
Abstract
Objective
To assess the economic burden of moderate to severe osteoarthritis (OA) management for patients and the health care system in Greece.
Design
A noninterventional, cross-sectional, prospective, epidemiological analysis of data from the medical records of patients with moderate to severe OA, recruited in a single visit from 9 sites in Greece. Outcomes included health care resource use (direct/indirect costs) associated with this patient population.
Results
A total of 164 patients were included in the analysis: mean age was 70.5 years, and the majority of participants were females (78.7%). The presence of comorbidities was reported by 87.2% of patients, with hypertension being the most frequently reported (53.7%). Paracetamol was the most commonly used analgesic treatment (96%), followed by systemic nonsteroidal anti-inflammatory drugs (NSAIDs) (75%) and opioids (50%). The mean overall annual direct costs per patient was estimated at 1,675.3€, with approximately half incurred by the National Health Insurance Fund, whereas the mean overall annual indirect cost (absenteeism of patients and informal caregivers) was estimated at 3,501.4€. Joint replacement (JR) procedures and paid care were the major drivers of annual direct costs in this patient population (4,326.3€ and 9,360.0€, respectively).
Conclusions
This real-world analysis of direct and indirect costs confirmed the substantial economic burden imposed by moderate to severe OA to the health care system and the patients. Our findings emphasize the need for interventions to enhance disease management, to improve patients’ health outcomes and reduce the global burden of OA on society.
Introduction
Osteoarthritis (OA) is a chronic multifactorial condition that has been associated with a number of specific risk factors (i.e., obesity, advanced age, and female gender)1 -3 and concurrent comorbid conditions (i.e., stroke, hypertension, peptic ulcer, anxiety, depression, diabetes, and obesity),4 -7 thus increasing both the complexity of disease management and the cost of treatment.3,8,9 Considering the increasing prevalence of adult obesity recorded over the past decades, in conjunction with the aging of population, concerns are raised over the burden of the disease in the future.2,10,11
Indeed, the prevalence of OA increased globally by 113.25%, from 247.51 million in 1990 to 527.81 million in 2019. 12 Accordingly, global trends demonstrated a 114.5% increase in years lived with disability (YLD) due to OA from 1990 to 2019.12,13 OA in large joints (i.e., knee and hip) is considered to cause the largest disability due to joint replacement (JR) at end-stage disease, 12 with knee OA accounting for approximately 85% of the disease burden worldwide. 14
Despite a number of available treatment options and guidelines for the management of pain associated with OA, patients continue to suffer from chronic pain, leading to physical inactivity, loss of autonomy, social distancing, and compromised quality of life (QoL).2,15 The resulting economic burden in terms of both direct and indirect health care cost is significant for both patients and health insurance organizations. Most of the direct costs of OA are usually attributed to JR surgery, with smaller proportions accounted for pharmacological and nonpharmacological treatment, side effects from treatment, physician visits, and diagnostic procedures (i.e., X-rays, magnetic resonance imaging [MRIs]). On the contrary, indirect costs are mainly attributed to productivity losses from absenteeism (sick leave), as well as presenteeism (decreased productivity because of pain), care-giver time, disability compensation/benefits, early retirement, and premature mortality.2,8,9,16 In particular, in several European countries, OA has been associated with annual direct and indirect costs of up to €7.2 and €4.6 billion respectively2,3,8,17 -22 corresponding to 0.25% to 0.5% of a country’s gross domestic product (GDP). 23
In Greece, there is a knowledge gap regarding the economic burden of the disease on the health care system in a real-world setting. The aim of our analysis was to estimate the annual direct and indirect costs within a Greek population with confirmed, moderate to severe OA, which is resistant to, cannot tolerate, or is ineligible for paracetamol and/or nonsteroidal anti-inflammatory drugs (NSAIDs) and/or opioids.
Methods
Ethics Statement
The study protocol and informed consent documentation were approved by the Institutional Review Boards at all participating sites.
Design and Study Population
The PONOS study (A4091091) was a noninterventional (NI), cross-sectional, epidemiological, primary data collection study to assess the burden of moderate to severe hip/knee OA management on the health care system.
Patients ≥18 years of age with confirmed and symptomatic hip or knee OA, of moderate to severe grade on radiographic examination (Kellgren-Lawrence [KL] grade 3-4), for whom treatment with paracetamol and/or NSAIDs and/or an opioid was ineffective, not tolerated or inappropriate were recruited in a single visit between 29 April 2021 and 30 November 2021 from 9 hospital outpatient departments/hospital clinics in Greece, after written informed consent was obtained by the enrolling physician.
Assessments
The following variables were retrieved from the medical records of each patient: demographic data, clinical characteristics, comorbidities, medications, and health care resource (HCR) use (direct and indirect costs). Short recall periods were used to reduce reporting bias.
HCR Use
HCR use was estimated as direct and indirect cost. An algorithm was used to sum the products of each variable and concluded to an aggregated estimate of both direct and indirect HCR use associated with this patient population in Greece. The algorithms for direct and indirect cost are provided in the Supplementary material.
