
Abstract
Objective:
The purpose of this article is to report on a distinctive pattern of linear femoral head chondral lesions that were observed in 7 patients who underwent hip arthroscopy for the treatment of mixed-type femoroacetabular impingement (FAI).
Design:
Between 2010 and 2012, 702 patients were treated with hip arthroscopy at our institution for symptomatic FAI. Among those patients, 7 were found to have a unique vertical chondral fissure located on the posterior femoral head. A retrospective review of the preoperative history, physical examination, and radiographic findings in addition to the intraoperative findings and surgical procedures performed was carried out for each patient.
Results:
All patients were diagnosed with mixed-type FAI by dynamic examination intraoperatively. The femoral head cartilage lesions were noted to be both linear and deep and resembled the appearance of a crevasse. Three of the 7 patients in whom these lesions were identified reported an acute event preceding their pain. Of the other 4 patients, 3 were involved in sports that involved vigorous rotational hip movements: golf, tennis, and wrestling. Notably, none of these lesions were identifiable on preoperative 3-T MRI scans.
Conclusions:
This series reports on a previously undefined femoral head cartilage lesion. It is hypothesized that increased pathologic translational movements and perching of the femoral head on the posterior rim of the acetabulum create this pattern of chondral damage. Recognition of this pattern of damage on the femoral head is important in the setting of mixed-type FAI.
Introduction
The intrinsic stability of the hip is critical in the prevention of subluxation or frank dislocation and ensures that the integrity of the articular surfaces remains undamaged. As a ball and socket joint connecting the axial to appendicular skeleton, the hip has a strong inherent osseous stability. This is further strengthened by static and dynamic stabilizers, both ligamentous and muscular, which allow for rotational movement in 3 axes while maintaining minimal translational articulation. It is imperative that each of these structures works in conjunction with the others so that normal hip joint kinematics may be maintained.
Despite being considered a constricted articulation, pathologic translational movements can still occur within the hip joint. In their seminal paper, Ganz et al. 1 demonstrated the association between pincer impingement and posteroinferior acetabular chondral lesions. They suggested that continual anterior abutment between the femoral head–neck junction and the acetabular rim resulted in intraarticular translational shifting and ultimately chondral damage. Labral tears, hyperlaxity states, and iliofemoral ligament rupture or elongation have also been proven capable of causing similar irregular intraarticular motion in isolation.2-4 Biomechanical studies have demonstrated a lateral shift in the center of contact between the femoral head and acetabulum when labral damage is present, 2 as well as increased femoral head external rotation and anterior translation when portions of the iliofemoral ligament are resected. 3 Increased translation and subluxation have even been demonstrated in anatomically normal hips. 4 In a study analyzing ballet dancers with morphologically normal hips, Charbonnier et al. 4 determined that even without the presence of abnormal bony anatomy, there was a high association between femoroacetabular translation and both impingement and subluxation at extreme ranges of motion.
Translational movements not only create abnormal shear stresses on the cartilage surfaces of the hip joint but, as discussed, may also result in pathologic contact between important structures. The aim of this study is to present the physical examination and radiographic and arthroscopic findings of 7 athletic patients who exhibited a distinctive pattern of deep, linear femoral head chondral lesions that we hypothesize occurred secondary to such pathologic contact. The proposed etiology and pathomechanics necessary to create these lesions are discussed.
