
Abstract
Objective
The objective of this study is to establish which patient and lesion characteristics are related to the clinical outcome after microfracture of cartilage defects in the knee.
Study design
Systematic review.
Methods
After preregistration, PubMed, Embase, and Cochrane were searched for studies that analyzed prognostic factors for the outcome of microfracture treatment in the knee. The criteria for inclusion were outcome measured using Patient-Reported Outcome Measures (PROMs), a clinical study with ≥10 participants receiving microfracture, and a minimal follow-up period of 1 year.
Results
For none of the investigated prognostic factors, effect size reporting was sufficiently homogeneous to conduct a meta-analysis. However, a majority of the included studies identified higher age, larger lesion size, longer preoperative symptom duration, and previous surgery on the ipsilateral knee, especially meniscectomy and anterior cruciate ligament reconstruction, as factors that are reported to be correlated to a less favorable outcome. A lesion location that does not include the trochlea or the patellofemoral joint and is not weightbearing, a nondegenerative mechanism of injury, and a single lesion were reported as factors that predict a favorable outcome. As to gender, body mass index, preoperative activity level, smoking, and concomitant knee surgery, the included articles were inconclusive or no effect was reported.
Conclusions
Several factors correlated with the clinical result after microfracture treatment. However, the information on the effect sizes of the influence on clinical outcome is incomplete due to poor reporting. Large-scale registries or pooling of homogeneous, well-reported data is needed to work toward prognostic models. That would be an important step toward personalized treatment.
Introduction
Cartilage lesions in the knee can lead to pain and functional impairment, comparable to patients with end-stage osteoarthritis who are scheduled for total knee arthroplasty.1,2 Most cartilage lesions have a traumatic origin and are located on the medial femoral condyle and patellofemoral joint. 3 The natural healing capacity of cartilage and regeneration after surgical repair are challenging, often only providing fibrocartilage defect filling rather than the native hyaline cartilage type. Untreated cartilage defects are a strong predictor for osteoarthritis development, which causes pain, a decrease in joint function, and a large demand for orthopedic care later in life.4 -6
First described by Steadman et al., 7 microfracture has been stated as the “golden standard” in the surgical treatment of full-thickness cartilage defects in the knee. Evidence is mostly derived from case series, cohort studies, and clinical trials. However, subjects in these studies often do not represent the typical patient in clinical practice. 8 Namely, microfracture is mostly investigated and consequently advised for smaller primary defects in young individuals by international guidelines, but in clinical practice it is often applied in older individuals with more complex lesions and comorbidities.1,9 -12 Indeed, in clinical practice, microfracture is one of the most used cartilage repair techniques and mostly applied in middle-aged individuals.13 -16 Similarly, this is driven by its technical ease, low costs, and high availability. 17 However, there is mounting evidence that the standard microfracture awls may cause subchondral bone sclerosis and cyst formation.18,19 Moreover, failed microfracture may also jeopardize the success of consecutive biological treatments such as autologous chondrocyte implantation (ACI).20 -23 The quality of the cartilage repair tissue after microfracture is also inconsistent and fluctuates, particularly with increasing age.12,24 -26 The exact reasons therefore remain unclear. Other techniques such as scaffold augmentations, osteochondral allografting (OCA) or autograft transplantation (OAT), and ACI challenge the position of microfracture as the first choice in operative management as there is increasing evidence that they are more durable than microfracture.12,27
There are particular concerns when microfracture is applied in larger defects and middle-aged patients. 12 To optimize the proper use of microfracture treatment, it is important to gather the evidence on factors that should be taken into account during (shared) treatment decision-making. There are several prognostic factors that have been named for microfracture outcomes, such as age, lesion size, and location. 28 Surprisingly and to the best of our knowledge, a study that scrutinizes the evidence for the influence of these factors has not been performed. Therefore, in this review, we aim to identify the prognostic factors that influence the clinical outcome of microfracture surgery of cartilage defects in the knee.
Methods
Literature Search and Selection of Studies
PubMed, Embase, and Cochrane were searched from inception until June 19, 2021 (registration in PROSPERO ID: CRD42020177512). The search was constructed using the following key words, including synonyms and closely related terms: “osteochondral lesion,” “osteochondritis dissecans,” “knee,” and “microfracture.” The full search strategies for all databases are listed in Supplemental Appendix I. Duplicates and manuscripts in any other language than English or German were excluded. Articles were included when (1) the study evaluated the outcome of microfracture treatment for cartilage defects based on Patient-Reported Outcome Measures (PROMs), (2) it was a clinical study with ≥10 participants in the microfracture-receiving group, (3) there was a minimal follow-up period of 1 year, and (4) the study addressed the preoperative or perioperative patient or lesion characteristics and their relation to the outcome. Concomitant procedures were allowed, but studies that only included patients with specific concomitant injuries were excluded. The primary outcomes were correlation coefficients, odds ratios, or differences between subgroups. Reviews, meta-analyses, cost-effectiveness analyses, congress abstracts, animal studies, and case series were excluded. Titles and abstracts were independently screened for relevance by 2 researchers (I.M.v.T. and K.S.E.) using Rayyan (www.rayyan.ai). If there was no consensus on the inclusion of a paper, a discussion with a third researcher (P.P.W.v.H.) was conducted until consensus or majority vote was reached.
Data Extraction
A data extraction form was created to obtain the following information: first author, journal, year of publication, number of patients receiving microfracture, lesion location, lesion size, age, etiology, history of knee trauma and/or surgery, follow-up, body mass index (BMI), smoking, concomitant injuries and/or procedures, and the International Cartilage Repair Society (ICRS) and/or Outerbridge Classification. When available, the PROMs, correlation (coefficient), uni- or multivariate analysis, subgroup analysis, and P values were collected for all identified following prognostic factors. If the primary outcomes were not completely reported, the corresponding authors of the included articles were contacted by e-mail, with a reminder e-mail after 8 to 10 weeks.
Quality Assessment
The included studies were subjected to a quality assessment based on the Methodological Index for Non-Randomized Studies (MINORS) by Slim et al. 29 This instrument was designed to assess the methodological quality of nonrandomized surgical studies, whether comparative or noncomparative. The maximal score was 16 for noncomparative and 24 for comparative studies.
Data Analysis
A narrative synthesis of the evidence and the statistical significance of the findings are given.
Results
Study Identification
After the literature screening, 23 articles that met the inclusion criteria were identified ( Fig. 1 ).30 -52 The most-studied prognostic factors were age, lesion size, gender, lesion location, and symptom duration. Other mentioned factors were defect count, BMI, smoking, concomitant knee surgery, mechanism of injury, previous knee surgery, activity level, and postoperative treatment, all of which will be addressed below.