Direct Cost
Direct cost included health care professionals (HCPs) visits for OA, medications, diagnostic tests (i.e., X-rays, MRIs, others), emergency visits, JR procedures, hospitalizations for JR, rehabilitation (physiotherapy), psychotherapy, paid care, and additional equipment. In Greece, prescription medications and diagnostic tests for insured patients are reimbursed by the national health insurance fund (National Organization for the Provision of Health Services/NOPHS) and patients shoulder a 25% co-payment for most medications (or 0% for life-threatening diseases and 10% for specific chronic diseases) and diagnostic tests. 24 Cost coverage was split depending on the source of payment (NOPHS, private contribution or both [co-payment]) to calculate overall cost and NOPHS-attributed cost separately. Costs of hospital admissions for the index hospitalization were calculated based on the Greek Diagnosis-Related Groups (DRGs).
Indirect Costs
Indirect costs included productivity losses from absenteeism (sick leave) of patients and informal caregivers (i.e., relatives and friends). In this study, productivity losses were estimated based on patient reports using the human capital approach (HCA), which considers forgone earnings due to OA as productivity losses and is the most commonly used method for the evaluation of indirect costs.25,26 Detailed information on cost estimation is provided in the Supplementary material.
Statistical Analysis
As this was an NI study, the results of the data analyses (overall and by index joint) are presented using descriptive statistics. The analysis did not involve any group comparisons or inferences and was not adjusted for any potential confounders.
Descriptive statistics for continuous variables are presented for annual direct and indirect costs. For the variables of the indirect cost and the direct cost where applicable, the 3-month reported periods were extrapolated to 12 months. Furthermore, for all categories of direct costs, NOPHS-attributed costs were calculated.
Statistical analysis and generation of all tables were performed using RStudio (RStudio Team (2020)). RStudio (Integrated Development for R. RStudio, PBC, Boston, MA) and/or IBM SPSS v.25 (IBM Corp. Released 2017. IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp.).
Results
Patients’ Characteristics
The characteristics of patients in the overall study population and in the hip and knee OA subpopulations are summarized in
Patients’ Demographic Characteristics.
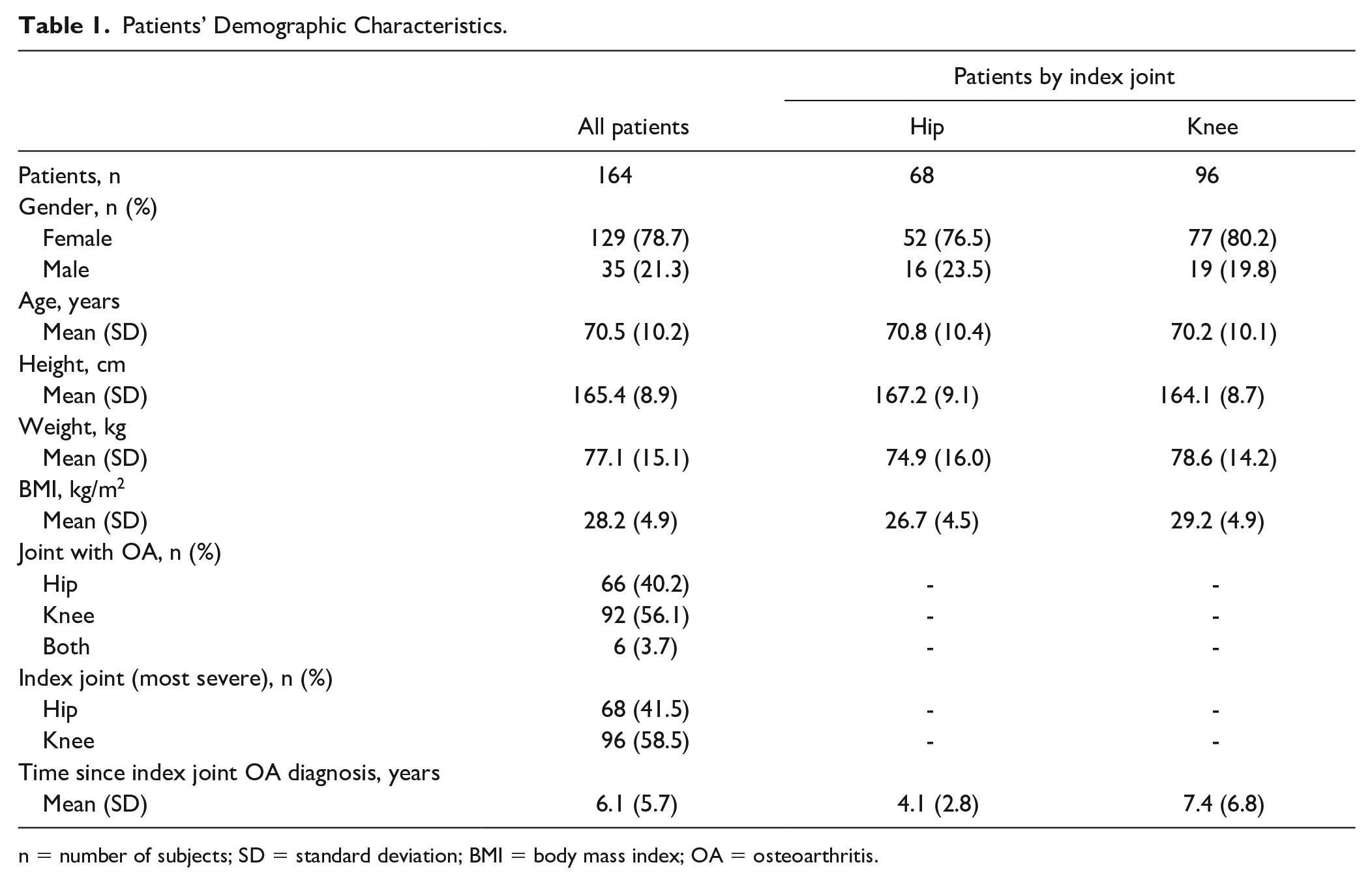
n = number of subjects; SD = standard deviation; BMI = body mass index; OA = osteoarthritis.
