
Abstract
Objective
After traumatic knee injuries, chondral fragments can avulse off bone with the progeny fragment becoming a loose body. The loose fragment may be larger than expected when trying to surgically repair the fragment back to its original site. The purpose of this study was to determine whether a loose chondral fragment from the lateral femur condyle would increase in size and weight after soaking in normal saline (NS) for 14 days.
Design
Twelve 6-mm OAT (osteoarticular transfer) plugs were harvested from 6 cadaver knees on the lateral femoral condyle to simulate a chondral fragment. The chondral fragments were then placed inside an airtight specimen container with NS (0.9% sodium chloride) and were measured over 14 days.
Results
After 14 days, the chondral fragments showed no increase in diameter as they measured an average of 5.567 ± 0.448 mm on Day 1 and 5.702 ± 0.253 mm on Day 14 (P = 0.183). The chondral fragments showed an increase in mass from an average of 0.058 ± 0.012 g on Day 1 to 0.073 ± 0.012 g on Day 14 (P < 0.001) and an increase in thickness from an average of 2.038 ± 0.346 mm on Day 1 to 2.229 ± 0.297 mm on Day 14 (P = 0.033).
Conclusions
Chondral fragments in NS increase in mass and thickness over time, but do not change in diameter. When surgeons are evaluating loose chondral fragments for fixation, they should consider that these fragments may appear thicker than the recipient location.
Introduction
After traumatic knee injuries, chondral fragments can avulse off bone with the progeny fragment becoming a loose body. The traumatic forces that create these either purely chondral or osteochondral loose bodies are often rotational or caused by an impaction force.1,2 In adolescents, an isolated traumatic patellar dislocation can result in significant deterioration of cartilage in the knee joint 3 and can potentially result in loose body formation.4,5 However, in adults, a chondral fracture is more commonly combined with other ligamentous or meniscal tears in the knee. 4 Loose bodies can also be formed by fractures in a joint space, osteochondritis dissecans, osteonecrosis, and osteoarthritis. 6 The longer the loose bodies remain in the joint, the more time they have to break into smaller pieces making them either more difficult to remove or repair. 4 Mobile loose bodies in the joint have the ability to cause internal derangement and can potentially lead to major damage of the surface of the joints and may lead to early osteoarthritis. 7 As purely cartilaginous bodies may be difficult to identify on plain x-ray, it has been found that magnetic resonance imaging (MRI) is the best non-invasive imaging for identifying loose chondral bodies in the knee joint.1,6,8
Methods
Specimen Preparation
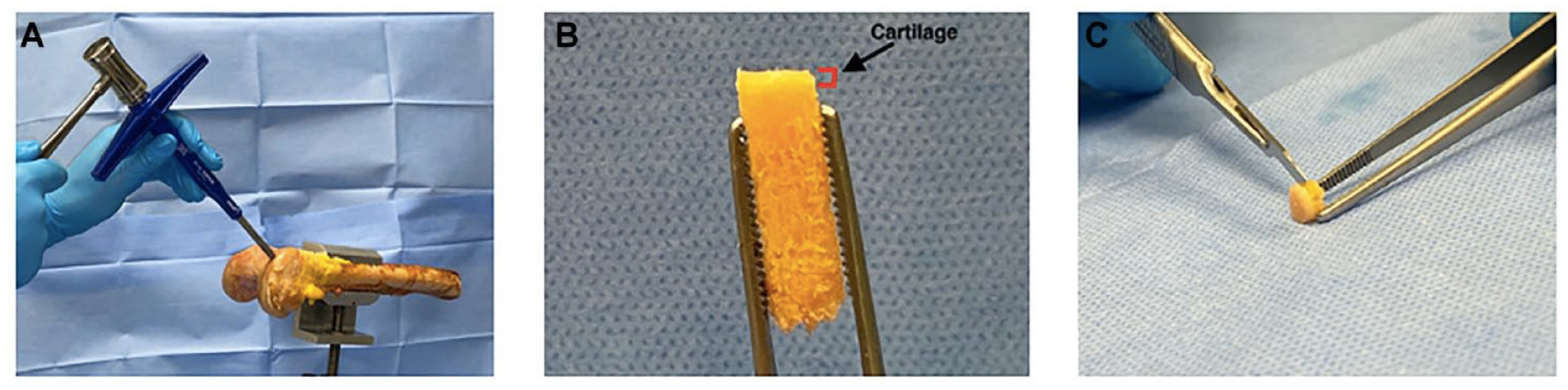
A Not Human Research Determination was made after project submission to the Institutional Review Board (IRB). Six femurs were harvested from 5 fresh frozen cadavers. After the knees were thawed over 24 hours, the distal femurs were isolated, and all soft tissue was removed. The femur shaft was placed into a vice to stabilize it and a 6-mm OAT (osteochondral autograft transplantation) harvester (Arthrex, Naples, FL) was used to obtain the samples from each femur ( Fig. 1A ). With a loose chondral fragment (secondary to patellar dislocation) being formed most commonly from the lateral femur condyle, all samples were taken from the lateral femur condyle.3,4,9 Two samples were taken from each lateral femur condyle, one anterior and one posterior from 6 cadaver knees, yielding 12 samples. The plugs were harvested to a depth of 12 mm ( Fig. 1B ). Knee traumas can often times lead to purely chondral loose bodies,2,4 so the bone was carefully removed from the cartilage with a rongeur and a 15 blade ( Fig. 1C ).