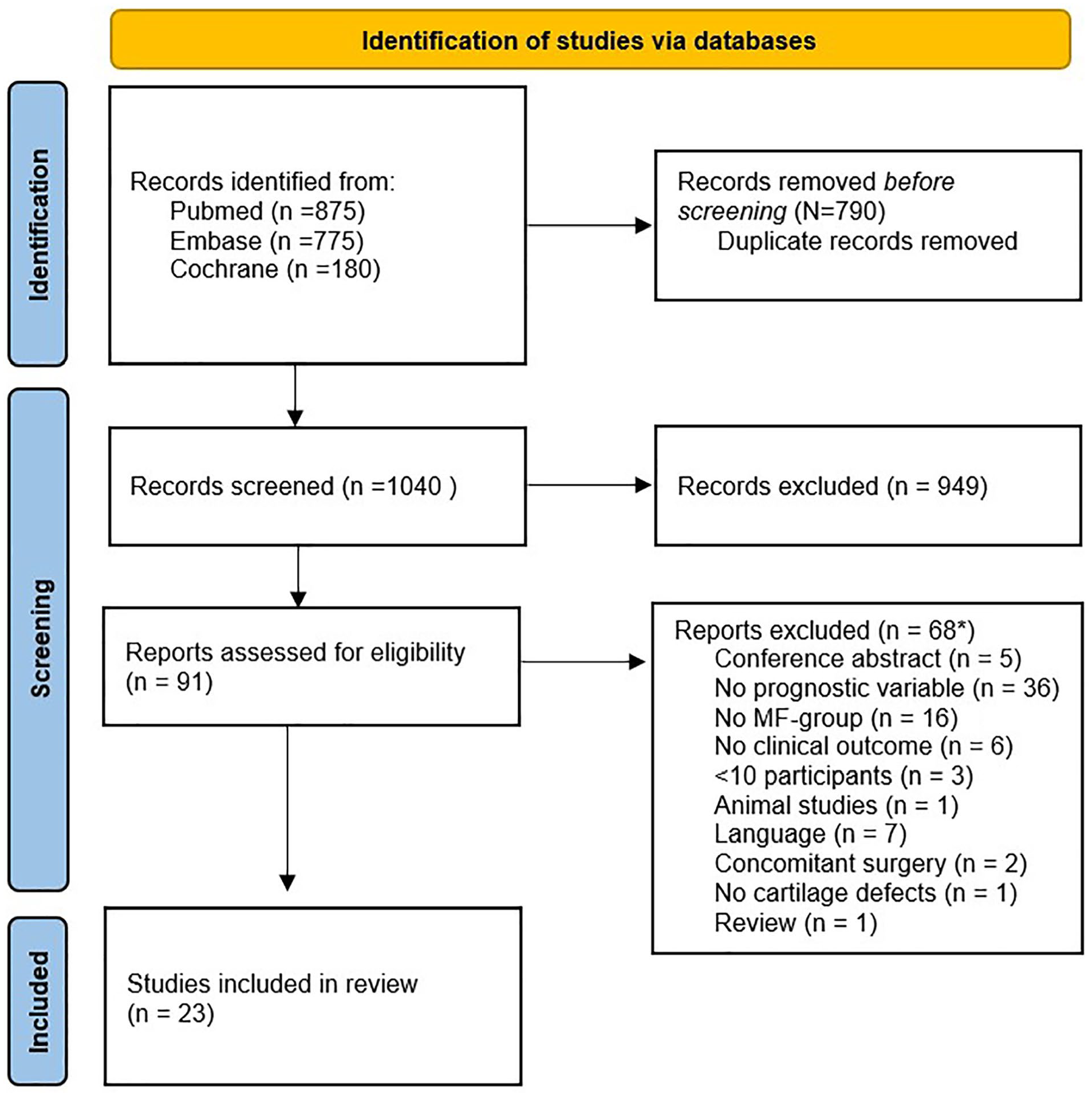
PRISMA flowchart of the selection process. 53 PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analyses; MF = microfracture.
Quality Assessment
Overall, a reasonable study quality was found throughout the studies ( Figure 2 ). The mean score for the included noncomparative studies was 13.9 (N = 16, range: 12-16), and for the comparative studies it was 20.4 (N = 7, range: 19-22). Most of the quality issues were due to loss to follow-up and the prospective calculation of the study. Due to prognostic factors being a secondary outcome measure in most studies, the prognostic calculation of the studies was usually not aimed at those.
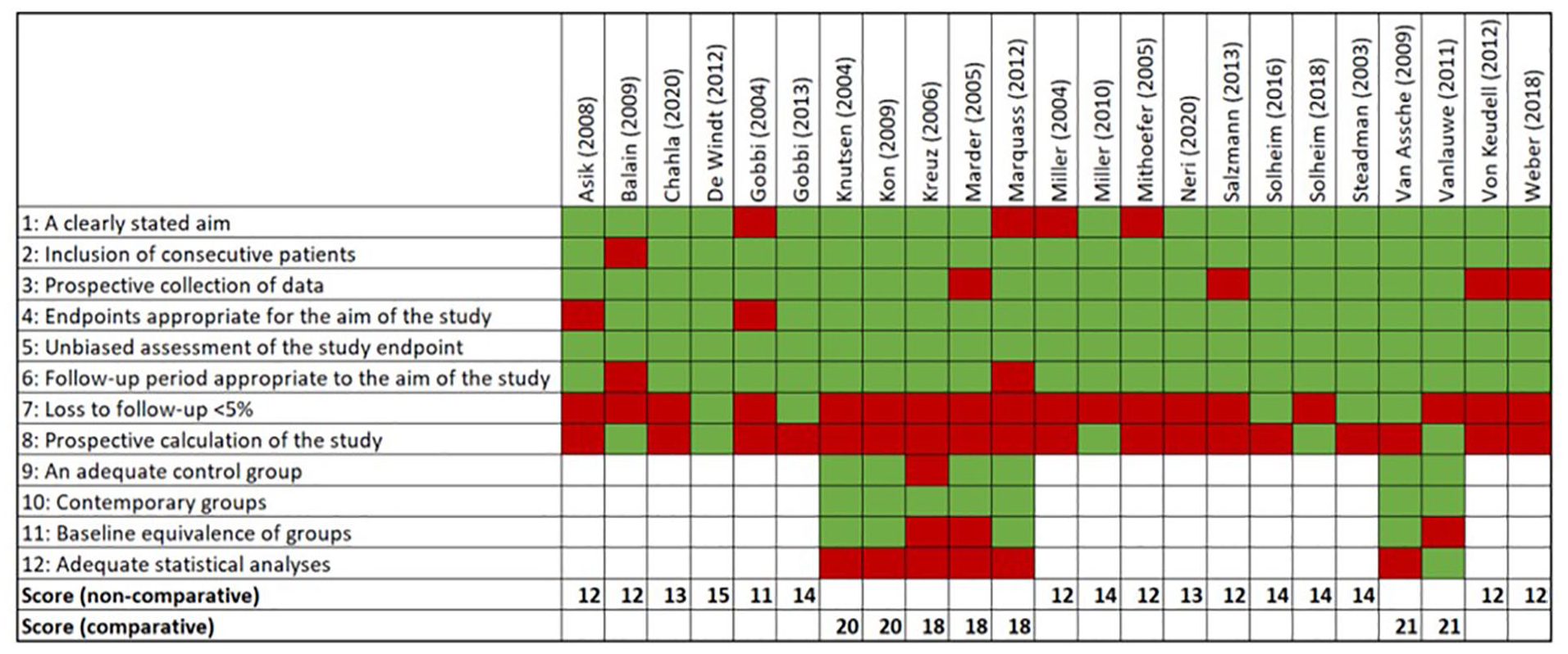
MINORS quality assessment. MINORS = Methodological Index for Non-Randomized Studies
Summary of Evidence
Due to poor reporting and heterogeneity of effect sizes, pooling of data was not possible. Therefore, a narrative synthesis of the evidence was given. Furthermore, the number of studies that studied a potential prognostic factor was counted and the ratio of studies that reported the factor to be significant to nonsignificant was reported.