Most Frequent Comorbidities and Medications.
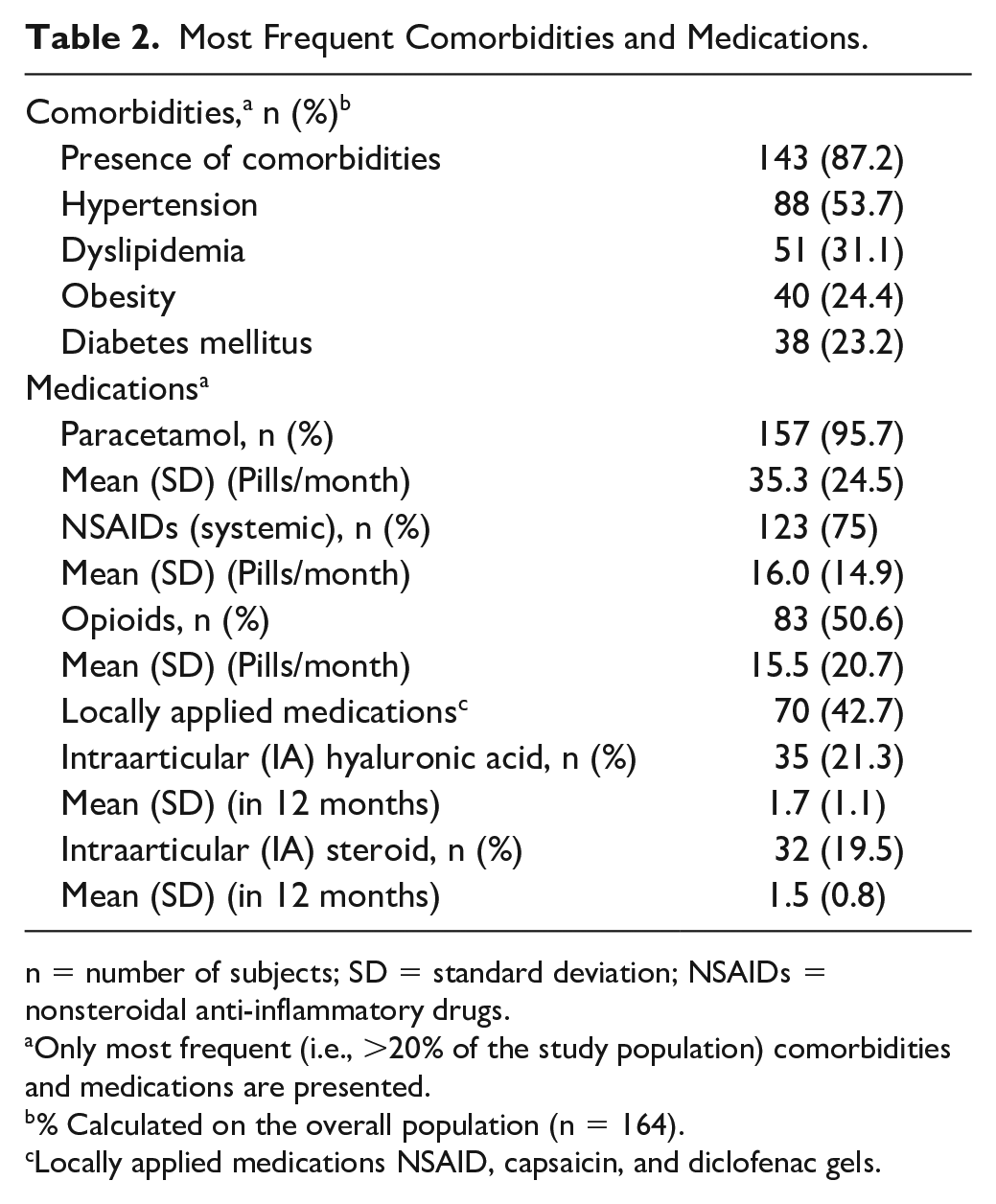
n = number of subjects; SD = standard deviation; NSAIDs = nonsteroidal anti-inflammatory drugs.
Only most frequent (i.e., >20% of the study population) comorbidities and medications are presented.
% Calculated on the overall population (n = 164).
Locally applied medications NSAID, capsaicin, and diclofenac gels.
A total of 164 patients were enrolled in the PONOS study between 29 April 2021 and 30 November 2021 from 9 hospital outpatient departments/hospital clinics in Greece. The majority of patients were females (129/164; 78.7%), mean (SD) age was 70.5 (10.2) years; mean (SD) body mass index (BMI) was 28.2 (4.9) kg/m2, classified as “overweight.” Knee, hip OA or OA of both joints (hip and knee) was reported by 56.1% (92/164), 40.2% (66/164), and 3.7% (6/164) of patients, respectively. The knee was indicated as the index joint, that is, the joint with the most severe OA in 96 out of 164 patients (58.5%) and the hip was the index joint for the remaining 68 patients (41.5%). The mean (SD) time since OA diagnosis of the index joint was 6.1 (5.7) years. Both types of OA were more prevalent in females, with 76.5% (52/68) and 80.2% (77/96) of women suffering from hip OA and knee OA, respectively ( Table 1 ).
