
Abstract
Objective
The use of perinatal-derived tissues and mesenchymal stromal cells (MSCs) as alternative treatment options to corticosteroid and hyaluronic acid injections has been gaining popularity. However, their ability to attenuate osteoarthritic (OA) symptoms while also slowing the progression of the disease remains controversial. Thus, the objective of this article is to summarize the results from both preclinical and clinical studies evaluating the efficacy of perinatal-derived tissue allografts and MSCs for the treatment of OA.
Design
A comprehensive literature search was conducted on databases including Pubmed, ScienceDirect, and Google Scholar beginning in March 2020 for both preclinical and clinical studies evaluating perinatal-derived tissues and MSCs in OA. Eighteen studies met the inclusion criteria and were used for this review.
Results
Both animal models and early human clinical trials demonstrated that perinatal tissues could reduce joint inflammation and pain as well as improve range of motion and function in OA. Perinatal tissue–derived MSCs in animal studies have shown the potential to support chondrocyte proliferation while also decreasing inflammatory gene and protein expression. Limited clinical results suggest perinatal tissue–derived MSC sources may also be a viable alternative or adjunct to hyaluronic acid in reducing pain and symptoms in an arthritic joint.
Conclusions
Perinatal tissue–derived allografts and MSCs have promise as potential therapeutics for mitigating OA progression. However, further research is warranted to fully define the therapeutic mechanism(s) of action and safety of these biological therapies.
Introduction
Overview
Osteoarthritis (OA) is a common disease in older populations and is characterized by the degeneration of joint cartilage and changes to the underlying bone. Major factors contributing to OA progression include proinflammatory cytokines, reactive oxygen species (ROS), matrix-degrading enzymes, changes in biomechanical stress, and age.1,2 Currently, conservative treatment options for OA focus on relieving symptoms, yet disease-modifying therapies that halt or slow progression are limited. Newer treatments, such as those that incorporate perinatal tissue–derived allografts and mesenchymal stromal cells (MSCs), are currently under investigation for their ability to favorably modify the joint environment and reduce OA mediators. Thus, the major aims of this review are to introduce the anatomy and composition of perinatal tissues, summarize results of basic science and clinical studies that evaluate the efficacy of perinatal tissue–derived allografts or MSCs as treatments for OA, and identify gaps in knowledge and/or limitations in current studies to inform future research directives.
Clinical Significance of OA
OA is a disease that disabled 63 million individuals in 2020 and is estimated to affect 78 million by the year 2040 (Centers for Disease Control and Prevention). 3 An increase in OA-inducing factors, such as obesity and longer life span, may contribute to the increase in OA prevalence. As the average human lifespan approaches 80 years, it is notable that the incidence of OA increases dramatically between the ages of 40 and 70 years, 4 and 40% of Americans aged 70 or older are affected by this disease. 5 While OA can significantly affect a patient’s quality of life, it can also pose large financial burdens on these individuals, the health care system, and society. 3 The total national arthritis-attributable medical expenditures were estimated to be $139.8 billion, with all-cause expenditures among adults with arthritis representing 50% of the $1.2 trillion national medical expenditures among all adults (2013 US Medical Expenditure Panel Survey). 6
The Pathology of OA
While cartilage degradation and pain are often associated with OA, this disease affects the entire synovial joint including the synovial fluid, synovial membrane, and subchondral bone. The exact cause that initiates degradation is unknown, but it is theorized that a trauma to the joint may lead to the production of extracellular matrix (ECM) wear particles, also known as damage-associated molecular patterns (DAMPS).7,8 DAMPS bind to receptors on chondrocytes and macrophages within the cartilage and synovium, respectively, causing them to increase the production of proteases (e.g., matrix metalloproteinases [MMPs] and a disintegrin and metalloproteinase with thrombospondin motifs [ADAMTS]) and proinflammatory cytokines including interleukin (IL)-1β, IL-6, IL-8, and tumor necrosis factor (TNF)-α.8-10 These cytokines can also cause the chondrocytes to decrease their production of cartilage ECM, which further disrupts joint tissue homeostasis and promotes cartilage degradation. 11 While OA has historically been thought of as a degenerative disease of cartilage, research from the past 10 years has shown OA to be a multifactorial disease that is influenced by chronic inflammation. 12 This indicates that OA involves non-biomechanical factors such as those related to lipid metabolism, which play a proinflammatory role by enhancing the production of MMPs, as well as gut microbiota, which influences the progression of OA by affecting or interacting with the body’s immune system.12,13
Methods
A comprehensive search was conducted on PubMed, ScienceDirect, and Google Scholar databases beginning in March 2020 using the following combination of terms:
Amniotic Membrane: “osteoarthritis” AND “amniotic membrane” OR “amnion” OR “amniotic suspension allograft” OR “amniotic MSCs”
Chorionic Membrane: “osteoarthritis” AND “chorionic membrane” OR “chorion” OR “chorion MSCs”
Umbilical Cord: “osteoarthritis” AND “umbilical cord” OR “umbilical cord MSCs”
Amniotic Fluid: “osteoarthritis” AND “amniotic fluid” OR “amniotic fluid stem cells” OR “amniotic fluid MSCs”
Inclusion criteria for relevant articles were the following: written in English language, full-text articles available, and primary articles evaluating preclinical or clinical studies on perinatal tissue–derived or MSC-derived treatments for OA. Exclusion criteria included studies on knee pathologies other than OA, no available abstracts or full texts, languages other than English, and focus on joints other than patellofemoral. Relevant data such as type of treatment, treatment dosage, primary and secondary outcomes, and overall conclusions were collected and subsequently compiled in this review.