Age
Age was the most frequently studied prognostic factor. Eighteen of the 23 included studies analyzed the relationship between the age of the patient and the clinical outcome of microfracture by means of either correlation ( Table 1 ) or subgroup analysis ( Table 2 ) with a cutoff age ranging between 25 and 45 years. Ten of the 18 papers reported a significant effect. A negative correlation with increasing age was reported in 4 of 10 studies (4/10). Lower scores in a subgroup analyses were observed in 7 of 10 studies (7/10, 1 study reported both). No significant effect of age was reported 8 times, either in correlation analysis (N = 6) or in subgroups (N = 2).
Correlations for Age.
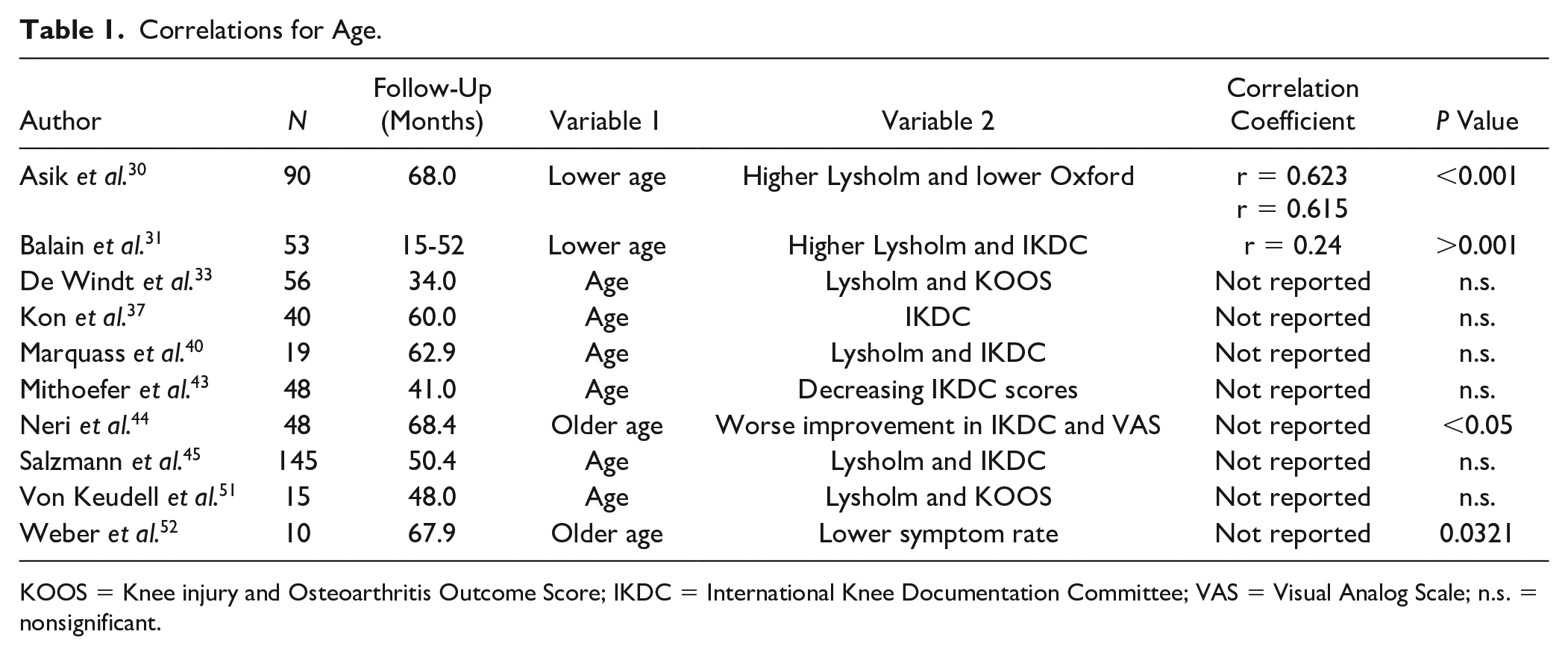
KOOS = Knee injury and Osteoarthritis Outcome Score; IKDC = International Knee Documentation Committee; VAS = Visual Analog Scale; n.s. = nonsignificant.
Subgroup Analyses for Age.
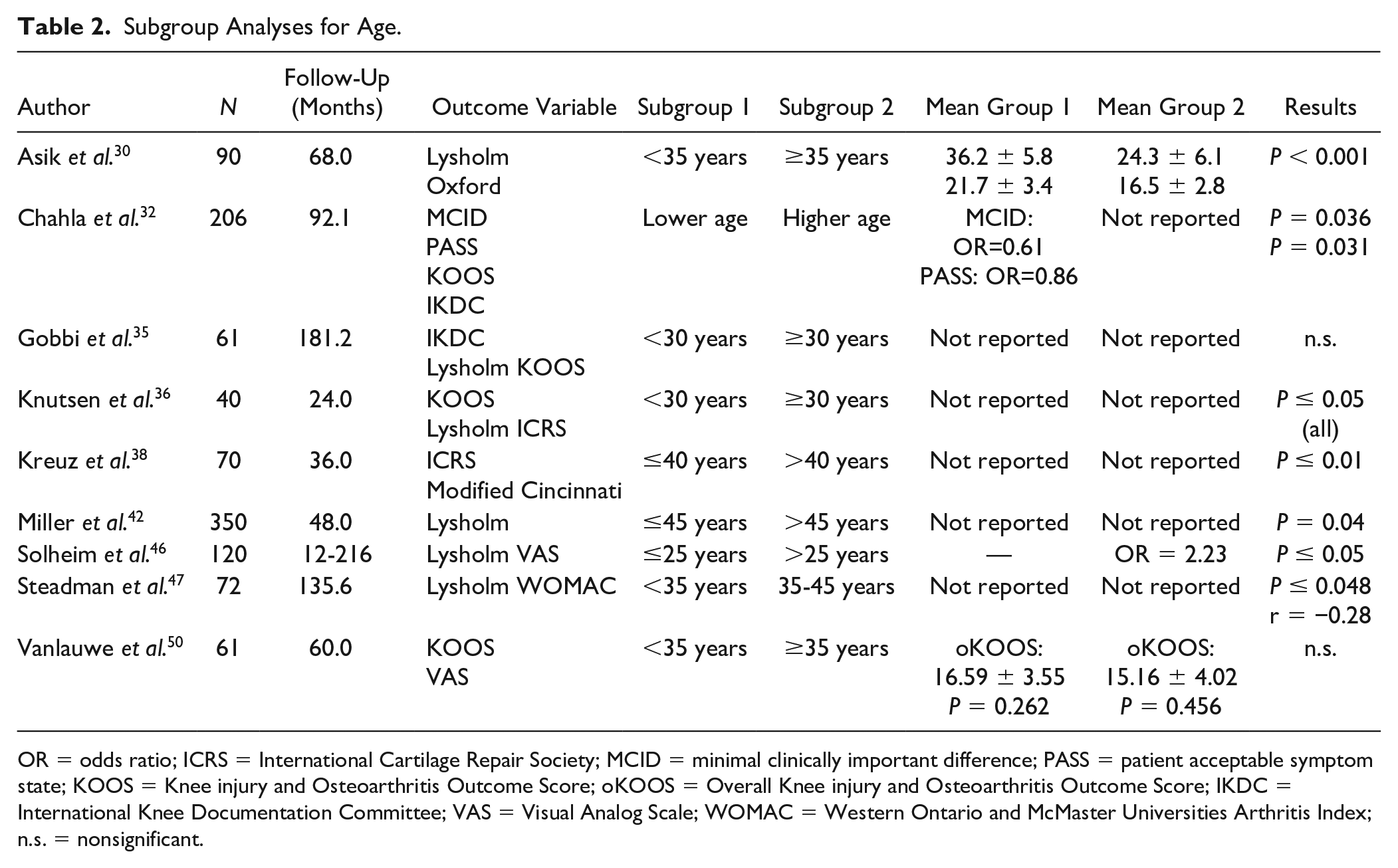
OR = odds ratio; ICRS = International Cartilage Repair Society; MCID = minimal clinically important difference; PASS = patient acceptable symptom state; KOOS = Knee injury and Osteoarthritis Outcome Score; oKOOS = Overall Knee injury and Osteoarthritis Outcome Score; IKDC = International Knee Documentation Committee; VAS = Visual Analog Scale; WOMAC = Western Ontario and McMaster Universities Arthritis Index; n.s. = nonsignificant.
