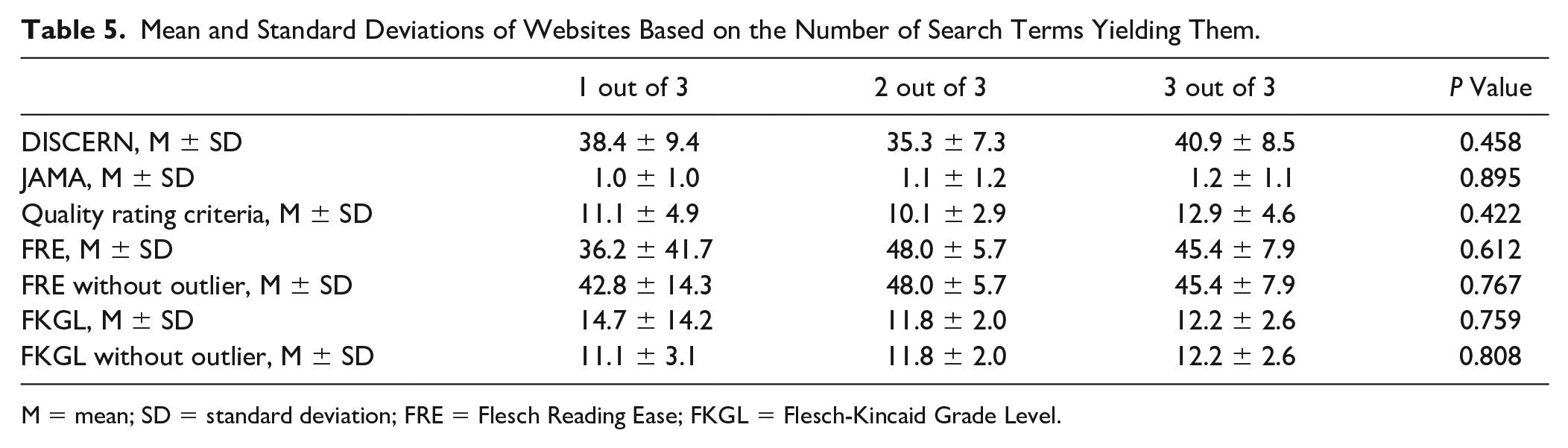
M = mean; SD = standard deviation; FRE = Flesch Reading Ease; FKGL = Flesch-Kincaid Grade Level.
Discussion
The internet has become a primary source for obtaining health-related information by patients. However, the quality and readability of the contents are not regulated. Therefore, patients should be cautious on the reliability of online resources. The current study demonstrated that the overall quality and readability of online websites discussing ankle OCL were poor. This is in line with most studies reviewing orthopedics online material.4,8-10,14,19,20 These findings are concerning, as patients often rely on those online resources to diagnose their conditions and make treatment decisions, which is critical for their outcomes.
The overall DISCERN score was low; however, when the score was broken down into its components we found that the reliability of the sources was slightly higher than the quality of the sources. Although most websites had clear aims and achieved them, the limitation in reliability (Suppl. Appendix 1) of the majority of websites was due to lack of referencing and addressing areas of uncertainty. As for the quality of treatment component, most of the websites mentioned that there are multiple treatment options; however, the downfall for the majority of websites was that there was little to no mention of the risks and benefits of each treatment. Overall, the information lacked any support for shared decision making.
The DISCERN tool findings were in line with the Quality criteria scores. It did, however, highlight an important point; the fact that less than half of the websites describe the difference between and the possibility to progress from OCL to generalized arthritis, despite the lack of understanding in the general population between focal osteochondral defects and arthritis.4,21 This dearth of information can lead to confusion for patients with ankle arthritis who may seek alternative options to joint arthrodesis or arthroplasty. 22 Last, the treatment section of the Quality criteria made it clear that some treatments are more frequently mentioned than others, and most websites did not even mention the risks of treatments or posttreatment rehabilitation and recovery. Further contributing to the challenge faced by doctors as it can be difficult to assist patients with understanding how their requirement for surgical intervention or lack thereof is due to certain characteristics unto the lesion itself. Unfortunately, the poor quality of reliable online materials makes the physician’s role even more challenging as they now have to convince their patients that what they read in what may appear to be a reliable source does not cover all aspects and that either the suggested treatments do not apply to their case or their case requires a treatment which was not suggested by these websites.