Current Treatment Strategies for OA
Overview of Treatment Strategies
Current treatment strategies for OA range from conservative medications, such as nonsteroidal anti-inflammatory drugs (NSAIDs), to surgical intervention. Oral NSAIDS are often used for short-term pain relief because their extended use is known to negatively impact the gastrointestinal tract and can be nephrotoxic.14,15 Another common method for short-term relief of OA is an intra-articular injection of corticosteroids. These local injections have fewer systemic side effects and have demonstrated the ability to decrease inflammation and pain levels 16 ; however, the evidence regarding long-term efficacy of these treatments is limited, 17 and in vitro and in vivo evidence has shown that cortisone injections are chondrotoxic with dose-dependent deleterious effects on cartilage. 18 Similarly, viscosupplementation, involving intra-articular hyaluronic acid (HA) injections, is used in an attempt to improve joint lubrication.19,20
Biological Therapies on the Rise as New Treatment Options for OA
Biological therapies are attractive alternatives to current treatments because they are thought to have potential disease-modifying properties. There is a growing role for biologic therapies for OA to provide noninvasive pain relief while also attempting to modify or delay the progression of OA. Platelet-rich plasma (PRP) is a commonly studied autologous biologic therapy used for the management of OA. Gato-Calvo et al. compared randomized controlled trials that evaluated the efficacy of PRP injections. Most evidence suggested that PRP injections were able to improve pain scores at 6 and 12 months post-injection; however, they concluded the overall level of evidence was low and that the efficacy of PRP injections is still under debate. 21 Autologous adipose-derived mesenchymal stromal cells (AD-MSCs) have also gained popularity as a potential OA treatment.22,23 A double-blind, randomized controlled clinical trial demonstrated that a single intra-articular injection of AD-MSCs led to significant improvements in Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) scores and prevented the worsening of cartilage defects at 6 months versus the control group. 23 In addition, MSC-containing bone marrow aspirate concentrate (BMAC) has been examined for its role in OA treatment and has noted short-term beneficial effects such as significant improvements in pain and function. 24
While these autologous products are an intriguing option, their potency and effectiveness are often limited by patient health and age, which may affect the quality of the autologous products harvested. An alternative source of biologic-based therapeutics includes perinatal tissue allografts, which contain an abundance of anti-inflammatory and pro-regenerative growth factors, ECM components, and other active biomolecules that can aid in the body’s natural healing process. 25 Similarly, perinatal tissue–derived MSCs are currently undergoing preclinical investigations as a potential therapeutic for OA due to their ability to alter the local chemical microenvironment of the joint, provide protection to chondrocytes, and manage local inflammation.26-29 Thus, the remainder of this review will focus on highlighting the preclinical and clinical findings employing perinatal tissue–derived allografts and MSCs and their potential as a therapeutic benefit.
Overview of Perinatal Tissues
Anatomy of Perinatal Tissues
Perinatal tissue is an overarching term encompassing the different tissues that comprise the placenta and umbilical cord between the 20th week of gestation and the neonatal period (Fig. 1). 30 The placenta and umbilical cord are temporary organs that form during pregnancy and play a crucial role in the development of the fetus.