Lesion size
Thirteen of the 23 studies reported the analysis of the influence of lesion size on patients’ clinical outcome via a correlation with PROMs or a subgroup analysis with a cutoff between 2 and 4 cm2. Eight of the 13 studies found a significant correlation (N = 2, Table 3 ) or a worse score in subgroup analysis (N = 6, Table 4 ) for larger lesions. The remaining 5 studies found no significant effect of lesion size.
Correlations for Lesion Size.
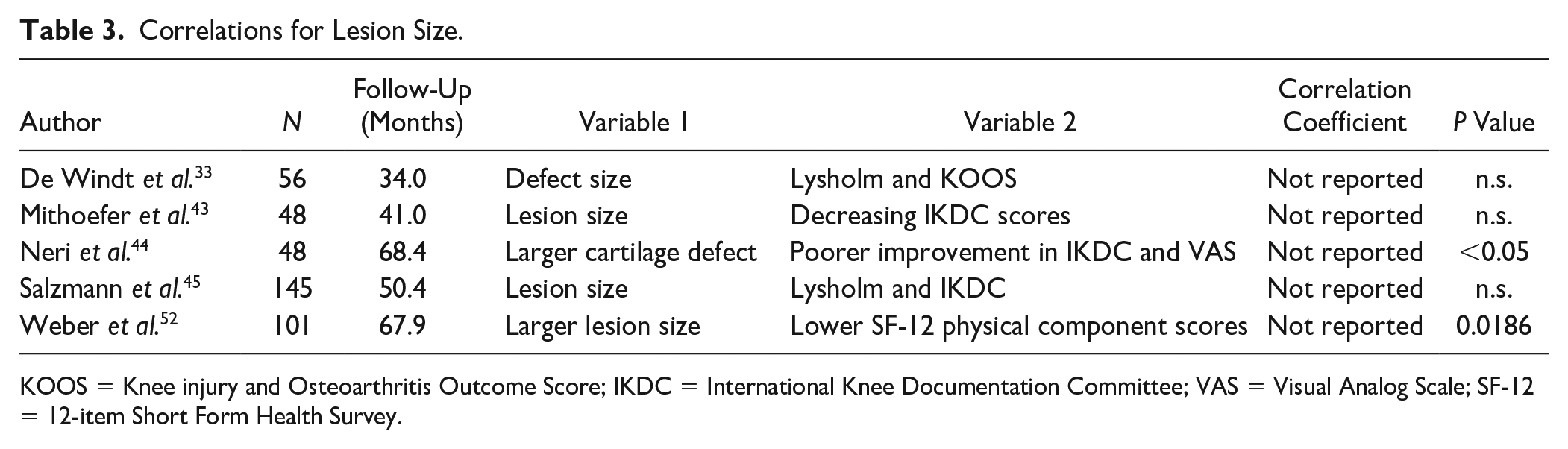
KOOS = Knee injury and Osteoarthritis Outcome Score; IKDC = International Knee Documentation Committee; VAS = Visual Analog Scale; SF-12 = 12-item Short Form Health Survey.
Subgroup Analyses for Lesion Size.
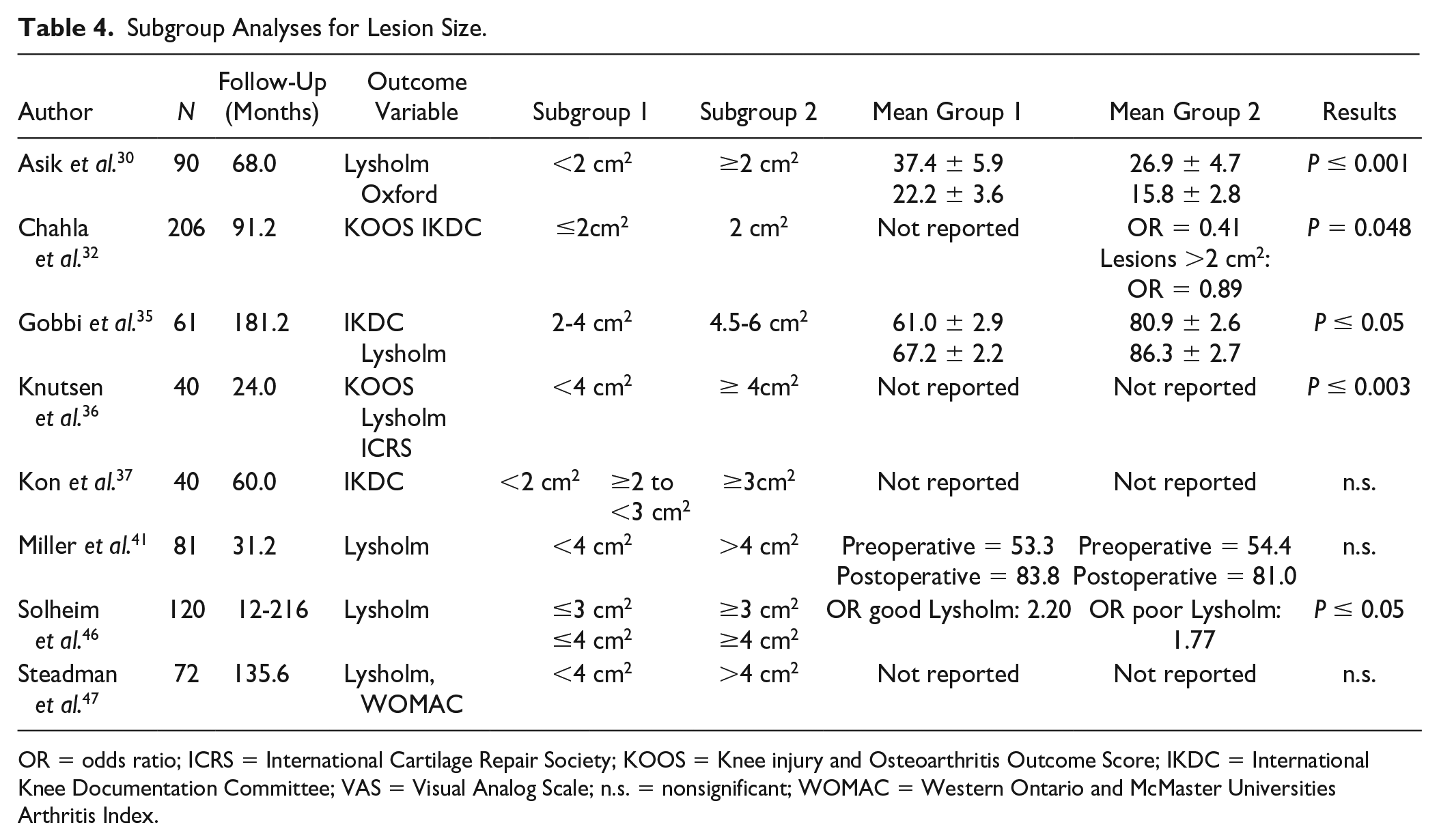
OR = odds ratio; ICRS = International Cartilage Repair Society; KOOS = Knee injury and Osteoarthritis Outcome Score; IKDC = International Knee Documentation Committee; VAS = Visual Analog Scale; n.s. = nonsignificant; WOMAC = Western Ontario and McMaster Universities Arthritis Index.