The JAMA criteria further attested to the findings of the Quality criteria and DISCERN tool. Of note, a small number of websites earned 1 of the 4 JAMA criteria points, and even fewer websites earned more than 1 point. This means that on average websites disclosed only one JAMA criterion; either authorship, attribution, disclosure, or currency. Both disclosure of authorship—very important aspect to determining the credibility of the source—and currency—important due to the dynamic nature of the field—are relevant in determining the quality of the websites. Attributions are equally important because even if the author was an expert in the field, evidence-based information is the essence of the medical field. Disclosure of any conflict of interest will also enable the reader to determine possible bias.
As for the readability of the websites the overall FRE was “difficult,” while the overall average FKGL was at a high school senior reading level. For grouped websites the FKGL ranged from high school senior to college reading level. This is significantly higher than the recommended level for patient health educating material (5th grade), 11 and even higher than previous studies.4,20 Although a previous study reported a higher FKGL in websites covering management of articular cartilage defects compared to those reported by foot and ankle studies, we found that websites on ankle OCL in particular have higher FKGL than the range listed in another study. 4 The mean FKGL for all websites was 11.82; higher than ranges reported in previous studies. 4
Although patient health literacy has been determined to be the most important indicator of health outcomes,23,24 the current poor quality and readability of the material may cause patient literacy to do more harm than good. This calls for improving the quality of the material available online by physicians specialized in the field. We believe that this could improve both patient literacy and patient-doctor interactions. This study provides pointers to improve certain aspects of the online OCL literature, and can guide new literature.
There were several limitation to this study. First, the websites were collected on one day limiting the sources to a specific day. Some of these links were no longer working by the time we started our analysis. In addition, the sources addressing osteoarthritis were filtered out, as this study focused on focal ankle OCL specifically. These sources, however, may be accessed by patients searching for focal ankle OCL and further contribute to the confusion (i.e., the actual quality of online material may be even poorer than what we determined it to be). By eliminating websites covering osteoarthritis most blogspots and other non–health care affiliated websites were eliminated. This may have contributed to the fewer number of non-healthcare affiliated websites in our study compared to other studies.4,9,10,14,20 The word “lesion” was avoided in our search terms as it is not commonly used by patients which may have yielded a less focused set of websites, slightly contributing to their poor quality. Last, commercial bias may have been at higher percentages than the reported one as website owners may be receiving financial compensation for mentioning certain treatments or emphasizing certain management plans.
Conclusion
The quality of the online sources on ankle OCL was proven to be poor by 3 different quality assessment tools and the readability tended to favor high school graduates/postgraduates. Even with that level of education, the poor quality of the material means that the information can be misinterpreted as well as misleading. In addition, more than half of websites did not distinguish between focal osteochondral defects and diffuse osteoarthritis. Our findings were in line with other studies reviewing different orthopedic topics. We hope that by highlighting the poor quality and readability of information on ankle OCL available online, physicians will be able to understand one possible source for their patients’ skepticism and confusion when discussing treatment plans. We expect that this article will provide an incentive as well as a guide to improve the quality and readability of online information on foot and ankle conditions in general and ankle OCL in particular.
Supplemental Material
sj-pdf-1-car-10.1177_19476035211021910 – Supplemental material for Evaluation of the Quality and Readability of Online Sources on the Diagnosis and Management of Osteochondral Lesions of the Ankle
Supplemental material, sj-pdf-1-car-10.1177_19476035211021910 for Evaluation of the Quality and Readability of Online Sources on the Diagnosis and Management of Osteochondral Lesions of the Ankle by Lamees Alshaikh, Yoshiharu Shimozono, John F. Dankert, Hugo Ubillus and John G. Kennedy in CARTILAGE
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: John G. Kennedy is a consultant for Arteriocyte, Inc.; received research support from the Ohnell Family Foundation, Mr. and Mrs. Michael J. Levitt. The other authors have no conflicts of interest to disclose.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.