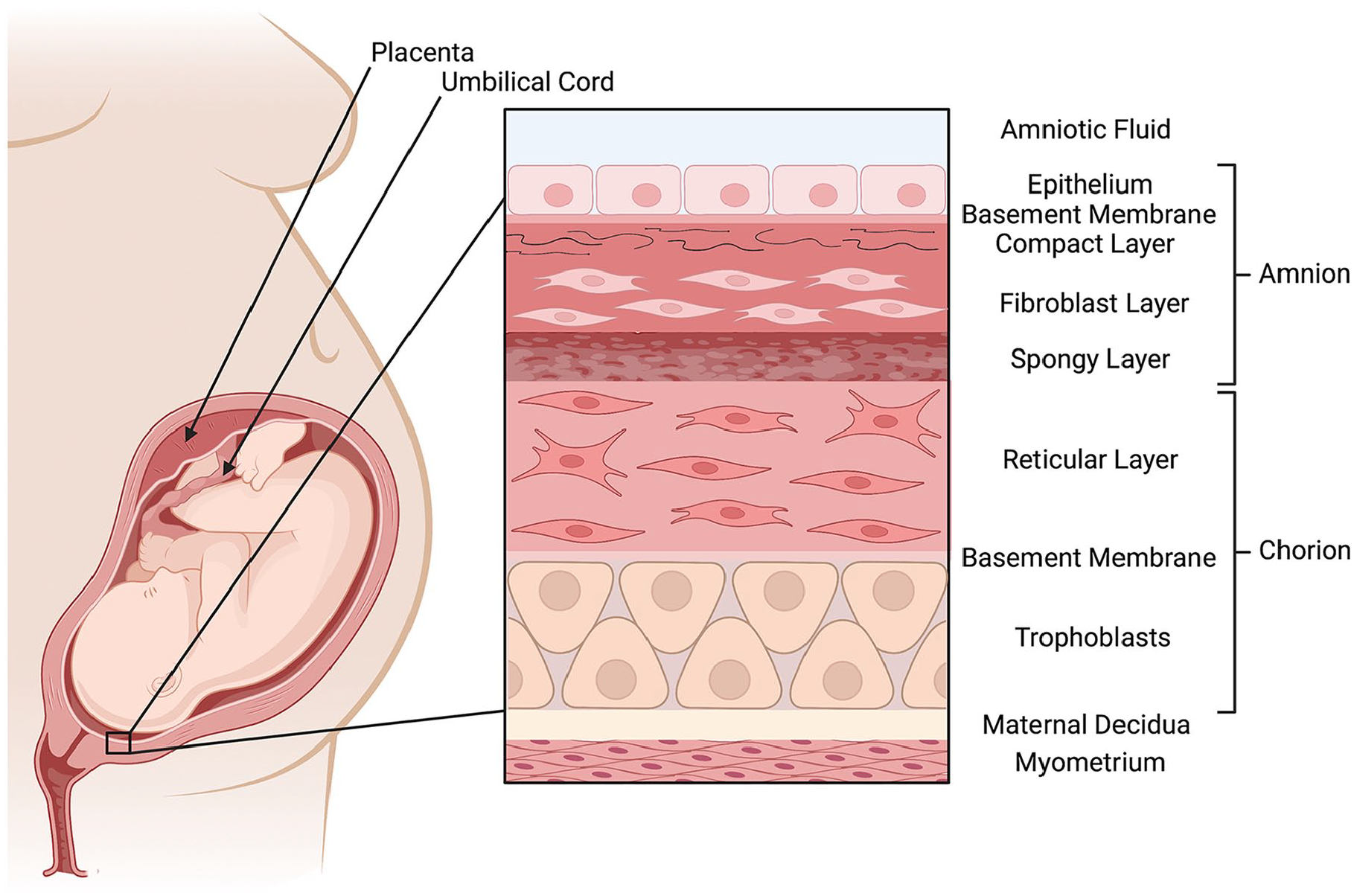
Anatomical location of perinatal tissues.
The surface of the placenta that faces the fetus is the chorionic plate, which is composed of the amniotic and chorionic membranes. These membranes provide an attachment site for the umbilical cord while also enclosing the fetus in a cavity filled with a protective/cushioning substance—amniotic fluid (AF). The space between the maternal component of the placenta and the fetal membranes is where maternal blood interacts with fetal blood via the chorionic villi. 31 The umbilical cord vessels also participate in fetal-maternal circulation and are encompassed by a gelatinous and proteoglycan-rich ECM known as Wharton’s jelly.
Amniotic membrane
The amnion is the thin, inner lining of the placenta that is composed of 5 different layers including the epithelium, basement membrane, compact layer, fibroblast layer, and spongy layer. 32 These layers are known to contain type I and IV collagens, fibronectin, laminin, proteoglycans, HA, and glycoproteins.33-35 The amniotic membrane (AM) and its cells function in providing mechanical support, 34 regulating the pH of AF, synthesizing growth factors, cytokines, and vasoactive peptides, 36 while also providing an immunoprivileged barrier between the mother’s immune system and the fetus.
Chorionic membrane
The chorion is the outermost fetal membrane; it is 4 times thicker than the amnion and is composed of a layer of trophoblast cells and a reticular layer separated by a basement membrane. Its proximal mesodermal layer and distal layer of trophoblast cells help to provide mechanical strength to the fetal membranes. 37 Components of the chorion ECM include type I and IV collagens, along with fibronectins and laminins. 34 Because of its thickness, the fresh and dehydrated chorion membrane is believed to contain more growth factors and cytokines than fresh or dehydrated amnion.25,38
Umbilical cord tissues
The umbilical cord is a 50- to 60-cm-long conduit that transports deoxygenated blood from the fetus to the placenta. It is composed of 3 vessels (2 arteries and 1 vein), Wharton’s jelly surrounding the vessels, and a thin, outer lining composed of mesenchymal and epithelial cells. 39 Wharton’s jelly is a mucopolysaccharide that is composed of HA and chondroitin sulfate, and functions to insulate and protect the umbilical vessels. 40
Amniotic fluid
The primary function of AF is to cushion and protect the fetus and umbilical cord from both trauma and compression.41,42 In addition, AF is known to provide essential nutrients such as proteins, electrolytes, immunoglobulins, vitamins, and growth factors to ensure normal development of different organ systems of the fetus.43,44 It has also been shown to contain MSCs.