Lesion location
Seven studies conducted research on the effect of lesion location on postoperative scores and end results. The same PROMs as mentioned earlier were maintained. From the 3 studies mentioning a correlation for lesion location, 1 article found a significant correlation ( Table 5 ). Five subgroup analyses were performed ( Table 6 ). In 4 cases, a significant difference was found. Asik et al. 30 found better scores at 68 months of follow-up comparing weightbearing to non-weightbearing zones. Gobbi et al. 34 found better outcomes for lesions located at the medial compartment compared with the lateral compartment. Kreuz et al. 38 reported worse outcome when the lesion was located at the patella or trochlea compared with the condyles or tibial plateau.
Correlations for Lesion Location.

n.s. = nonsignificant.
Subgroup Analyses for Lesion Location.
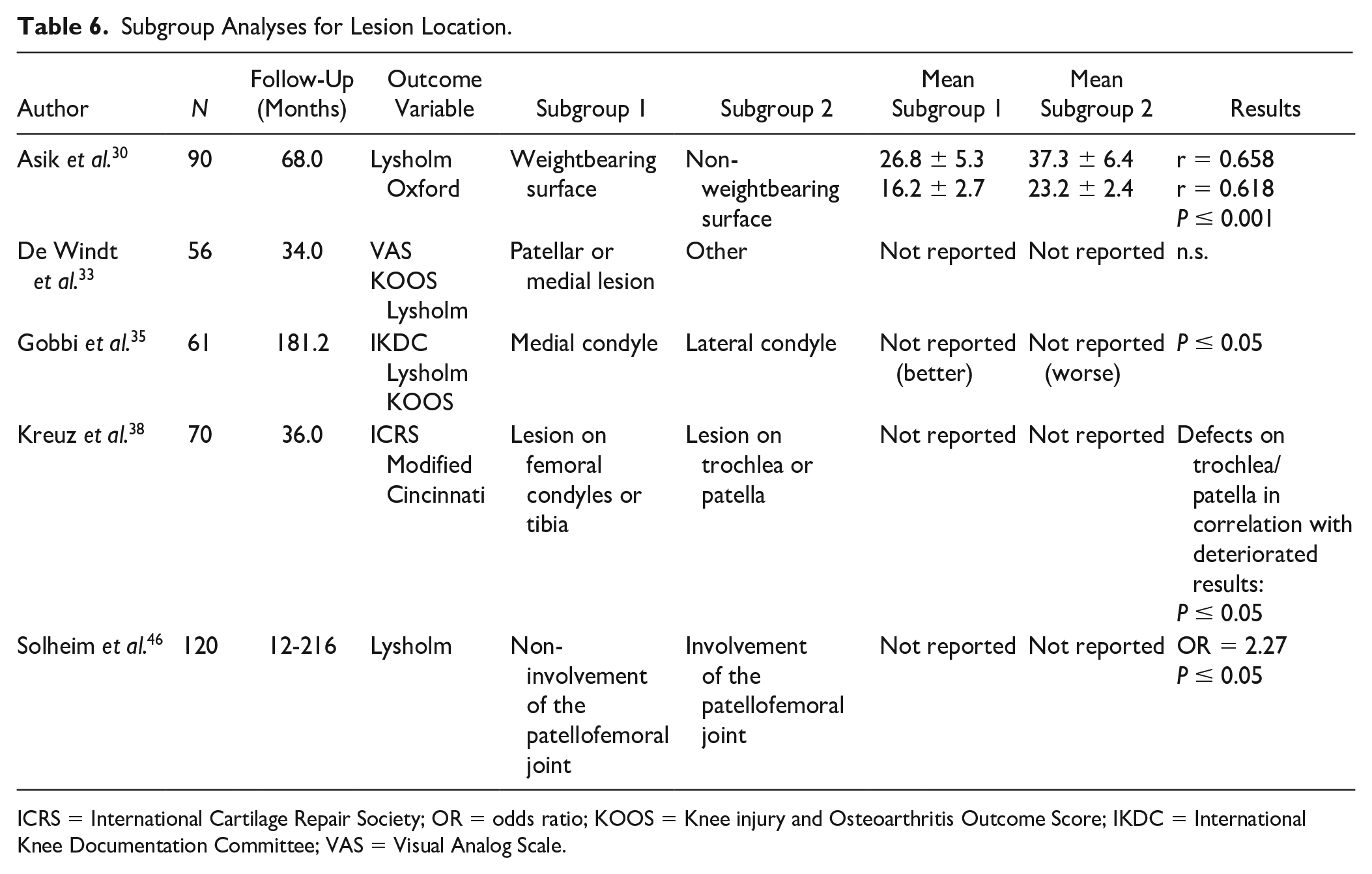
ICRS = International Cartilage Repair Society; OR = odds ratio; KOOS = Knee injury and Osteoarthritis Outcome Score; IKDC = International Knee Documentation Committee; VAS = Visual Analog Scale.
Symptom duration
Seven of the 23 studies researched the influence of symptom duration prior to the surgical treatment, preoperative interval, delayed surgery, and chronicity of the complaints on the postoperative outcome. Four studies researched the correlation between these factors and the PROMs, and one of them found a significant correlation ( Table 7 ). Three subgroup analyses were conducted in which a symptom duration ranging from ≤12 months to <36 months was compared with complaints that were already present for a longer period of time ( Table 8 ). In 2 cases, a significant difference in the effect on PROMs was found. Overall, a shorter duration of symptoms was found to be more beneficial for the outcome.
Correlations for Symptom Duration.
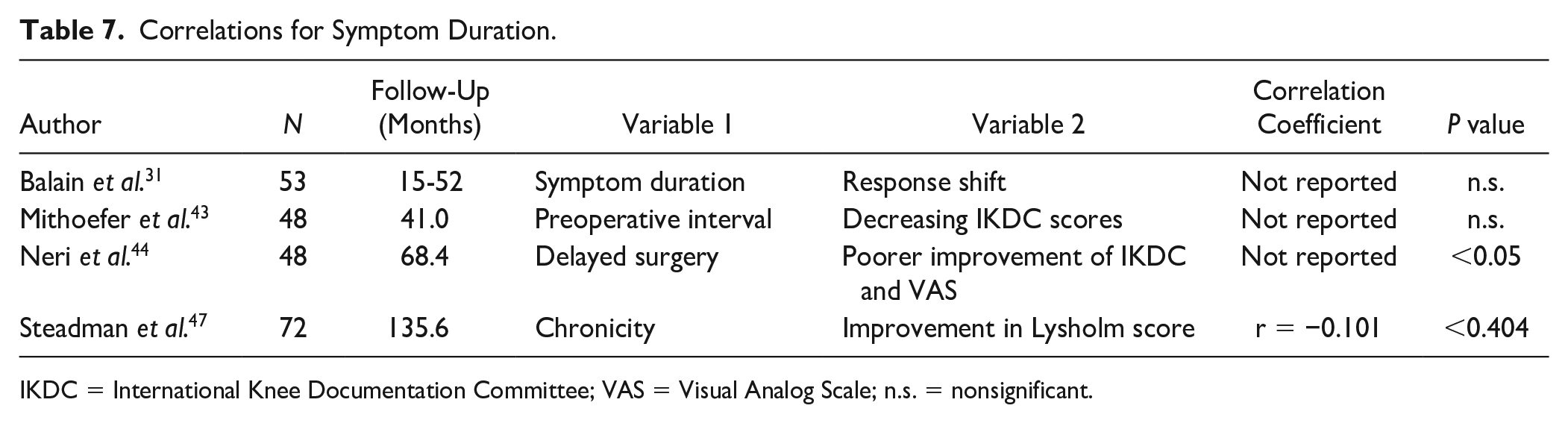
IKDC = International Knee Documentation Committee; VAS = Visual Analog Scale; n.s. = nonsignificant.