(
Fluid Simulation
Twelve 90 cc MediChoice Leakbuster specimen containers (Owens and Minor, Alpharetta, GA) were labeled with the femur sample and the location the plug would be harvested from and then filled with 50 cc of normal saline (NS; Braun Medical 0.9% sodium chloride). As most patellar dislocations that form loose bodies have some level of hemarthrosis, we chose 0.9% NS as an analog for a synovial fluid environment in the knee mixed with blood from a traumatic injury. Following patellar dislocations, there is often hemarthrosis. 10 While the osmolality of a hemarthrosis is poorly defined, the osmolality of blood serum is normally approximately 295 mOsm/kg, 11 and the osmolality of human knee synovial fluid has been found to be between 280 and 404 mOsm/kg. 12 The osmolality of 0.9% NS has been shown to be approximately 287 mOsm/kg. 13
Measurements
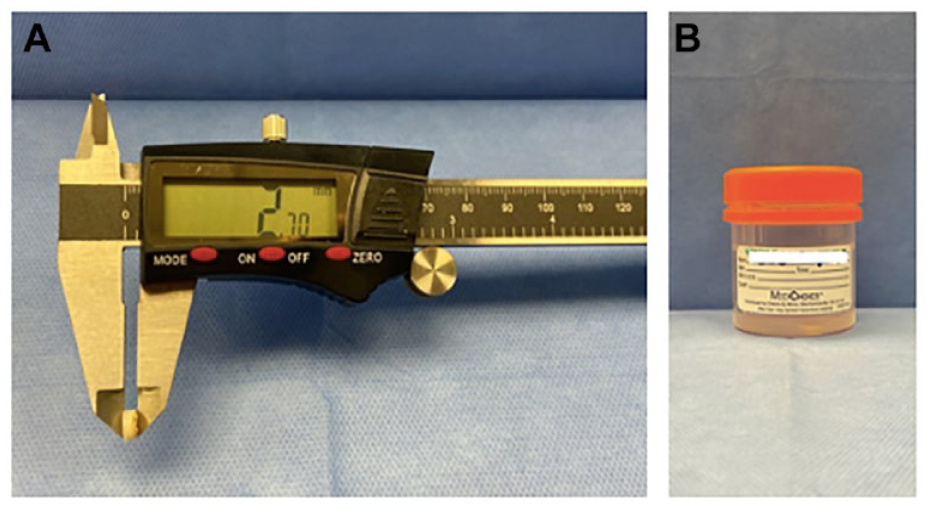
After removal of the bone, each plug was measured at baseline for diameter and thickness with a caliper (Husky 6 inch 3-Mode Digital Fractional Caliper, Atlanta, Georgia) ( Fig. 2A ) and mass was measured with a digital scale. As each plug was harvested using the same instrument with a circular cutout, the diameters of each sample were similar no matter what the orientation is. Each specimen was then placed into its corresponding cup of NS and closed for 24 hours. The following day, the plug was removed from its cup and dabbed dry to remove excess saline and then the following measurements were taken: diameter, thickness, and mass. The room was maintained at 20°C (68°F).
(
After the excess saline was removed from each chondral fragment, its diameter and thickness14-16 were measured with a caliper in millimeters. Its mass was then recorded to the hundredth of a gram using a digital scale. The chondral fragment was then placed back into its corresponding cup with an airtight seal ( Fig. 2B ). This process was repeated for over a total of 14 days with 10 days of measurement while recording all data. This was chosen because most loose bodies are attempted to be removed or fixed within 14 days after injury.4
Statistics
Numerical data comparing the thickness, diameter, and weight of the chondral fragments was analyzed with a Student 2-sample t test.