Studies Evaluating the Therapeutic Efficacy of Injectable Perinatal Tissue Allograft Suspensions for OA
Preclinical Studies
Amniotic membrane
The efficacy of intra-articular injections of particulated human AM in preventing cartilage destruction has been evaluated in a rabbit model of OA. 45 On days 0 and 4, both knees of 6 New Zealand rabbits underwent intra-articular injections of type II collagenase to induce OA. After OA was established, the rabbits were divided into 2 treatment groups, where each rabbit received intra-articular injections of lyophilized and pulverized human AM (0.040 mg/0.200 ml) in the right knee and injections of saline solution (0.6 ml) in the left knee as a control. At 3 and 6 weeks, AM treatment prevented macroscopic changes to the cartilage along with protecting the ECM from destruction, as illustrated by intact cartilage surfaces that demonstrated continuity with less deformity and fibrillation compared with untreated controls. 45
In addition, employ a rat monosodium iodoacetate (MIA) model of OA, an amniotic suspension allograft (ASA) composed of AF and particulated AM. ASA treatment yielded significant improvements in pain and swelling, with reductions in weightbearing differences compared with the control group. 46 The reduction in swelling observed indicated that the ASA mitigated joint inflammation. This was confirmed through synovial fluid analysis, which revealed reduced levels of IL-6 and significantly increased levels of IL-10. 46
Chorionic membrane
Human chorion has been combined with amnion in an injectable, micronized form (μ-dHACM) that has been shown to have protective effects in a post-traumatic OA model in rats. 47 Twenty-four hours after undergoing medial meniscal transection (MMT) surgery to induce OA, Lewis rats were treated with intra-articular injections of either μ-dHACM or saline into the stifle joint of the left leg. The μ-dHACM demonstrated higher proteoglycan levels and fewer cartilage erosions / lesions. 47 In addition, allograft particulates were found to be present within the synovial membrane for at least 21 days post-injection. 47
Umbilical cord
The effect of intra-articular injection of an amnion/umbilical (AM/UC) cord suspension on cartilage degeneration was evaluated in a rat post-traumatic OA model. 48 Two weeks after MMT surgery, rats received intra-articular injections of 50 µg/µL AM/UC, 100 µg/µL AM/UC, or a saline control. Equilibrium Partitioning of an Ionic Contrast agent via microcomputed tomography (EPIC-μCT) demonstrated that overall cartilage destruction and total lesion area were reduced in the treatment groups compared with saline. Significantly greater cartilage thickness and volume for both doses were observed at 1 week compared with the saline-injected joints, while only the high dose demonstrated positive results at 4 weeks post-injection. 48
Clinical Studies
Amniotic membrane
There are few clinical studies evaluating the safety and efficacy of perinatal tissues for the treatment of OA. The first randomized controlled trial to investigate ASA for OA was completed in 2019 and compared the use of single injections of ASA, HA, and saline over a 6-month period. 49 Eligible patients involved in this trial were 18 years or older, with a body mass index (BMI) of <40 kg/m2, diagnosed with moderate knee OA (grade II or III on the Kellgren-Lawrence [KL] score), and had a 7-day average pain score of 4 or greater on a scale of 1 to 10. The treatment groups involved in this trial included: an ASA treatment group consisting of 68 patients with a mean age of 55.9 ± 12.3 years, an HA treatment group consisting of 64 patients with a mean age of 55.4 ± 11.0 years, and a saline group consisting of 68 patients with a mean age of 54.9 ± 9.9 years. The investigators found that ASA injections were superior to HA and saline in almost every patient-reported outcome measure, as well as there were notable improvements in range of motion, activities of daily living, pain, and symptoms. 49
In continuation of this study, a separate report was published with data up to a 12-month follow-up. 50 Their main endpoints were to assess improvements in both pain and function through patient-reported outcomes, including Knee Injury and Osteoarthritis Outcome Score (KOOS) and visual analog scale (VAS) score at baseline, 1-week, 6-week, 3-month, 6-month, and 12-month time points. 50 Results showed that ASA injections in symptomatic patients resulted in significant improvements out to 12 months in the KOOS subscales and VAS scores compared with HA and saline with no concerning immunological or adverse reactions. 50 However, no differences between groups for radiographic measures in the index knee were observed. To date, multiple other clinical studies using ASA have been completed or are currently underway, with results yet to be published.