Subgroup Analyses for Symptom Duration.
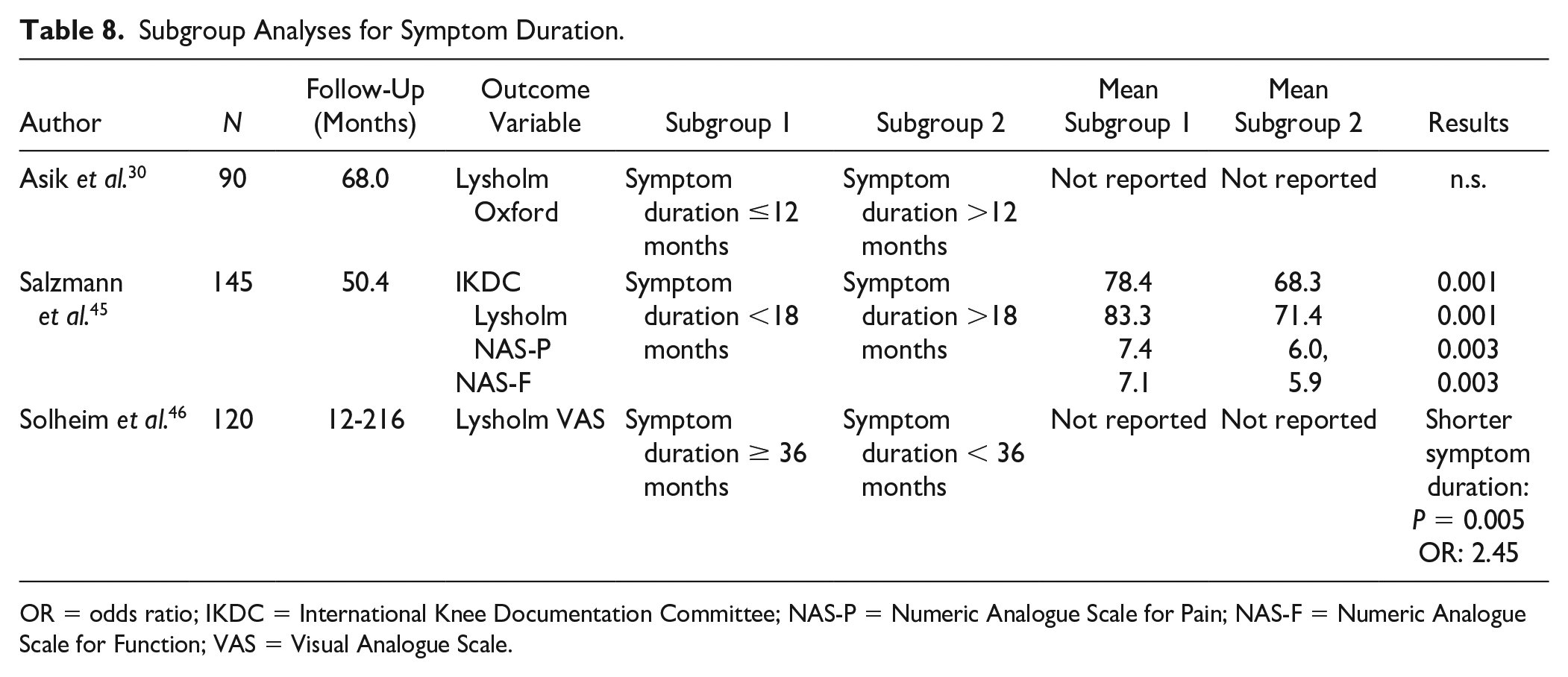
OR = odds ratio; IKDC = International Knee Documentation Committee; NAS-P = Numeric Analogue Scale for Pain; NAS-F = Numeric Analogue Scale for Function; VAS = Visual Analogue Scale.
Gender
Seven studies investigated the influence of gender on the outcome of microfracture. All 7 articles performed subgroup analyses, out of which 2 showed significantly better PROMs at follow-up for male patients in comparison with females ( Table 9 ). Chahla et al. 32 found an odds ratio of 2.7 for males to reach the Patient Acceptable Symptom State (PASS) at 6 months after microfracture. Salzmann et al. 45 found significantly better Lysholm, Knee injury and Osteoarthritis Outcome Score (KOOS), and International Knee Documentation Committee (IKDC) scores for males at an average of 50 months of follow-up. However, a majority of 5 papers did not report significant differences.
Subgroup Analyses for Gender.
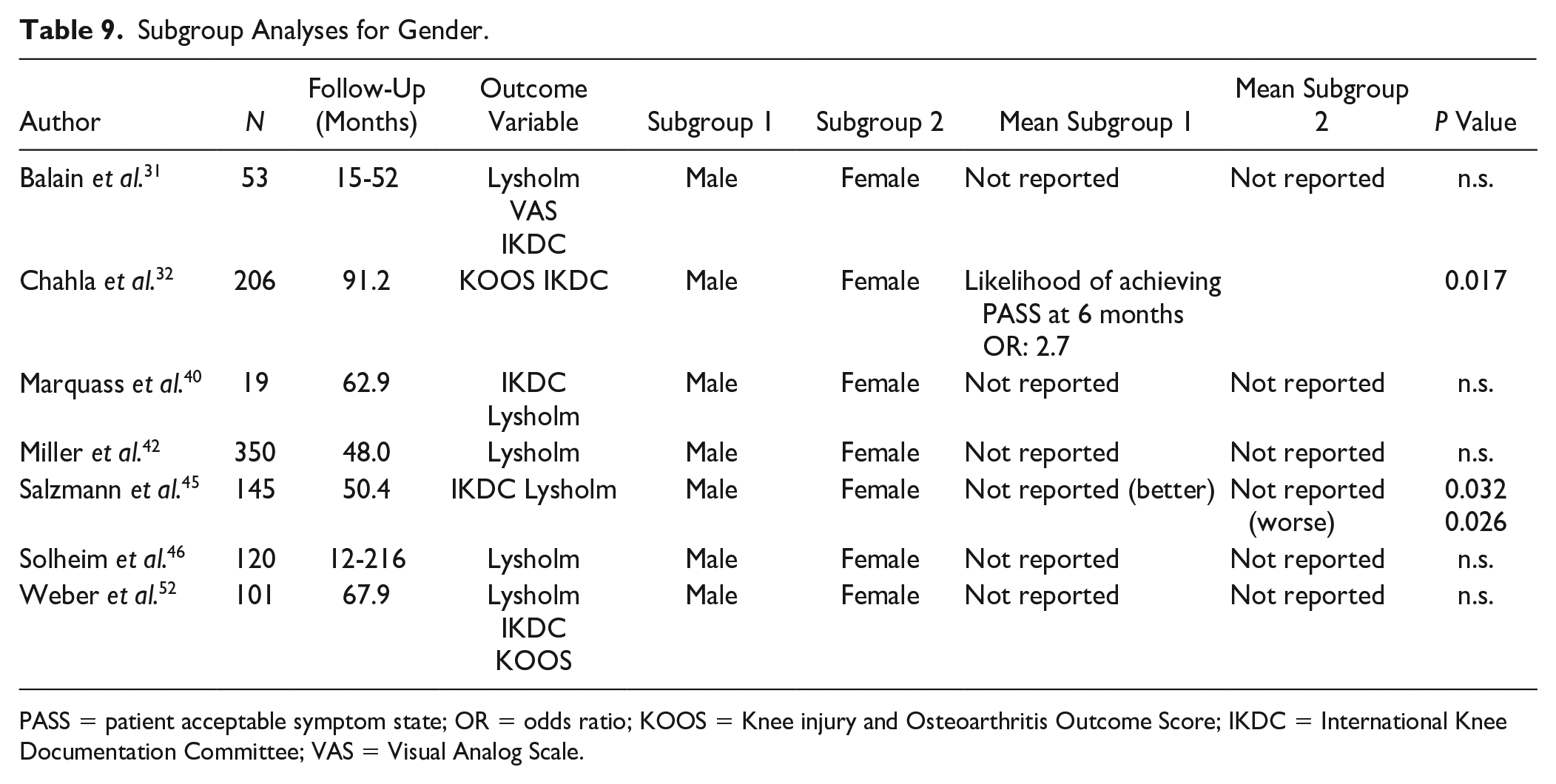
PASS = patient acceptable symptom state; OR = odds ratio; KOOS = Knee injury and Osteoarthritis Outcome Score; IKDC = International Knee Documentation Committee; VAS = Visual Analog Scale.