Presence of comorbidities was reported by the majority of patients (143/164; 87.2%), with hypertension being the most frequently reported (88/164; 53.7%), followed by dyslipidaemia (51/164; 31.1%), obesity (40/164; 24.4%) and diabetes mellitus (38/164; 23.2%) ( Table 2 ).
Paracetamol was the most commonly used analgesic treatment (96%), followed by NSAIDs (systemic) (75%), opioids (50%), locally applied medications (NSAID, capsaicin and diclofenac gels) (42.7%) and intraarticular (IA) (steroid or hyaluronic acid) injections (41%). Patients in the overall study population reported a consumption of a mean (SD) of 35.3 (24.5), 16.0 (14.9) and 15.5 (20.7) pills/month of paracetamol, NSAIDs (systemic) and opioids, respectively ( Table 2 ).
HCR Use
Direct
Over the 12 months prior to study enrollment, most patients (151/164; 92%) had visited HCPs for their OA with a mean (SD) of 2.3 (1.5) visits. Regarding diagnostic tests performed for OA during the same period, 94.5% of patients (155/164) had an X-ray and 24.4% (40/164) had an MRI. These tests were covered by NOPHS in 113 patients (71.5%). The mean (SD) number of X-rays and MRIs performed was 2.3 (1.7) and 1.1 (0.3) respectively ( Table 3 ).
Health Care Resource Use.
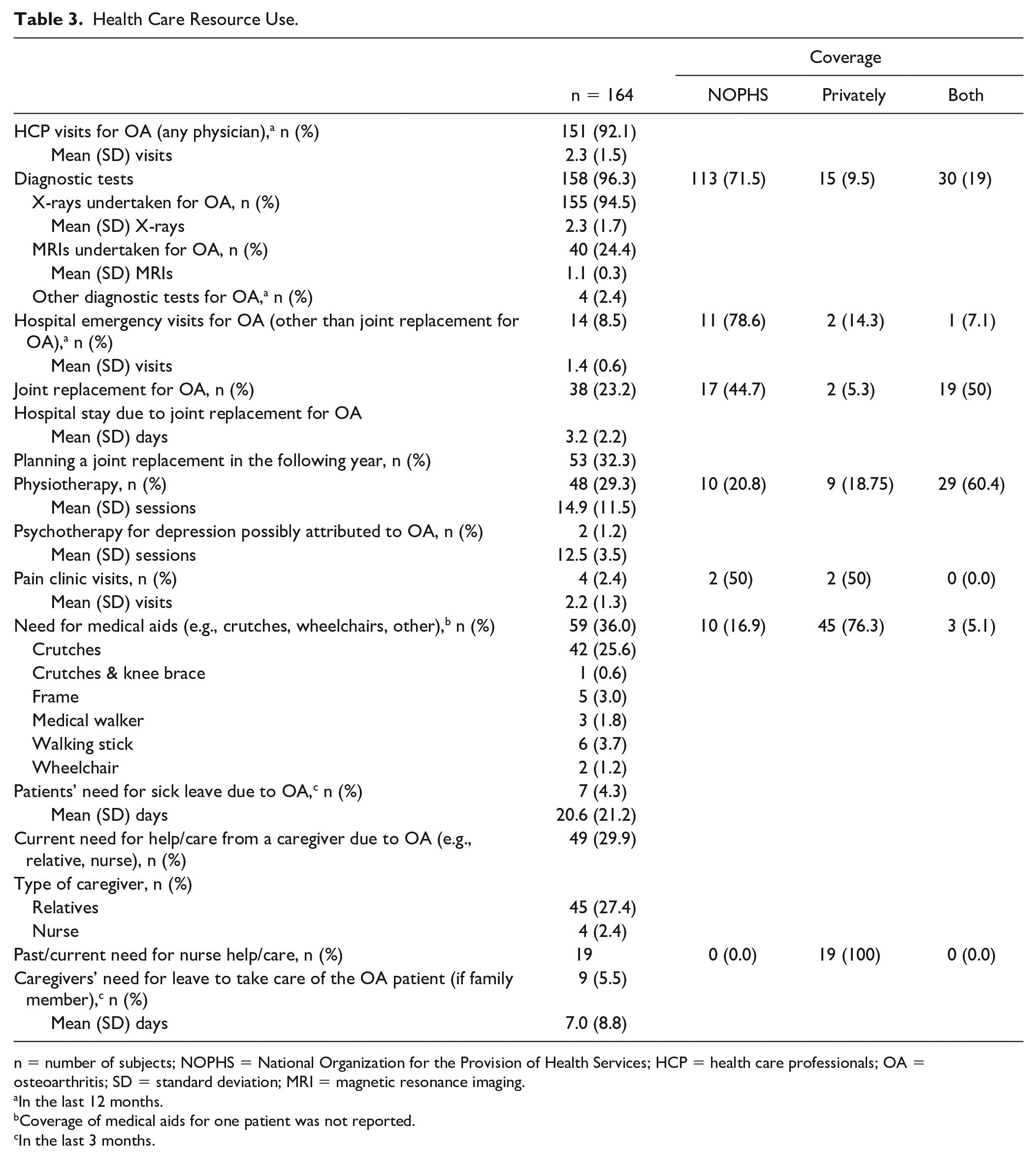
n = number of subjects; NOPHS = National Organization for the Provision of Health Services; HCP = health care professionals; OA = osteoarthritis; SD = standard deviation; MRI = magnetic resonance imaging.