In addition, an open-label feasibility study was performed on 6 patients to evaluate the safety and efficacy of ASA injections for knee OA. 51 This study followed patients for 12 months after treatment, finding that ASA injections did not cause any adverse changes in the patients’ renal function, blood cell counts, or lymphocyte subgroups. Based on this, and the improvements observed in patient-reported outcomes for pain, symptoms, and quality of life, the authors concluded that a single intra-articular ASA injection was safe for clinical use. This study was performed in anticipation of a larger, blinded trial to determine the efficacy of ASA treatments. 51
Chorionic membrane
The only study published to date that employs the chorion is a case series of 40 patients with a mean age of 50.7 ± 12.4 years. 52 Twenty of these patients were treated for OA of joints, including the knee, tibiotalar, subtalar, glenohumeral, cervical facet, and femoroacetabular joints, whereas the other 20 patients were treated for tendon pathologies that included common extensor tendons at the elbow, supraspinatus tendons, conjoint hamstring tendons, gluteus medius tendons, patellar tendons, Achilles tendon, fibularis longus tendon, and iliopsoas tendon. The authors demonstrated that ASA containing particulated amnion and chorion is effective in reducing pain and restoring function in patients with tendonitis or arthritis without any adverse events or side effects. 52
Umbilical cord
A 2019 pilot study evaluated the short-term safety and efficacy of AM/UC allografts versus HA injections in managing pain in knee OA patients with different degrees of disease severity based on bone marrow lesions (grades 0-3). 53 In this study, 20 patients aged 71.0 ± 6.4 years received ultrasound-guided intra-articular injections of 50 mg of AM/UC particulate reconstituted in saline. The patients were monitored at 6, 12, and 24 weeks post-injection. Of note, patients who did not show a greater than 30% reduction in pain by 6 weeks received a second injection at the follow-up. The study demonstrated significantly decreased levels of pain from baseline to 24 weeks and was associated with significant improvements in physical function as indicated by improved WOMAC scores. 53 This study also revealed patients with severe bone marrow lesions were more likely to show improvement after AM/UC injection, which differed from the HA study group. Single injections were sufficient in controlling pain as early as 6 weeks in nonobese patients, whereas 7 of the 8 obese patients required a second injection to experience reductions in pain by 12 weeks. 53 However, these effects were short-lived in obese patients as all WOMAC scores regressed, suggesting AM/UC treatments might not be as effective in this patient population.