Other factors and summary
Other prognostic factors that were addressed are defect count, BMI, smoking, concomitant knee surgery, mechanism of injury, previous knee surgery, activity level, and postoperative treatment. The tables displaying the extensive results of these factors can be found in Supplemental Appendix II, with a summary in Table 10 . In short, the studies indicated that the presence of a single cartilage lesion compared with multiple lesions (significant in 3/4 studies) and a BMI <25-30 kg/m2 (3/6) have a beneficial effect on the clinical outcome after microfracture. Patients who have had previous, ipsilateral knee surgery were reported to have worse outcomes in 4 of 6 studies. Little or no evidence was found for the prognostic value of the variables smoking (0/2 significant), concomitant knee surgery (0/2), and the mechanism of injury (1/6).
Summary of Reported Effects.
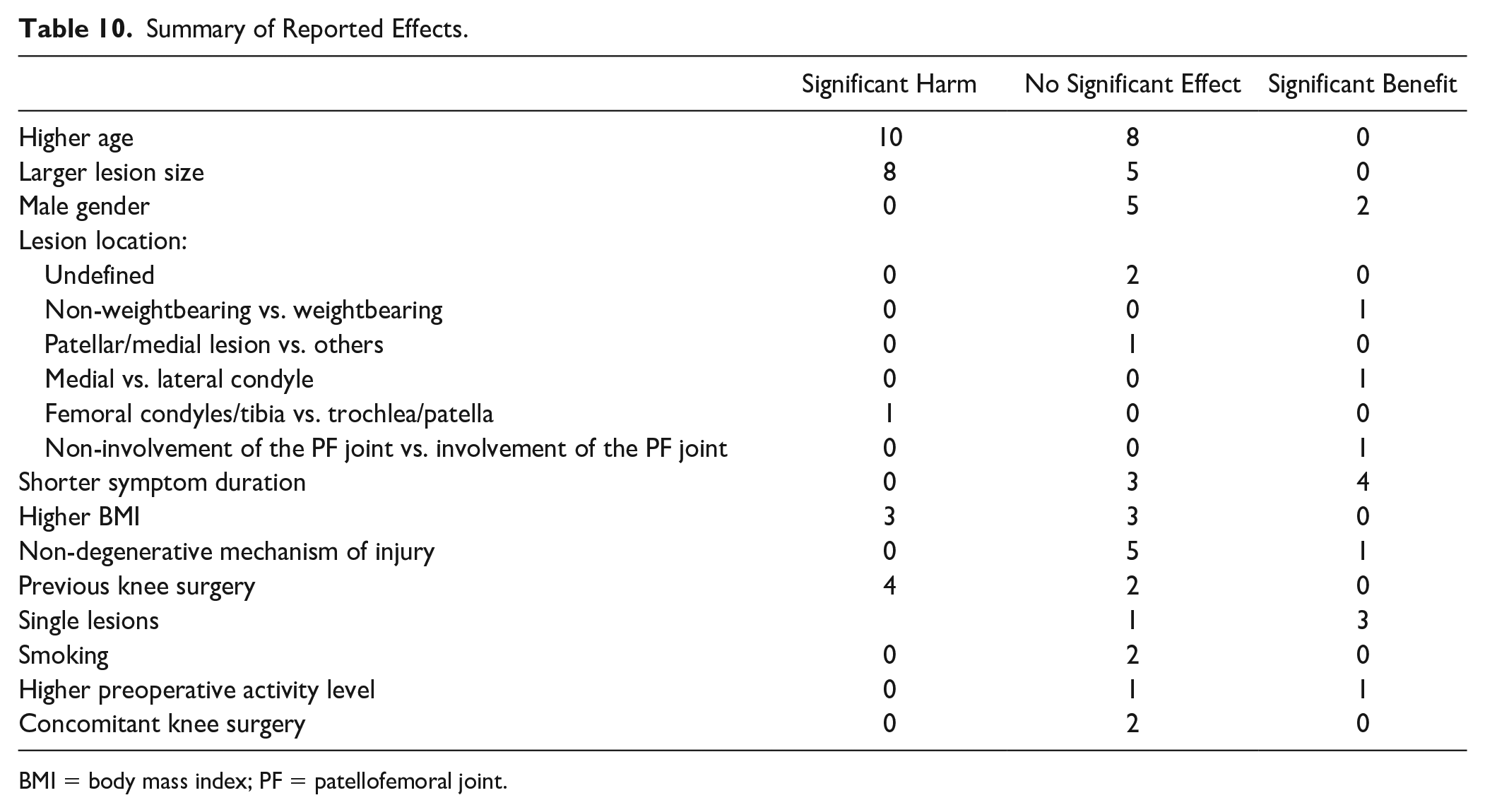
BMI = body mass index; PF = patellofemoral joint.
Discussion
In this systematic review, we identified the prognostic factors that influence the clinical outcome of microfracture surgery of cartilage defects in the knee. A lack of reporting of effect sizes made it impossible to pool the effect of the different variables. However, in a majority of the included studies, it was reported that patient age, lesion size, preoperative symptom duration, previous knee surgery, and lesion count were reported to have a significant effect on the outcome of microfracture. No study reported a significant effect of smoking (out of 2 studies). Conflicting evidence remains for BMI, with 3 studies reporting a significant negative effect and 3 studies stating no effect, and gender, with 3 studies describing a significant benefit for male patients and 4 studies stating no effect.