Results
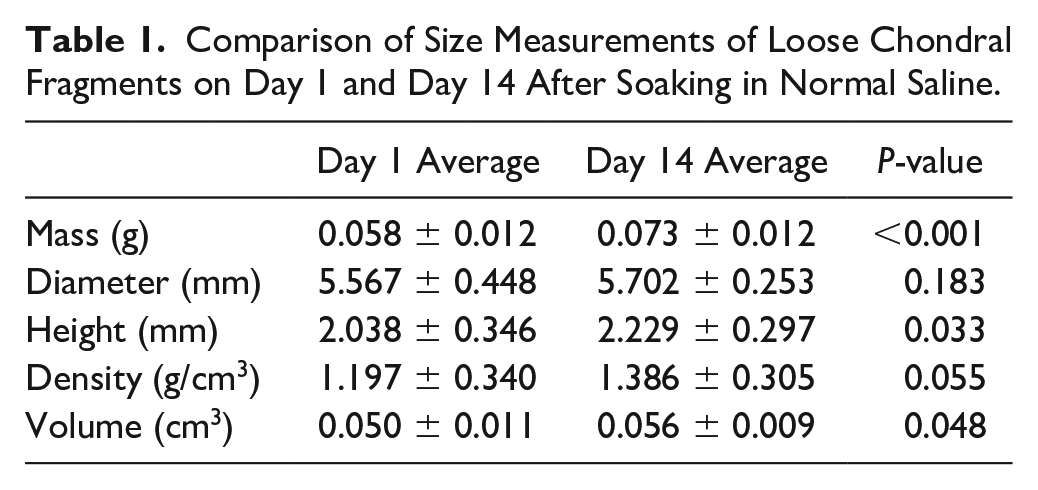
Twelve cartilage plugs were taken from 6 cadaver knees on the anterior and posterior lateral femoral condyle to simulate a chondral fragment. Based on available data, the average age of the cadaver knees was 82.2 years (SD = 6.9). Ten measurements were taken over 14 days. Measurements were taken on days 1 to 3, 6 to 10, and 13 to 14. After 14 days, the diameter of the chondral fragments showed no significant increase as they started on Day 1 at an average of 5.567 ± 0.448 mm and ended Day 14 at an average of 5.702 ± 0.253 mm (P = 0.183). After 14 days, the mass of the chondral fragments revealed a significant increase as they started on Day 1 at an average of 0.058 ± 0.012 g and ended Day 14 at an average of 0.073 ± 0.012 g (P < 0.01). After 14 days, the height (thickness) of the chondral fragments showed a significant increase as they started on Day 1 at an average of 2.038 ± 0.346 mm and ended Day 14 at an average of 2.229 ± 0.297 mm (P = 0.033). After 14 days, the density of the chondral fragments showed no significant increase as they started on Day 1 at an average of 1.197 ± 0.340 g/cm3 and ended Day 14 at an average of 1.386 ± 0.305 g/cm3 (P = 0.055). After 14 days, the volume of the chondral fragments showed a significant increase as they started on Day 1 at an average of 0.050 ± 0.011 cm3 and ended Day 14 at an average of 0.056 ± 0.009 cm3 (P = 0.048) ( Table 1 ).
Comparison of Size Measurements of Loose Chondral Fragments on Day 1 and Day 14 After Soaking in Normal Saline.
A subgroup analysis was performed to compare anterior versus posterior plugs at the 14-day mark. This demonstrated that there was no significant difference between anterior versus posterior with respect to mass, diameter, height, density, and volume (P = 0.16, 0.47, 0.21, 0.35, 0.49, respectively). A post hoc power analysis utilizing the measurements for mass at Day 1 and Day 14, with a sample size of 12 in each group demonstrated a 1 − β = .922.
Discussion
Although uncommon, isolated chondral fragments do occur and, according to recent literature, can be primarily fixed with good outcomes.14-16 Tanos et al. found that a twisting injury while playing sports was the most common cause of a purely chondral lesion in young adults/pediatric patients. They reported that surgeons used a variety of techniques to secure the chondral fragment to its original location including polydactine pins, cortical bone pegs, pushlock anchors, and bioabsorbable meniscus arrows. 15 Some surgeons also use chondral darts for fixation.15,16 Tisseel fibrin glue and 6-0 vicryl have been used as an adjunct to the previously mentioned techniques for additional stabilization. 15 The majority of these patients have been able to return to sports within 6 months to a year of surgery with little to no complications, leading to the current belief that purely chondral lesions can be fixed primarily with good outcomes.14,15,17
After patella dislocation, loose bodies can cause damage and should be urgently removed or repaired back to their parent region.4,18 Many authors have reported that these loose chondral fragments may need to be trimmed in order to get them to fit properly defect.4,6,19,20 It is also established that chondromatosis lesions may swell in the synovial fluid.6,21 While it may be that these loose fragments swell or change dimensions, after breaking free, this has not been previously evaluated. Our study sought to determine whether loose chondral fragments from the lateral femur increased in size or weight over time in NS as a surrogate for a hematoma-filled synovium. After 14 days of the chondral plugs being submerged in saline, we found that chondral fragments increase in mass and thickness.