Amniotic fluid
Studies are being performed to analyze the ability of AF to treat OA compared with HA injections because of AF’s native cushioning and lubricating functions. One of the first studies compared the long-term effects of freshly collected AF in a group of 26 patients with a mean age of 49 ± 6.4 years versus a triamcinolone acetonide (40 mg in 10 ml) steroid treatment group consisting of 26 patients with a mean age of 51.4 ± 4.6 years. Presenting only anecdotal data, the study showed that AF injections were superior to conventional steroid treatments through sustained pain relief and greater patient satisfaction. 54
Taken together, preclinical and clinical findings suggest that perinatal tissue allografts do demonstrate varying degrees of efficacy ( Tables 1 and 2 ). It is believed that the primary therapeutic mechanism of action is largely due to the anabolic growth factors and anti-inflammatory cytokines deposited within the ECM by resident MSCs, as most commercially available perinatal tissue allografts that are not cryopreserved do not contain viable MSCs.55,56 This is due to the processes required to manufacture them, which often includes rinsing and washing to remove excess blood, air drying or freeze drying to make the grafts shelf stable, sterile filtration (for AF), and the use of different terminal sterilization techniques. Despite these techniques rendering perinatal cells nonviable, these cells, including their cellular and pericellular components, may remain intact and can play essential roles in regulating biological activity. 57 As a result, there is interest in evaluating the potential efficacy of perinatal tissue–derived MSCs themselves or extracts derived from cells as an OA treatment.
Summary of Preclinical Studies Evaluating the Efficacy of Perinatal Tissue Allografts to Mitigate OA.
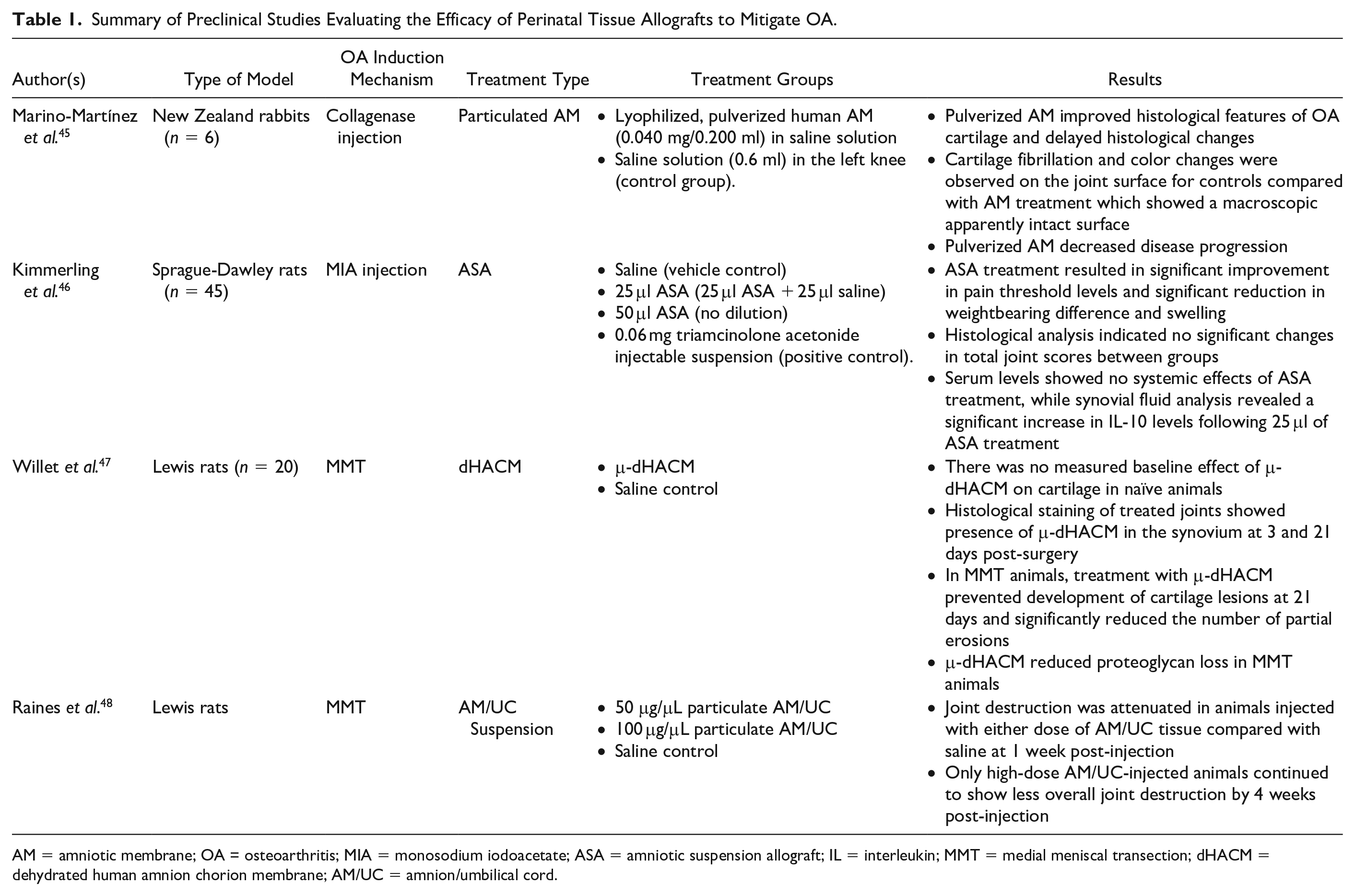
AM = amniotic membrane; OA = osteoarthritis; MIA = monosodium iodoacetate; ASA = amniotic suspension allograft; IL = interleukin; MMT = medial meniscal transection; dHACM = dehydrated human amnion chorion membrane; AM/UC = amnion/umbilical cord.
Summary of Clinical Studies Evaluating the Efficacy of Perinatal Tissue Allografts to Mitigate OA.
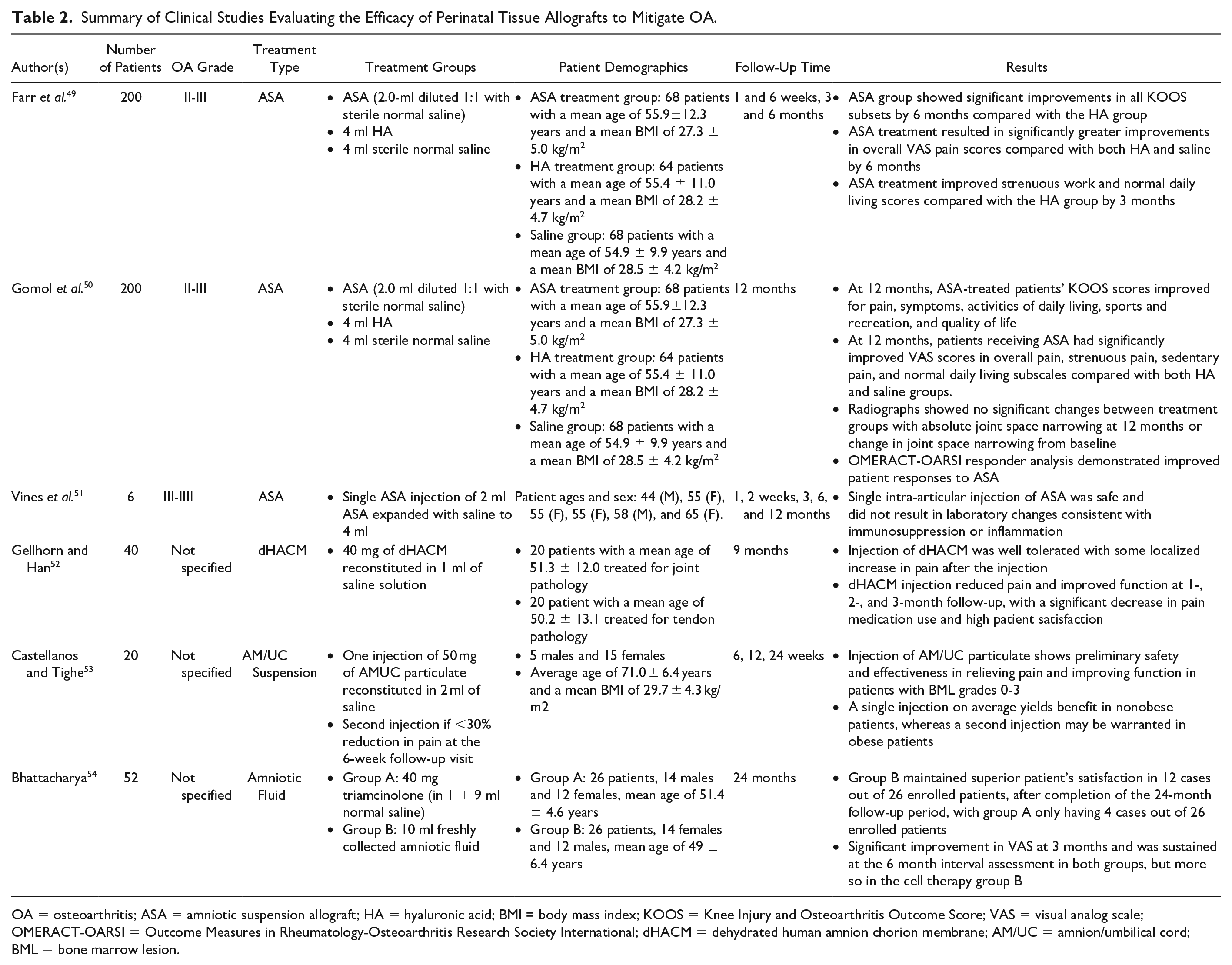
OA = osteoarthritis; ASA = amniotic suspension allograft; HA = hyaluronic acid; BMI = body mass index; KOOS = Knee Injury and Osteoarthritis Outcome Score; VAS = visual analog scale; OMERACT-OARSI = Outcome Measures in Rheumatology-Osteoarthritis Research Society International; dHACM = dehydrated human amnion chorion membrane; AM/UC = amnion/umbilical cord; BML = bone marrow lesion.