Methods
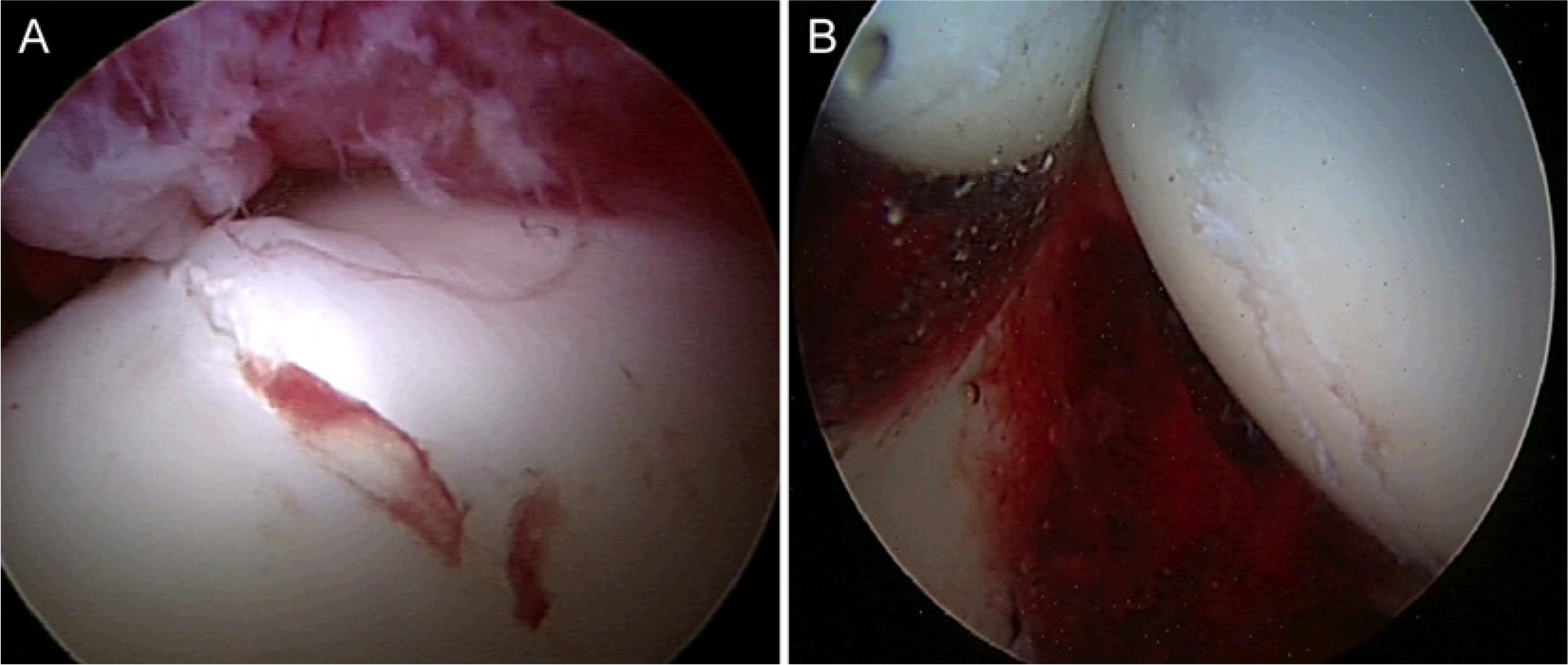
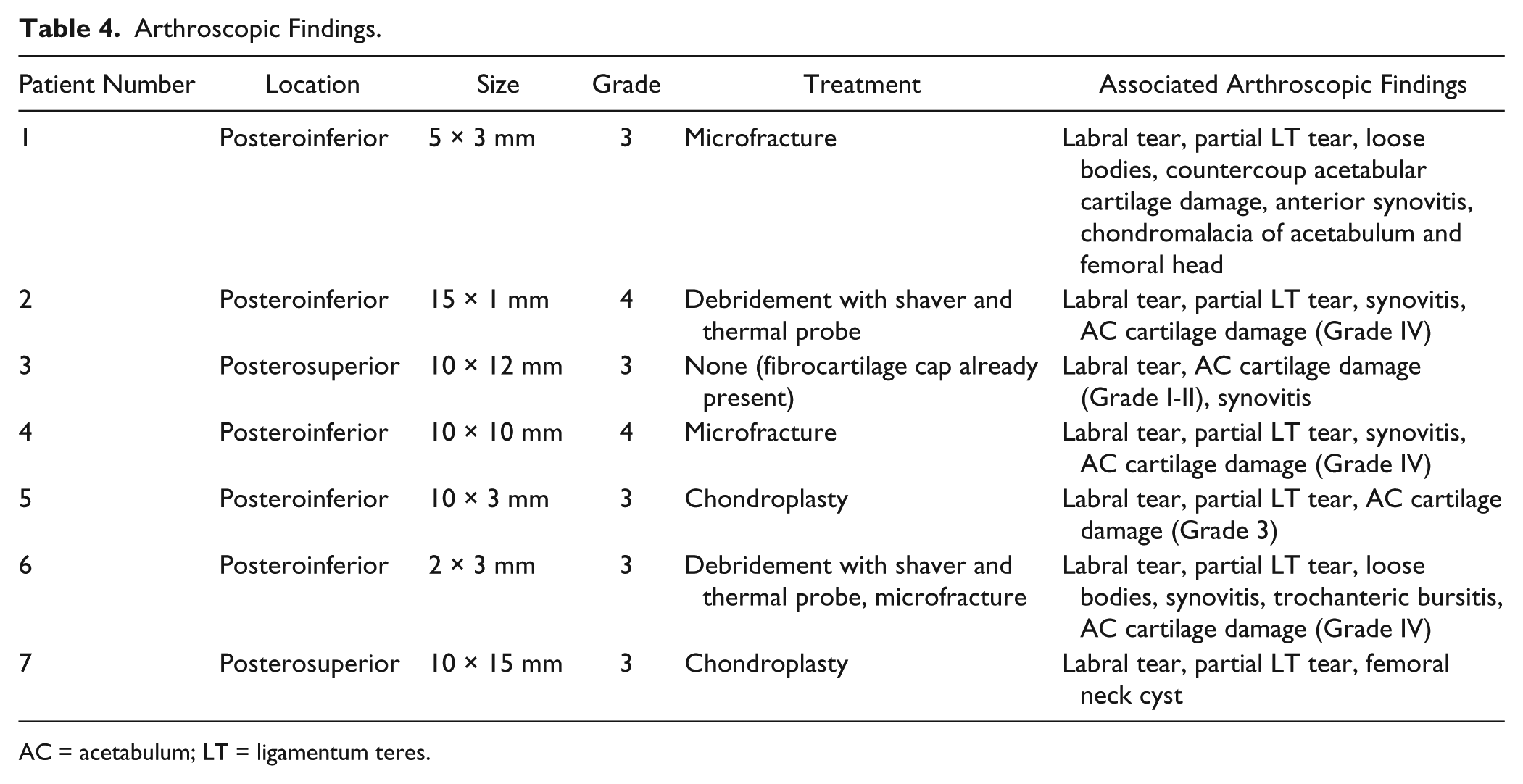
Institutional review board approval was obtained for the present study. Between October 2010 and November 2012, 702 patients were treated with hip arthroscopy for symptomatic femoroacetabular impingement (FAI) at one institution. Patients were considered for inclusion if they underwent arthroscopy during this time period. Patients diagnosed with intraarticular synovial and neoplastic disorders, posttraumatic deformities, postinfectious etiology, and pediatric-related disorders, including slipped capital femoral ephiphysis, Legg-Calve-Perthes disease, and ephiphyseal dysplasia, were excluded from the study. Seven patients presenting for surgery for the treatment of painful FAI were found to have an associated vertical chondral fissure located predominantly over the posteroinferior or posterosuperior surface of the femoral head ( Fig. 1A and B ).
(
There were 4 males and 3 females, with 4 left hips and 3 right hips. The average patient age was 42 years ± 8 months (range = 28-50 years). All patients were athletic and actively involved in sports ( Table 1 ).
Patient Demographics.