In the last 12 months.
Coverage of medical aids for one patient was not reported.
In the last 3 months.
Furthermore, 14 out of 164 patients (8.5%) had hospital emergency visits for OA (other than JR) with a mean (SD) of 1.4 (0.6) visits. Emergency visits were covered by NOPHS in 11 patients (78.6%) and by both the NOPHS and privately in 1 patient (7.1%). Thirty-eight out of 164 patients (23.2%) underwent JR for OA and 53 out of 164 patients (32.3%) were planning to have the procedure within the following year. The procedure was covered both by NOPHS and privately for 19 patients (50%) and only by NOPHS for 17 patients (44.7%). Patients spent a mean (SD) of 3.2 (2.2) days in the hospital due to JR ( Table 3 ).
Forty-eight out of 164 patients (29.3%) had physiotherapy during the last 12 months that was covered by both the NOPHS and privately in 29 patients (60.4%) and only by NOPHS in 10 patients (20.8%). The mean (SD) number of physiotherapies performed was 14.9 (11.5) ( Table 3 ).
The use of medical aids was reported in 59 out of 164 patients (36.0%), which was covered by NOPHS in 10 patients (17.2%) and by both the NOPHS and privately in 3 patients (5.2%). Crutches were the most commonly used medical aid (42/164; 25.6%) among the OA patient population ( Table 3 ).
Indirect
Need for sick leave due to OA was reported by 7 out of 164 patients (4.3%) in the last 3 months, with a mean (SD) number of days on leave of 20.6 ( Table 3 ).
Forty-nine out of 164 patients (29.9%) needed help/care from a caregiver (e.g., relative, nurse) due to OA, with relatives being the most frequent caregivers (45 patients; 27.4% of the total study population). No need for leave by their caregivers was reported by 40 patients (24.4% of the total study population), while 9 patients (5.5% of the total study population) reported need for leave by their caregivers. The mean (SD) number of days on leave was 7.0 (8.8) days. In cases that nurse support was needed, 19 patients (100%) reported that the cost was covered privately ( Table 3 ).
Costs
Direct Costs
Annual direct costs
The mean (SD) overall annual direct costs for each patient within the total study population and within the hip OA and knee OA subpopulations within the year prior to enrollment were estimated at 1,675.3 (2,518.2), 2,282.1 (2,770.8), and 1,245.6 (2,239.5) Euros, respectively ( Table 4 ).
Annual Direct Costs (Overall and by Component) (in €).
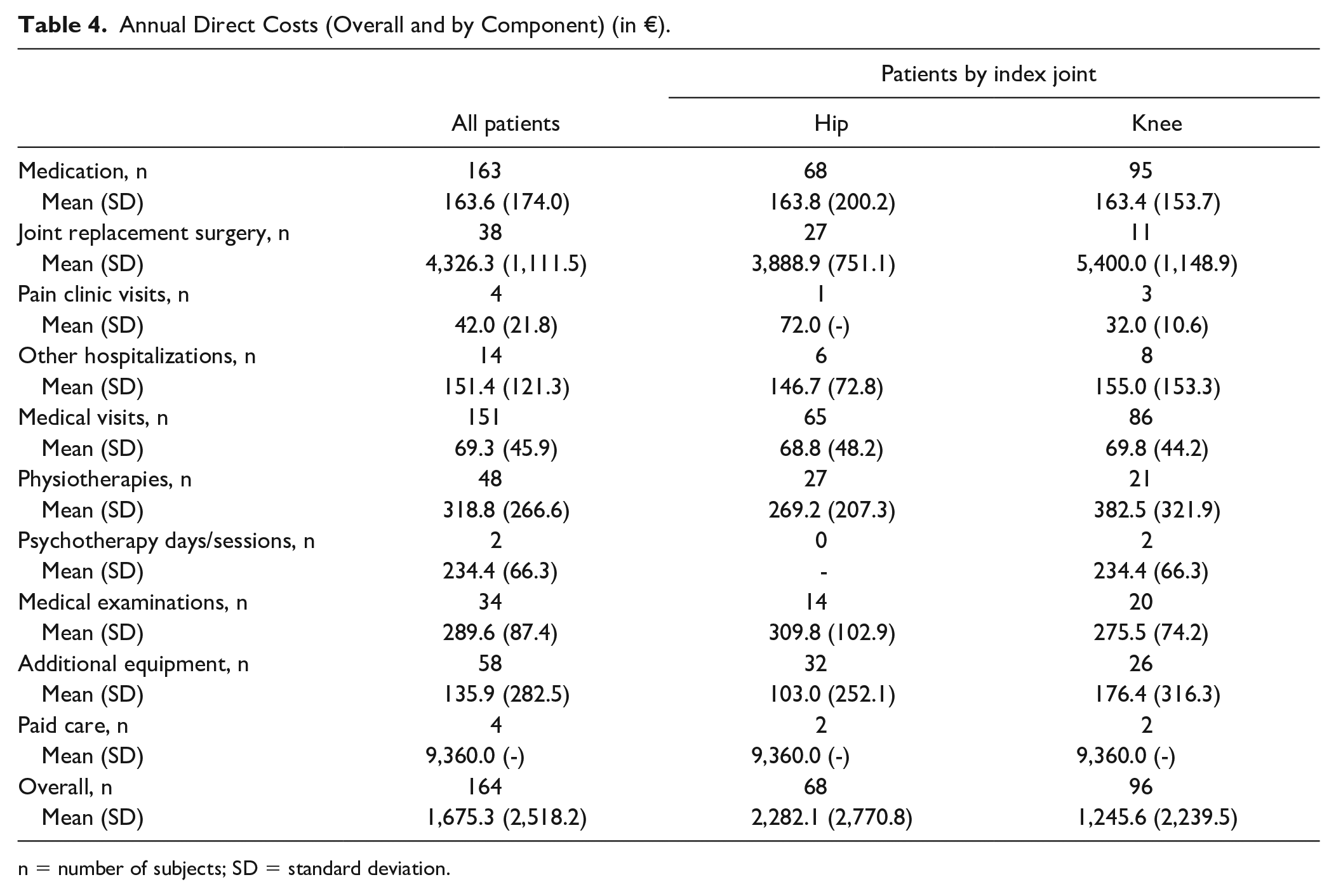
n = number of subjects; SD = standard deviation.