Overview of Perinatal Tissue–Derived MSCs
Tissues isolated immediately following delivery (including amniotic and chorionic membranes, AF, and umbilical cord) have been shown to contain viable MSCs ( Fig. 2 ). MSCs derived from these tissues have been found to be highly angiogenic, antifibrotic, and antimicrobial and demonstrate immune-privileged properties.29,32,44,58 Such MSCs have also shown pluripotent characteristics, as well as the ability to help preserve local tissues.53,54 Furthermore, perinatal tissue–derived MSCs can be isolated in significantly greater quantities,30,59,60 with no donor site morbidity or ethical concerns compared with other MSC sources. 61 In addition, compared with adult MSCs, perinatal tissue–derived MSCs do not form teratomas,30,62 secrete more anabolic growth factors, 63 exhibit greater pluripotency capability, 30 have higher immunosuppressive capacity, and have superior angiogenic capabilities. 64 With these unique characteristics and advantages, perinatal MSCs have shown great potential in areas of regenerative medicine, representing a potential treatment option for OA.
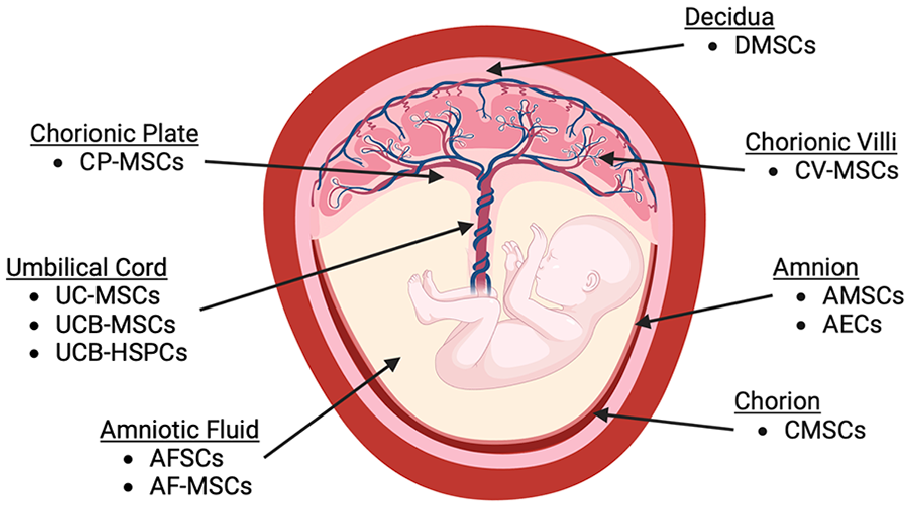
Schematic representing the sources of perinatal MSCs. AMSCs = amniotic membrane mesenchymal stromal cells; AEC = amniotic membrane epithelial cells; CMSCs = chorionic membrane mesenchymal stromal cells; CP-MSCs = chorionic plate mesenchymal stem cells; CV-MSCs = chorionic villi mesenchymal stromal cells; AFSCs = amniotic fluid stem cells; AF-MSC = amniotic fluid mesenchymal stromal cells; UCB-HSPCs = umbilical cord blood hematopoietic stem/progenitor cells; UCB-MSCs = umbilical cord blood mesenchymal stromal cells; UC-MSCs = umbilical cord mesenchymal stromal cells; DMSCs = decidua-derived mesenchymal stromal cells.
Perinatal MSCs’ Preclinical Data
Amniotic membrane MSCs
While the healing effects of amnion-derived MSCs and HA have been investigated separately, the combined effect of these treatments has not been explored until recently. Wang et al. evaluated the effects of human amniotic mesenchymal stromal cells (hAMSCs) and HA to treat knee MIA-induced OA in a rat model. 43 Their results illustrated that this combination treatment could significantly impact cartilage regeneration. Fifty-six days post-injection, injured cartilage was significantly regenerated, yielding results comparable to those of normal cartilage levels. 43 These results were attributed to HA’s ability to assist hAMSCs in chondrogenic differentiation, proliferation, colonization, and regenerative modulation, as the combined treatment showed an improved therapeutic effect than either of the individual treatments.