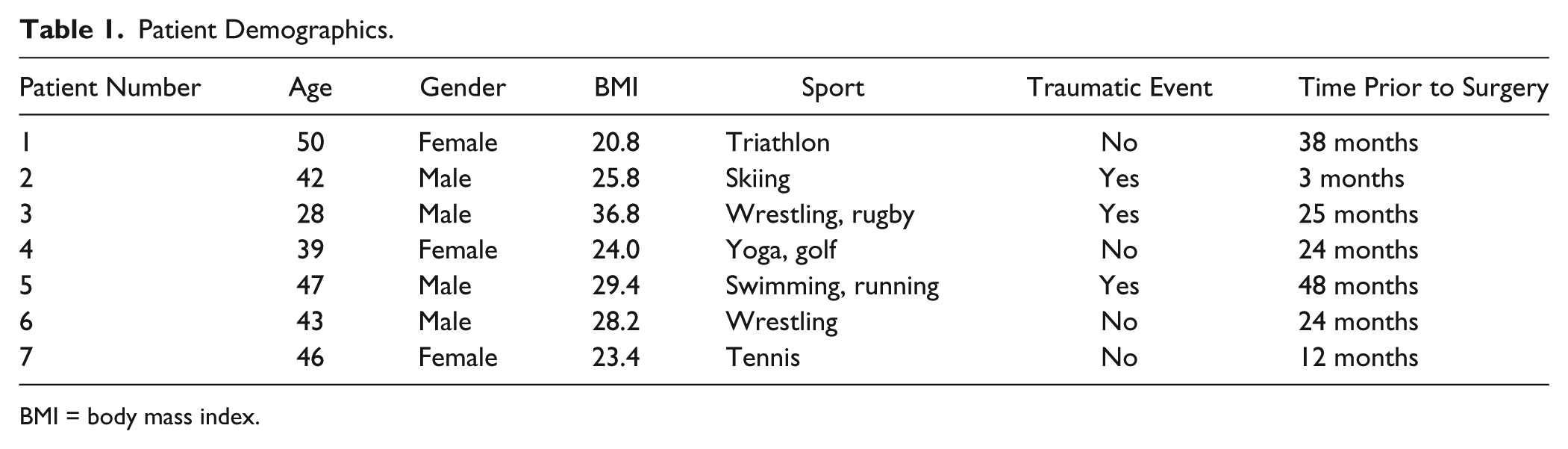
BMI = body mass index.
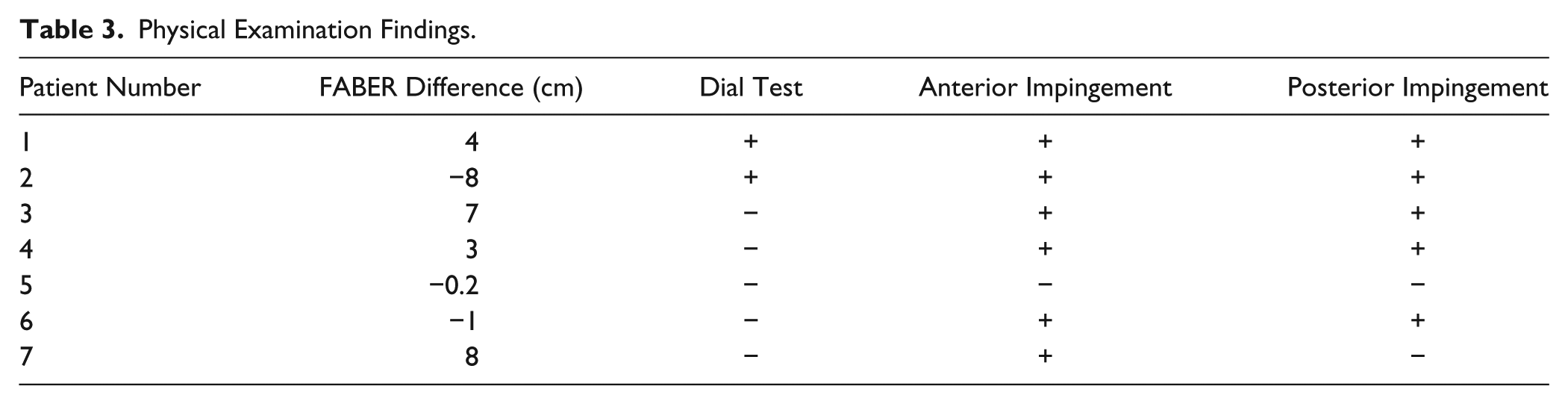
All data were gathered prospectively. Patients were assessed for both clinical and radiographic evidence of FAI, as described by Beck et al. 5 Each patient underwent a focused clinical examination, assessing range of motion (ROM) and hip positions that reproduced their pain. In the supine position, hip flexion, abduction, adduction, internal, and external rotation in flexion and extension, Faber’s test, Dial Test, and anterior and posterior impingement tests were recorded. A Beighton test was carried out to assess for benign joint hypermobility (a score ≥6 was considered lax). 6 Routine radiographs were performed, including supine AP pelvis, false profile, and Dunn lateral views of both hips. A 3-T MRI was carried out without contrast (see Tables 2 and 3 ).