In addition, the mean (SD) annual direct cost per patient for JR surgery was estimated at 4,326.3 (1,111.5) Euros (reported by 38 out of 164 patients), 3,888.9 (751.1) Euros (reported by 27 out of 68 patients), and 5,400.0 (1,148.9) Euros (reported by 11 out of 96 patients) within the total study population and within the hip OA and knee OA subpopulations, respectively. The mean (SD) annual direct cost for paid care in the total study population and the hip and knee OA subpopulations was estimated at 9,360.0 (-) Euros ( Table 4 ).
Annual direct NOPHS-attributed costs
As indicated in Table 5 , the mean (SD) overall annual direct NOPHS-attributed costs per patient in the total study population, as well as within the hip OA and knee OA subpopulations during the year prior to enrollment were estimated at 813.4 (1,289.0), 1,112.4 (1,296.3), and 601.7 (1,247.6) Euros, respectively.
Annual direct NOPHS-Attributed Costs (Overall and by Component) (in €).
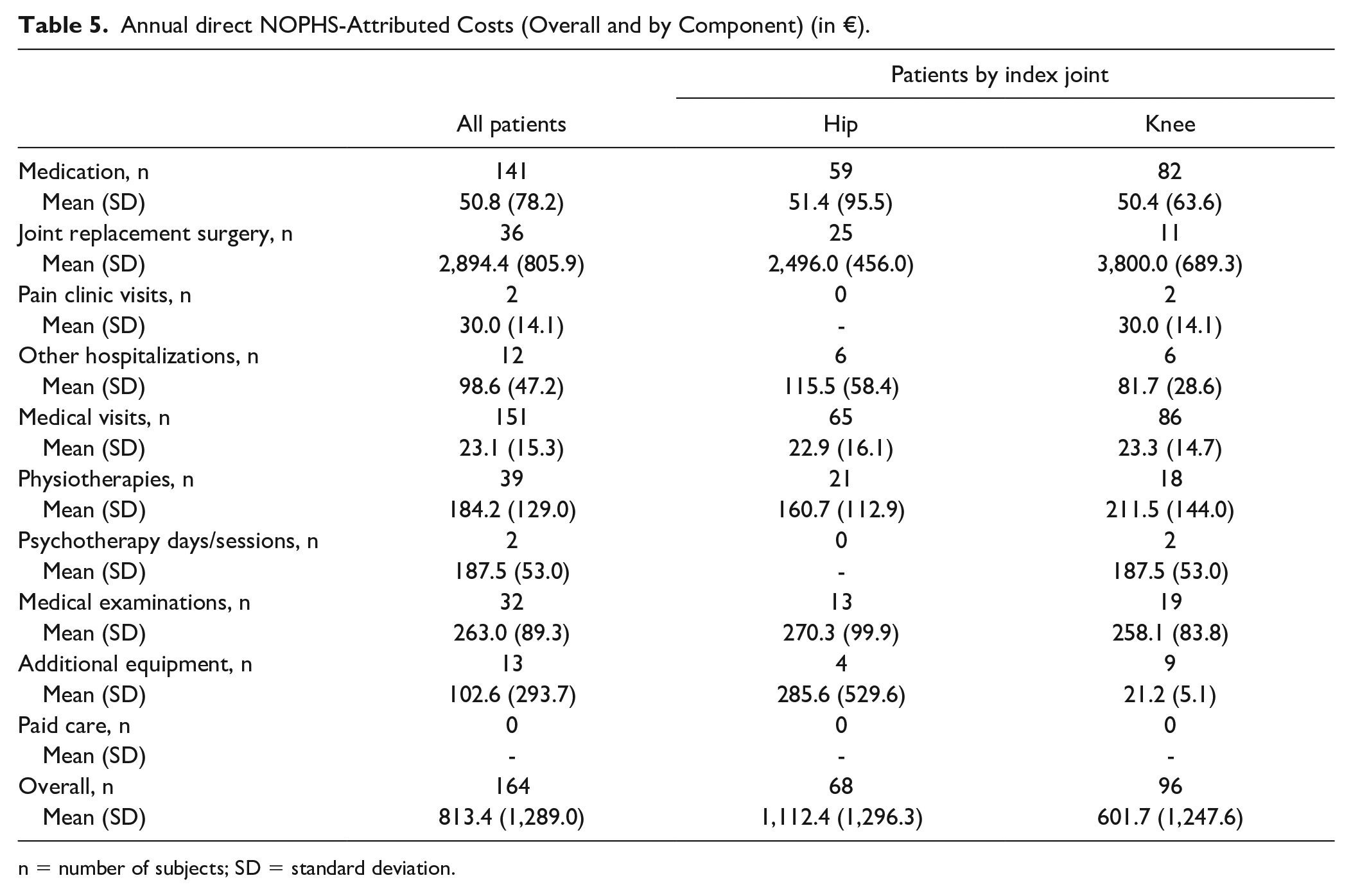
n = number of subjects; SD = standard deviation.