A harmful correlation between age and clinical outcome comes as no surprise, as with increasing patients’ age, their cell turnover and renewing capacities decline. In the case of articular chondrocytes, older cells exhibit a senescent phenotype. 54 Moreover, advancing age may also impair the joint homeostasis. Taken together, chondrogenesis works insufficiently with increasing age, leading to inferior, fast deteriorating fibrous defect filling which is not able to withstand the so-called pothole effect. 12 On the other hand, in the few studies on the natural history of cartilage defects—that is, untreated—a young age was often associated with stabilization of cartilage defects and high functional outcomes.55,56
A larger lesion size as risk factor is in accordance with biomechanical studies that have shown that defects larger than 2 cm2 increase the load on the base of the defect as well as on the rim. 57 This will potentially negatively influence the development of the repair tissue in the defect and the progression of rim cartilage deformation, resulting in the pothole effect as mentioned before. 58 The same biomechanics apply to lesion location as a prognostic factor. Lesion location showed an effect on the outcome in 4 of 7 mentioned studies, compared with 3 studies showing no significant effect. Particularly, patellofemoral defects have been well known to have inferior outcomes as this compartment endures high compression and shear forces. 59
The effect of BMI on the outcome is inconclusive, with 3 studies showing significant harm (average N = 80) and 3 studies showing none (average N = 71). As BMI is a predictor for osteoarthritis disease development via both mechanical and inflammatory pathways, a negative effect on cartilage regeneration can be expected as well. 60 From a pure mechanical point of view, this holds especially true for patients with a BMI >30 kg/m2, potentially amplifying the effect of concomitant mechanical-based prognostic factors such as defect size larger than 2 cm2. 61
A shorter preoperative symptom duration showed a beneficial effect in 4 of 7 mentioned studies. As already stated, cartilage defects are a well-known risk factor for osteoarthritis development. 4 As osteoarthritis is a whole-joint disease, this transition over time from local to generalized damage can only be explained by a biological process, that is, an impaired joint homeostasis. 62 Indeed, in such impaired environment, cartilage repair is hampered.63 -65 The fact that we found 1 study with beneficial effects for nondegenerative cartilage defects over degenerative defects confirms this rationale. Namely, degenerative defects are probably either older traumatic defects or an early expression of osteoarthritis due to malalignment, for instance. Also, previous surgeries were shown to be harmful in 4 of the 6 studies, again highlighting the importance of a jeopardized/catabolic joint homeostasis. 66
Gender did not show a significant effect on the outcome in 5 of the 7 studies. Two studies showed a better outcome for men, mostly based on subgroup analyses. The use of existing PROMs for comparing differences in outcome between various genders is debatable in general. Women and men may interpret their complaints differently, often resulting in worse outcome for women. 67 Current PROMs do not correct this effect.
As for a higher preoperative activity level, the effect on the outcome is questionable as there was both a study showing an effect by preoperative activity and a study showing no effect.
For smoking, the mentioned studies (average group size N = 99) only specify the absence of a significant correlation between smoking and the response shift and clinical outcome. This is in contradiction to the study of Kraus et al., 68 which found significantly worse postoperative PROMs for smoking patients after arthroscopic partial meniscectomy. We postulate that this difference is perhaps due to more impairment of the micro-vascularization of the meniscus compared with the high blood flow in trabecular bone.
The results for concomitant knee surgery, in both cases reconstruction of the anterior cruciate ligament, found no significant difference. However, we postulate that the results could have been worse without ligament reconstruction due to increasing shear forces on the repair tissue.
Limitations
The limitations of this study lie predominantly in the poor quality and/or absence of the reporting of effect sizes, such as a correlation and an odds ratio. Furthermore, a wide variety of PROMs and outcome measures were used (Visual Analog Scale [VAS], KOOS, Lysholm, IKDC, Oxford, Western Ontario and McMaster Universities Arthritis Index [WOMAC], NAS-P, NAS-F). Combined, it was not possible to pool data and perform a classical meta-analysis. Being unable to pool the data was a limitation in itself. Therefore, the evidence was weighed based on the fraction of papers reporting a significant effect of the prognostic factor. With this approach, a higher risk of bias is unavoidable. Two factors should be considered: especially the smaller sized studies may have been underpowered for the detection of the prognostic factors, as the prognostic factors were rarely the main outcome variable in the studies, and therefore in no study a power analysis was performed for the prognostic factors. Second, for the same reason, a publication bias could be present. While the used PROMs slightly differ, they all aim to measure clinical satisfaction and function of the knee. Therefore, they are highly correlated and are therefore interchangeable in a linear regression analysis. This can also be found in the studies that reported correlations of one factor to multiple PROMs: all results were in agreement. For example, the relation between age and either Lysholm or Oxford score resulted in correlation coefficients of r = 0.623 and r = 0.615, respectively.
Recommendations
Most factors that are discussed above may already be in consideration in standard practice. Therefore, it is surprising that there is little research specifically aimed at testing these assumptions. That the results confirm the general assumptions could therefore also be enhanced by publication bias. This may be partly due to the large variations between patients, as cartilage defects often present with concomitant injuries. This makes it difficult to isolate prognostic factors. For the future, more research dedicated at investigating the impact of prognostic factors, optimally in larger cohorts, on clinical outcome is highly recommended. Furthermore, reportage of effect sizes should be standard practice to enable meta-analysis. Larger registries that combine data from various sources, such as the German Knorpel Register, could be used in future validation studies. 69 The results from this review can be used to determine the variables of interest.
The results of this review indicate that the best prognosis for microfracture is for patients with cartilage defects smaller than 2 cm2, situated on the medial femoral condyle, that are of nondegenerative origin in healthy normal-weight patients younger than 40 years with less than 12 months of complaints. In clinical practice, this is a rare encounter. However, the alternatives (either conservative or with other surgical techniques) may share up until some extend the same risk factors. Comparative studies may therefore need to differentiate in population to find the best treatment for each subgroup and with increasing data availability work toward individual treatment advises. Ultimately, combining large-scale data collections with advanced data analysis holds the premise of fine-tuning the treatment algorithms based on patient factors, lesion characteristics, and clinical indications.
Finally, one of the key messages and recommendations which follows from this article is to emphasize the importance of the reporting of effect sizes, also for secondary outcome measure analysis.
Conclusion
In conclusion, the overall evidence regarding prognostic factors and their influence on clinical outcome is incomplete and possibly influenced by bias.
However, based on the reported evidence, the best prognosis after microfracture is for patients with lower age, smaller lesion size, a shorter preoperative symptom duration, a nondegenerative mechanism of injury, and a single lesion. Patients of previous surgery on the ipsilateral knee, especially meniscectomy and anterior cruciate ligament reconstruction, were indicated to be at risk. Taken together, the indication to perform microfracture is perhaps much smaller than reflected by current clinical practice. As to lesion location, gender, BMI, preoperative activity level, smoking, and concomitant knee surgery, the included articles are inconclusive or there is a lack of evidence. To determine effect sizes, better reporting is needed.
This study also highlights the need for collaboration on national and international level in the form of registries to generate larger data sets concerning cartilage repair.
Supplemental Material
sj-docx-1-car-10.1177_19476035221147680 – Supplemental material for Prognostic Factors for the Clinical Outcome after Microfracture Treatment of Chondral and Osteochondral Defects in the Knee Joint: A Systematic Review
Supplemental material, sj-docx-1-car-10.1177_19476035221147680 for Prognostic Factors for the Clinical Outcome after Microfracture Treatment of Chondral and Osteochondral Defects in the Knee Joint: A Systematic Review by Iris M. van Tuijn, Kaj S. Emanuel, Pieter P.W. van Hugten, Ralph Jeuken and Pieter J. Emans in CARTILAGE
Footnotes
Authors’ Note
This research was conducted at the Department of Orthopedic Surgery of Maastricht University Medical Center+.
Acknowledgments and Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: K.S.E. is supported by the Dutch Research Council (NWO) domain Applied and Engineering Sciences (P15-23).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This systematic review was registered in PROSPERO on the 19th of June 2021 (id: CRD42020177512).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.