Radiographic Findings.
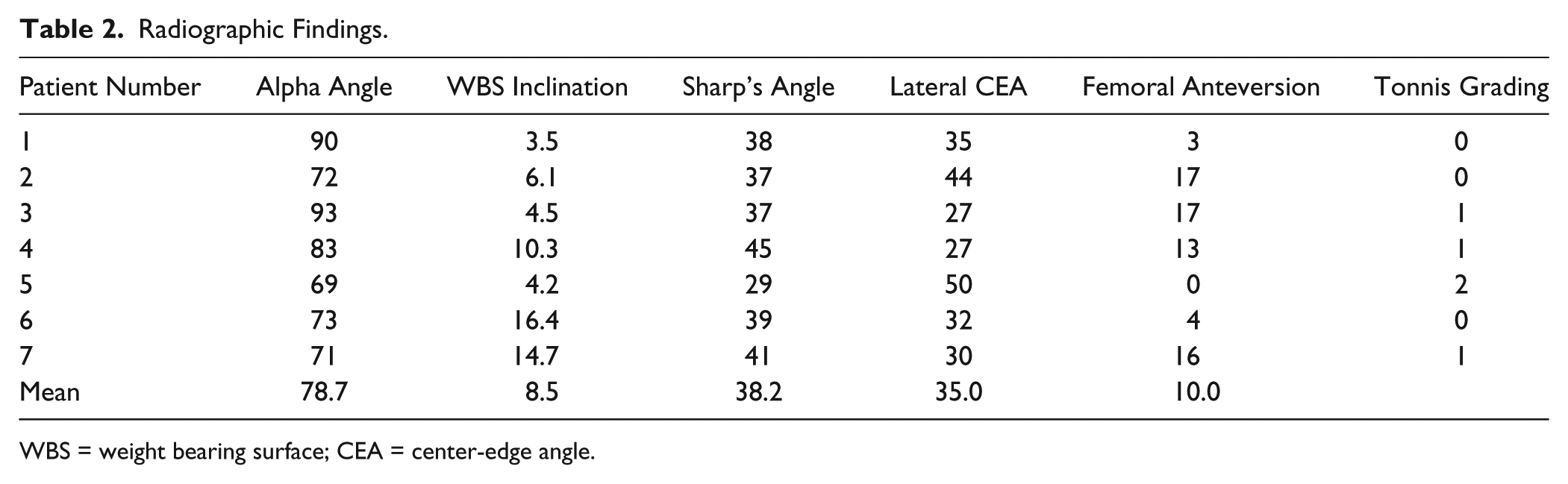
WBS = weight bearing surface; CEA = center-edge angle.
Physical Examination Findings.
The radiographs were assessed for femoral morphology, acetabular morphology, and tonnis grading. Each MRI was reviewed for osseous morphology, labral damage, and documentation of the presence of femoral and acetabular chondral lesions. Standard acetabular and femoral radiographic indices including lateral center-edge angle, femoral anteversion, weight bearing surface (WBS) inclination, sharp’s angle, and alpha angle were recorded on MRI or radiograph. Hip joint space was measured at the lateral sourcil, medial sourcil, and above the fovea on supine AP radiograph.