Indirect Costs
The mean (SD) overall annual indirect costs due to productivity loss (absenteeism) of both OA patients (N = 7) and their informal caregivers (N = 9) within the year prior to enrollment were estimated at 3,501.4 (4,439.9) Euros for the total study population and at 3,985.8 (4,962.5) and 2,435.8 (3,208.0) Euros for the hip OA and knee OA subpopulations, respectively ( Table 6 ).
Annual Indirect Costs (Overall and by Component) (in €).
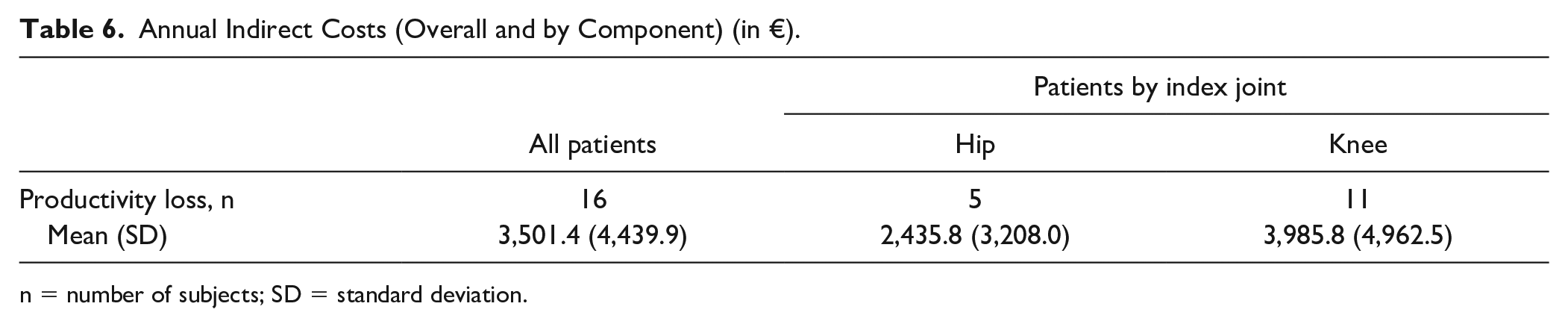
n = number of subjects; SD = standard deviation.
Discussion
The PONOS study is the first observational study designed to assess the economic burden of moderate to severe hip/knee OA management for the health care system and patients in Greece, assessed as either direct or indirect HCR use. Undoubtedly, OA imposes a substantial economic burden on patients, health care providers, governments, and the society as a whole, resulting from functional impairment, psychological burden, comorbid diseases, and increased HCR utilization.3,9 Studies reporting OA costs for a number of Western European countries estimated annual direct costs between 497€ and 1,800€ (or from €0.2bn to €7.2bn at a national level) and indirect costs between 200€ and 8,350€ (or from €0.2bn to €4.6bn at a national level).17 -22 OA management has been therefore related to costs corresponding to 0.25% to 0.5% of a country’s GDP. 23 The findings of this study confirmed the high economic burden of OA in Greece with annual direct and indirect costs per patient with moderate to severe OA estimated at 1,675.3 € and 3,501.4 €, respectively. Overall, in this patient population with moderate to severe OA, JR procedure (reported by 38 patients) and paid care (reported by 4 patients) were the major drivers of costs, with substantially high annual direct costs per patient (4,326.3€ and 9,360.0€, respectively).
Costs for JR surgery were found to be in line with the estimated cost of hip and knee replacement across European Union (EU) countries (5,600€-5,700€). 28 Significant advances in surgical treatments have provided effective options for OA patients that have not responded to conservative treatments for the reduction of pain and functional disability. Importantly, the number of hip and knee replacement procedures has increased in recent years in most European countries, contributing to health expenditure growth, since these are quite expensive interventions. More specifically, in the EU, the rates of hip and knee replacement were 189 and 130 per 100,000 population, respectively, whereas in Greece, the rate of hip replacement were 163 per 100,000 population, and there were no records regarding knee replacement. 28 Generally, rates of hip and knee replacement vary between countries, without reflecting the prevalence of OA, most likely due to lack of internationally agreed and adopted criteria for selecting individuals for joint surgery, resulting in variable waiting times.29,30 The average waiting times for hip and knee replacement have been reported to be around 40 days in the Netherlands, but around 150 days in Hungary, Spain, and Norway, and over 365 days in Poland. 28 In this study, it was noted that within this challenging population suffering from chronic pain and having no further pharmacological options, nearly 30% of the cohort had neither performed JR surgery nor planned one in the following year. This finding could perhaps be explained by the long waiting times for surgery in Greece, highlighting the need for better disease management and treatment options that could timely offer pain relief in moderate to severe OA patients. In this direction, it is noteworthy that several countries have adopted policy tools by setting waiting time standards in an effort to reduce long waiting times. This has been the case in Finland 31 and England. 32
The results of this analysis also emphasizes the considerably high economic burden imposed on the Greek national health insurance fund (NOPHS), with the average annual direct costs being incurred by the NOPHS estimated at 813.4€. More specifically, the annual NOPHS contribution per patient was estimated at 2,894.4€ for JR procedures, 263.0€ for medical examinations, 184.2€ for physiotherapies sessions and 102.6€ for additional equipment. OA patients are also affected by high health care costs, mainly attributed to paid care because these costs are covered entirely by private contribution. The overall impact of the need for care for moderate to severe OA patients may be underestimated since patients in Greece are commonly taken care by family members due to strong family bonds and extended households. This was highlighted in our study in which among the 49 patients in need for help/care, 45 patients received care by family members, and only 4 patients received paid care.