In addition, we found a significant increase in volume but not density. Previous studies have shown the density of articular cartilage to be approximately 1.12 g/cm3. 22 Our study demonstrated an initial density of 1.197 which is comparable to previous studies. Another previous study reported the average cartilage thickness of the distal lateral femur condyle was 1.99 mm, while the posterior lateral condyle was 2.30. 23 This is comparable to our measurements of 2.038 mm for height or thickness. While the diameter of these chondral fragments does not appear to increase, the mass and thickness appear to increase resulting in an increase in volume.
It has been shown that the viability of cartilage on loose bodies is comparable to the viability of the intact native cartilage on the articular surface.18,24 Saotome et al. found that loose bodies from synovial chondromatosis can enlarge due to growth of chondrocytes. 21 Attarian and Guilak 25 were able to follow a patient refusing surgery for 11 years and found that 2 loose bodies in his knee had nearly doubled in size since his initial presentation. While loose bodies are capable of growth after long periods due to chondrocyte growth, there is also an element of swelling that is involved. Our study focused on the swelling of the cartilage after traumatic dislocation due to the fact that it is recommended to remove or repair the fragment as soon as possible.
Articular cartilage can typically be divided into 4 layers or zones.26,27 The first and thinnest is the superficial (tangential) zone, then the middle (transitional) zone, the deep zone, and finally the calcified zone that serves as an anchor to the subchondral bone (with hydroxyapatite crystals). 27 Regarding damage to the cartilage and its layers, there can either be partial thickness defects, where there is no access to the progenitor cells in the subchondral bone and therefore no spontaneous healing, or full thickness defects which have a potential to repair itself with a fibrocartilaginous tissue. 28 Because of its avascular nature, articular cartilage must receive the raw materials it needs through its surrounding environment, most notably the synovial fluid.
Synovial fluid in joint spaces not only acts as a lubricant for articular cartilage but also as a source of nutrients for some of its surrounding structures which they receive through diffusion. It is constantly circulating with the help of joint movement, the lymphatic system, and small capillaries. 29 The cartilage can imbibe synovial fluid and is thought to be nourished by metabolites coming to and from the synovial fluid moving by diffusion or mechanical force. 30 It also functions to transport waste products and other enzymes or metabolites. 31 It is commonly believed to be an ultrafiltrate created from blood plasma passing through the synovial membrane.29,31 Type-B synovial cells within the joint are able to produce hyaluronan (hyaluronic acid) which can create a complex with the proteins in the synovial fluid which acts as one of the major lubricants (contains 3-4 mg/mL of HA 31 ). 32 Synovial fluid also contains proteinases, collagenases, and one other lubricant known as lubricin (or PRG4) that is created by fibroblasts in the synovium. 33 The synovial fluid also contains growth factors and cytokines that are important in regulating the populations of cells in the joint and fluid. Compared with whole blood, there are relatively few cells (leukocytes) in the synovial fluid. 34 Any change in this homeostasis of transport and lubrication can lead to diseases such as rheumatoid arthritis or osteoarthritis causing joint destruction. 31
As discussed above, chondral fragments can become loose bodies in the knee joint after a traumatic event. These fragments have the potential to cause damage to the joint itself including the cartilage, synovial lining, or bursa and therefore need to be either removed completely or fixed back into its proper position. 4 Although some sources say there is no biologically beneficial effect shown after debridement and loose body removal, 35 there is at least an improvement in pain following the surgery. 36 If an injury is severe enough to cause a loose body in the joint, the majority of surgeons would recommend fixation of the loose fragment if there is enough healthy subchondral bone.37,38 Fixation of the loose body can be done in many different ways, and it is up to the surgeon to determine which method is appropriate depending on the size and location of fragment. While there is no definite time frame for fixation, it is usually better to address fractures of any sort as quickly as possible. According to one study by Siparsky et al., 4 if done within 2 weeks of the traumatic knee injury, a purely chondral fragment can be successfully repaired back in place using absorbable sutures, biologic adhesives, or chondral darts—especially in adolescents but also in adults. One traumatic event that can result in mostly or purely chondral fragments is patellar dislocations. This can occur in children and adults and fixation of the fragment is often performed. In 2005, Nikku et al. looked at operative versus non-operative treatments in 127 patients with a primary patellar dislocation. They determined that patient outcomes, both self-reported and functional, were lowered if a loose body was seen on imaging. 