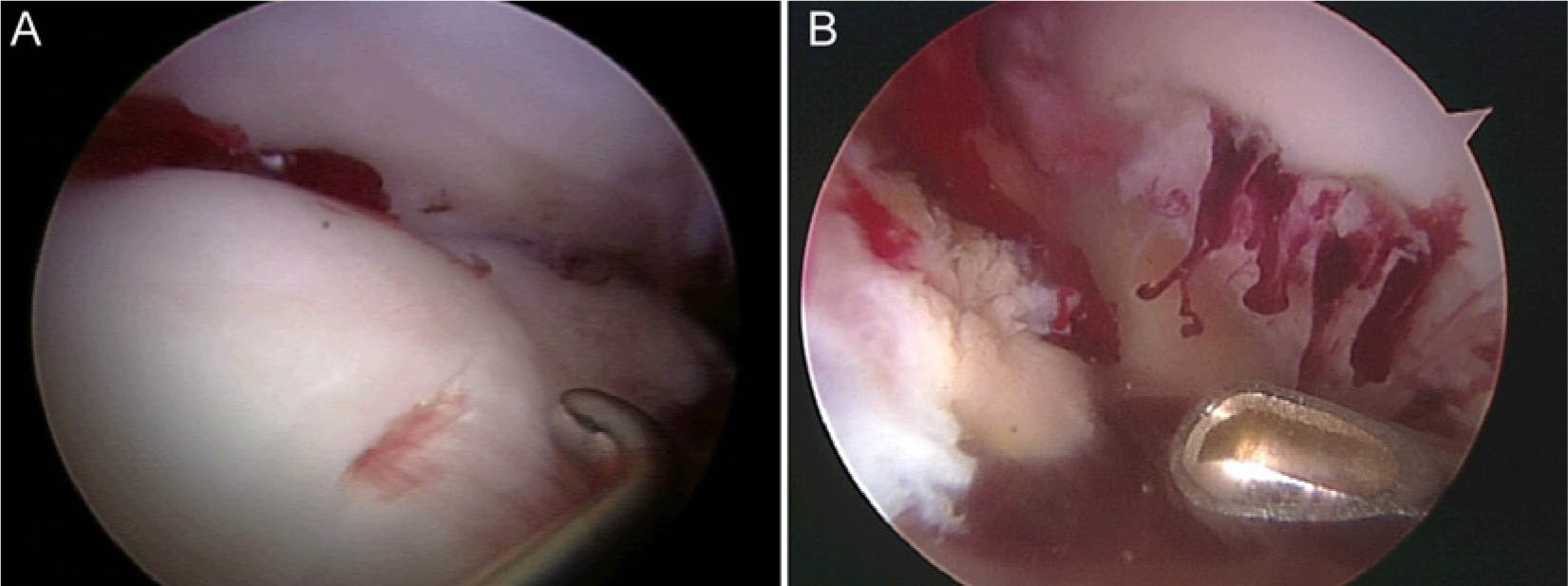
Each hip arthroscopy was performed in the modified supine position with traction gently applied to distract the hip. Standard lateral and midanterior portals were used in all cases. All patients were found to have a labral tear, which were treated with repair, and in 1 case reconstruction of the labrum ( Table 4 ). In addition to treating the femoral and acetabular deformity and any associated cartilage damage, the femoral lesion location and grade were also recorded and the size across its greatest diameter and depth was measured. Treatment of the femoral chondral lesions varied from microfracture, to sealing with fibrin glue, to chondroplasty and thermal probing ( Table 4 ; Fig. 2A and B ).
Arthroscopic Findings.
AC = acetabulum; LT = ligamentum teres.