Our results also confirmed the considerable impact of OA on work productivity, with mean annual indirect costs estimated at 3,501.4€ for the total study population and at 2,435.8€ and 3,985.8€ for the hip OA and knee OA subpopulations, respectively. The mean number of days on leave in the last 3 months was 20.6 days, accounting for 82.4 sick leave days per year. A recently conducted study in the Netherlands using data from administrative databases reported an annual average sick leave duration of 186 and 159 days for knee and hip OA patients, respectively, 33 whereas another study from the same setting using self-reported sick leave found 0.8 sick days per knee OA patient per month, accounting for 9.6 sick leave days per year. 34 Productivity loss was also examined in OA patients with self-reported disease from five European countries (France, Germany, Italy, Spain and the United Kingdom), with approximately one-third of them being employed. They have reported approximately 7% absenteeism (percentage of work missed), whereas the rates of presenteeism (percentage of overall work impairment due to OA) were almost four times greater than absenteeism, with an average of 24%. 35 These variations might reflect differences in disease severity of OA workers, methods for reporting sick-leave (i.e., administrative databases, self-report),33,34 as well as differences in social security systems and labor legislation between countries. 36
It is widely accepted that the actual costs remain challenging to measure—especially prospectively—because of differences in OA severity, accompanied comorbid conditions, treatment, and health care systems, as well as in methods for cost estimates and this is reflected in the variation of OA costs found among different studies. It is also acknowledged that indirect costs represent a largely underestimated economic burden, with some evidence suggesting they could be even up to 4 times as high as direct costs and therefore, these estimates may just be the tip of the iceberg.8,9,23
The limitations of this study were mainly related to its NI nature that is often associated with missing data and lack of homogeneity that could lead to an overestimation or underestimation or even nondetection of differences and associations. Another limitation that should be acknowledged is that indirect costs were restricted to productivity losses from absenteeism (sick leave of patients or informal caregivers), whereas the burden from presenteeism, substitution, and training of new employees and disability compensation/benefits was not estimated, thus potentially leading to underestimation of the actual indirect costs. Overall, differences in treatment and health care systems, as well as in methods for cost estimates could also lead to an over-/underestimation of the actual costs of OA found among different OA patients’ population across geographic settings. On the contrary, the study’s strength relies on the fact that it is prospective and examined a well-defined, relatively large and likely to be representative group of patients with end-stage hip and knee OA. The age and gender profiles of the study participants reflect those of the entire patient populations in international settings.
The PONOS study confirmed for the first time in Greece the substantial economic burden on patients, health care providers, governments, and the society as a whole, imposed by OA. Our findings emphasize the need for appropriate intervention through public health strategies to address risk factors for OA, in conjunction with interventions for the timely diagnosis and effective management of the disease. With regards to management, there is an unmet need for new molecules that will focus both on symptomatic treatment, as well as joint regeneration. This is the only way to improve patients’ health outcomes and reduce the global burden of OA on society.
Supplemental Material
sj-docx-1-car-10.1177_19476035231196524 – Supplemental material for Moderate to Severe Osteoarthritis: What is the Economic Burden for Patients and the Health Care System? Insights from the “PONOS” Study
Supplemental material, sj-docx-1-car-10.1177_19476035231196524 for Moderate to Severe Osteoarthritis: What is the Economic Burden for Patients and the Health Care System? Insights from the “PONOS” Study by P. Savvari, I. Skiadas, M. Barmpouni, S. A Papadakis, V. Psychogios, A.P. Pastroudis, G.A. Skarpas, A. Tsoutsanis, A. Garofalakis, G. Katsifis, O.D. Argyropoulou, D. Boumpas and D. Menegas in CARTILAGE
Footnotes
Acknowledgments and Funding
The study was funded by Pfizer Hellas.
Declaration of Conflicting Interests
Paraskevi Savvari, Ioannis Skiadas, Myrto Barmpouni and Damianos Menegas are currently Pfizer employees. The rest of author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki and Guidelines for Good Epidemiological Practices (GPP) and was approved by the respective institutional review boards (IRBs) at all participating sites. The corresponding IRBs were: Board of Directors “Laiko” General Hospital of Athens, Board of Directors Attikon University General Hospital, Scientific Board—Ethics Committee Naval Hospital of Athens, Scientific Board Asclepeion General Hospital of Athens, Scientific Board MITERA Private Hospital, Scientific Board General Hospital of Attica KAT. Informed consent was obtained from all subjects.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.