39 In another study, it was shown that after patellar dislocation with loose body formation, internal fixation of the mostly chondral fragments in the knee joint with bioabsorbable polyglycolic acid rods to the lateral condyle is an option and have shown positive outcomes in adolescents. 9 In a similar study, Nakamura et al. 19 showed that complete healing of a chondral fragment could be expected in an adolescent when repaired with bioabsorbable pins. Because of articular cartilage’s unique, complex composition acting along with internal hydrostatic pressures, it displays a novel swelling ability.40,41 Depending on its shape, it has even been noted to curl at a higher swelling pressure. 42 This swelling pressure is partly the cause of its unique ability to withstand such strong forces and compression.43,44 It is believed to be the interaction between the sulfated glycosaminoglycan (sGAG) (negatively charged) and the interstitial fluid inside the cartilage structure that creates this swelling pressure. 45 It has been shown that the higher the level of glycosaminoglycan compared with collagen, the greater the increase in swelling of cartilage.46,47 Brown et al. showed how important the structural composition of cartilage is and how it can influence swelling. They determined with cartilage strips that with a disruption in the most superficial zone of the cartilage and a disruption in the structure of the tissue matrix and collagen (to simulate trauma/wear), the swelling is greater than a structurally intact and healthy cartilage strip. 48 Summers et al. 49 found that when not protected by surrounding healthy cartilage and/or subchondral bone, a sample of cartilage in phosphate-buffered saline has the potential to increase in hydration by 6% on average. Decreased levels of sGAG in cartilage (simulating progression of arthritis) result in a reduced swelling stress acting in the cartilage.50,51 After a trauma creating a loose body in a joint, lower levels of cartilage that are not typically exposed are now in contact with a direct source of synovial fluid. Because the deeper levels of cartilage contain progressively more sGAG, 40 it could be that they are able to swell more and create a larger fragment than was originally made.
Limitations
We recognize that this experiment has some limitations. First, it is limited by the use of NS in the place of actual synovial fluid. While we have explained above how NS would be a similar osmolality to synovial fluid mixed with blood after a traumatic injury, there is no replacement for real synovial fluid. Further experiments could be completed with a closer match to physiological synovial fluid to better simulate a real patient. Another limitation is the stagnant nature of the NS that the chondral fragments were sitting in. Synovial fluid is continuously being renewed in joints and would possibly provide even more nutrition for chondral fragments to grow over time. Potential experiments could be done to simulate this constant turnover of fluid. The quality of articular cartilage has been shown to decrease with age. 52 This study was limited by the use of articular cartilage from an older population than would be expected to experience a traumatic injury of this sort. Although digital calipers have been shown to produce similar measurements of soft structures when compared with advanced methods of measurement, measurements done with the digital caliper could have been influenced by compressive factors 53 and a non-contact measurement could resolve this potential issue. Proteoglycan loss over the course of the experiment could have influenced the swelling seen, as no physical constraints or enzymatic inhibitors were utilized. The average age of our cadaver specimens is also a limitation of the study. The quality of articular cartilage has been shown to decrease with age. 54 Further studies with younger cadaver tissue are encouraged. The final limitation was that we were not able to have consecutive days of measurements. Due to personnel constraints, Days 4 and 5 and 11 and 12 were not measured. While there were not 14 fully consecutive days measured, we were still able to measure the primary endpoint of the study.
Supplemental Material
sj-docx-1-car-10.1177_19476035231206258 – Supplemental material for In Vitro Evaluation of Lateral Femur Condyle Free Chondral Fragment Swelling after Soaking in Normal Saline
Supplemental material, sj-docx-1-car-10.1177_19476035231206258 for In Vitro Evaluation of Lateral Femur Condyle Free Chondral Fragment Swelling after Soaking in Normal Saline by Carver Montgomery, Wayne Scalisi, James Robinson, William Sherman, Giovanni F. Solitro and Patrick Massey in CARTILAGE
Footnotes
Acknowledgements
The authors thank Baraa Shihadeh for manuscript preparation and Ki’avian Johnson for data collection. The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for this study was waived by the Louisiana State University Health Sciences Center’s Institutional Review Board in Shreveport, LA because it was determined to be research not involving human subjects.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.