(
After surgery, patients were mobilized as soon as possible depending on the time of day that the surgery was completed. Patients were limited to 20 pounds of flat foot weightbearing in an abduction and external rotation limiting brace for approximately 3 to 6 weeks to permit time for the cartilage repair to mature. In the case that a microfracture was performed, this regimen was continued for 6 to 8 weeks. For the first 4 to 6 weeks following surgery, physical therapy consisted of passive or actively assisted hip ROM exercises, with isometric exercises focusing on the gluteus medius. After 6 weeks, weightbearing as tolerated was encouraged and patients were instructed, under physical therapy supervision, in gluteal, tensor fascia lata, and lower extremity strengthening. At this time, a sport specific regimen was also instituted, and based on patient progress and hip strength, a return to sporting activities was typically possible between 10 and 16 weeks postoperatively. 7
Results
Preoperative Findings
All patients had a preoperative diagnosis of FAI.8,9 Three of the 7 patients reported a specific traumatic event preceding their hip pain. No patients demonstrated ligamentous laxity or reported fellings of hip instability.
The average duration of symptoms prior to surgical intervention was 24.9 months (range = 3-48 months).
All patients had >2 mm of joint space at the lateral sourcil, middle sourcil, and above the fovea on supine AP pelvis radiographs. None of the femoral chondral defects were diagnosed preoperatively using 3-T MRI.
Surgical Findings
A definitive diagnosis of mixed-type FAI was made for every patient during arthroscopy based on evidence from dynamic intraoperative examination. The ranges of femoral head lesion and location of lesions are shown in Table 4 . The crevasse lesion necessitated microfracture for treatment in 3 cases. One patient had a Tonnis grade of 2, and 3 patients had a Tonnis grade of 1. All patients were found to have labral tears in association with the chondral defects, extending from the anterosuperior to posterosuperior aspect of the acetabulum. All patients required acetabular rim trimming to correct for pincer abnormalities, as well as femoral neck osteoplasty to correct for any cam lesions.
Discussion
This series describes a lesion on the posterior aspect of the femoral head, which has not been previously described, in a cohort of high-activity-level patients. The term Crevasse Lesion was used to denote the appearance of a linear cleavage in the cartilage on the femoral head and its resemblance to a crevasse in a glacier—deep cracks within an ice sheet with vertical or near-vertical walls. It is postulated that the location of the “Crevasse Lesion” results from a combination of a pathological posterior translational motion of the femoral head leading to partial subluxation and posterior impaction between the head and the posterior acetabular rim. The unique appearance of the lesion is believed to result from transient perching of the femoral head on the posterior acetabulum prior to re-articulation. The mechanism is not dissimilar to the creation of a Hill-Sach’s lesion on the posterior aspect of the humeral head following bony impaction against the anterior glenoid rim during an anterior shoulder dislocation. 10
Zaltz and Leunig 11 have previously described the clinical, radiographic, and surgical characteristics of a rare focal anterolateral parafoveal femoral chondral defect associated with FAI. In their study of 10 young patients, who participated in sports involving rapid, forceful, repetitive hip flexion, they reached a hypothesis that these motions, in the presence of FAI, induce shear stresses on the femoral head that can produce pathological changes. The location and shape of the lesions differ from the findings of this study, however. The lesions reported by Zaltz and Leunig 11 were located predominantly in the posterosuperior quadrant of the femoral head and involved a greater surface area, as opposed to the posteroinferior quadrant location and linear nature of 5 lesions reported in this series. There were 2 lesions of the posterosuperior quadrant in this series; however, both were linear in nature and not large surface area lesions. In addition, the patients presented with an isolated cam impingement in 8 of the cases and mixed impingement in only 2 cases, compared to a mixed pattern in all 7 of the patients presented here. Although, there is little doubt that the pathomechanics are similar in each group, it is likely that the additional presence of a pincer deformity on the acetabular side contributed to the development of a curvilinear chondral defect on the femoral head, as it would increase the potential for the femoral head to lever out of the joint, ultimately resulting in a period of subluxation or perching on the posterior rim of the acetabulum.
Biomechanical and kinematic studies have demonstrated that translational movement of the femoral head within the acetabulum occurs in the setting of hypermobile states, as well as in the presence of a tear of the iliofemoral ligament or labrum.2-4 Lamontagne et al. 12 have shown, in a kinematic study comparing 16 cam FAI patients with16 control patients, that cam impingement had a detrimental effect on sagittal pelvic ROM. The subjects with cam impingement were unable to reach as low of a squat as the control group. It is possible that these limitations are an adaptation to the abnormal biomechanical environment imposed by FAI. Furthermore, these accommodations may fail during sports activities in extremes of motion resulting in translational movements and/or subluxation inside the hip joint. It is felt that a similar phenomenon occurred within the current patient population. In these instances, it is possible that sudden forceful abutment between the cam protrusion and pincer overcoverage during hip flexion acts to transiently lever the femoral head out of its articulation, subluxing the joint just enough for it to impact against the acetabular rim before reducing again once the joint motion is stopped. The presence of labral tears in all of the subjects examined in this series would also reinforce the suggestion that a translational force was at play in the etiology of these lesions.
In support of this pathomechanical theory, FAI was observed in 9 out of 14 professional athletes who sustained traumatic hip dislocations, which were subsequently treated with hip arthroscopy. 13 In this hip dislocation study, Philippon et al. found 4 patients with mixed-type impingement, 4 patients with cam impingement, and 1 patient with pure pincer impingement. These findings suggest a similar mechanism between the dislocation group of patients and the patients who sustained a “Crevasse Lesion”; the difference being the “Crevasse Lesion” patients were exposed to a lower degree of energy around their hips. This is corroborated by the fact that 3 of the 7 patients in which these lesions were identified had an acute event preceding their pain; not severe enough to result in frank dislocation, but instead we postulate represented the partial subluxation event. Of the other 4 patients, 3 were involved in sports that involved vigorous rotational hip movements—golf, tennis, and wrestling.
Interestingly, a mirror lesion on the corresponding posterior acetabular labral rim was not identified. This could be explained by the differences in collagen configuration between the posterior and anterior areas of the acetabulum. Multiple studies have identified differences in both the collagen fiber orientation as well as in the number of attachment extensions between the posterior and anterior labrum.14,15 These differences have already been suggested by several authors as the reason for the anterior labrochondral junction being weaker and more vulnerable to degenerative changes and traumatic events.16,17 These studies may also help explain the lack of a corresponding labral lesion in the posterior acetabular rim in our patients.
The hip joint cartilage is especially thin in comparison to other joints, and the treatment of cartilage injuries continues to represent a challenge for the orthopaedic surgeon.18,19 Translational movements are deleterious and result in an increased shear stress that can be especially harmful if the more random and loose fibers of the cartilage middle layer are exposed. 20 The impaction lesion of the femoral head against the posterior rim, seen in the “Crevasse Lesion” patients, may accelerate a degenerative process, exposing the deeper layers of the cartilage tissue to a harmful and repetitive translational motion that is associated with FAI.
The “Crevasse Lesions” presented in this series represent a heretofore undefined lesion in the posteroinferior aspect of the femoral head. It is postulated to occur as a result of subluxation of the hip and perching of the femoral head on the posterior lip of the acetabulum. These lesions were seen in 7 cases of mixed FAI in a group of active patients. This series of patients serves to highlight the need for vigilance both while taking a history and while performing hip arthroscopy to recognize the presence of these cartilage defects on the femoral head.
Conclusion
In FAI of the hip, it is generally accepted that damage to the articular surface of the femoral head is less common than injury to either the chondrolabral junction or articular cartilage of the acetabulum. However, this series demonstrates that in the presence of pathologic translational movement of the hip, as occurs in high-demand patients with FAI, there is an increased risk for the development of earlier, localized, and severe femoral head chondral lesions.
Footnotes
Acknowledgment and Funding
Research support has been provided to the institution by Smith & Nephew, Siemens, Ossur, and Arthrex.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The author (MJP) has potential conflict of interest with Smith & Nephew (consultant, royalties), Arthrosurface (stock, royalties), Bledsoe (royalities), DonJoy (royalties), Slack (royalties), Elsevier (royalties).
Ethical Approval
This study was institutional review board approved.