Utilizing an in vitro model, Topoluk et al. found that direct contact co-culture of human hAMSCs on explants of human osteoarthritic cartilage and synovium demonstrated higher chondrocyte viability and heightened alleviation of cartilage destruction compared with human adipose stromal cells (hADSCs). 27 After 15 days of direct culture, chondrocyte viability in the cartilage biopsies was significantly decreased in both OA and hADSC groups, while chondrocyte viability was maintained with the hAMSC-treated group. hAMSCs were also able to improve mean OARSI histological scores for the treated cartilage biopsies and more effectively shifted synovial macrophages toward a pro-regenerative M2 phenotype compared with hADSC-treated explants. In addition, safranin-O staining demonstrated that hAMSC-treated cartilage biopsies had less surface fibrillation and darker staining of aggrecan than that of hADSCs, as well as significantly more glycosaminoglycan (GAG) content. 27 This study’s findings indicated that hAMSCs may be more effective in chondroprotection in the OA microenvironment compared with hADSCs.
Umbilical cord MSCs
A cell co-culture study was used to explore the interaction and therapeutic potential of UC-MSCs with OA-degenerated chondrocytes. 65 Isolated human OA chondrocytes were split up into 2 different experimental groups: a control group with chondrocytes cultured in normal medium and a co-culture group with chondrocytes grown in supernatant from UC-MSCs. After culture, the experimental group illustrated significantly higher chondrocyte proliferation rates and significant decreases in expression of genes related to inflammation and matrix degradation (COX-2, MMP13, and collagen Xα1). 65 The supernatant for the experimental group was also collected and demonstrated lower levels of proinflammatory cytokines (TNF-α, IL-1β, IL-6). 65 These results indicate that UC-MSCs in vitro were able to mediate the inflammatory response of OA chondrocytes while also promoting their proliferation through their secretome.
Similarly, Tong et al. studied the therapeutic effects of UC-MSCs on an MIA-induced rat OA model, with the aim of determining the mechanisms of action involved. The rats were separated into 2 experimental group: the first group received single doses of 2.5 × 105 undifferentiated UC-MSCs 1 day after MIA, and the second group received 3 intra-articular injections of 2.5 × 105 UC-MSCs on 1, 7, and 14 days after MIA. 66 Joints from the rats were harvested and analyzed 4 weeks after MIA. While both single and triple doses of UC-MSCs were able to slow the progression of OA, their results showed that repeated UC-MSC injections were able to significantly reduce cartilage erosion, as well as decrease OA Mankin scores. 66 Repeated UC-MSC injections also increased the number of cartilage superficial layer cells (SFCs), which are essential to maintaining cartilage homeostasis, that were present on the surface of the articular cartilage. In addition, UC-MSCs switched SFCs from a catabolic to anabolic phenotype, protected them from apoptosis, and inhibited inflammatory cell infiltration. 66 While these findings emphasize the importance of repeated UC-MSC injections for the reduction of OA progression, they are impactful to the field by revealing a potential mechanism of action in which UC-MSCs protect and restore cartilage.
Amniotic fluid MSCs
Recently, investigators have become interested in evaluating the potential efficacy of MSC-secreted exosomes for OA. Exosomes are soluble signaling molecules that have been found to be the main secretory product of MSCs and function to carry various biomolecules, proteins, lipids, and nucleic acids (mRNA, microRNA [miRNA], and DNA) across cell membranes influencing cell signaling and regulating specific biological functions.67,68 Exosomal miRNA has also been shown to be involved in gene regulation, including those that encode type II collagen and play a key role in cartilage development and homeostasis. 68 Zavatti et al. 69 were able to demonstrate the efficacy of the growth factors and immunomodulating molecules found within amniotic fluid stem cell (AFSC) exosomes to promote cartilage repair and mitigate tissue destruction. Three weeks after an intra-articular injection of exosomes into an MIA-induced rat model of OA, the treatment group demonstrated an almost complete reconstruction of hyaline-like cartilage with no unwarranted inflammatory effects. 69 This study illustrates the ability of AFSC exosomes to aid in the repair of cartilage damage. Zavatti et al. 69 attributed these effects specifically to the transforming growth factor β (TGFβ) and nucleic acids in the exosomes to promote macrophages into the anti-inflammatory M2 state. These results also support previous findings that the healing potential of MSCs lies in the secretome produced by these cells and not necessarily their ability to differentiate and form new tissue.70,71
Perinatal MSCs’ Clinical Data
Umbilical cord–derived MSCs
In 2018, a human clinical trial was performed to determine the safety and efficacy of UC-MSC treatments over the course of 12 months. Patients with symptomatic knee OA with KL grades II-III were randomly divided into 3 groups: a control group consisting of 8 patients with a mean age of 54.8 ± 4.5 years that received 2 HA injections at baseline and 6 months, an “MSC-1” group consisting of 9 patients with a mean age of 56.1 ± 6.8 years that received a single dose of UC-MSCs (20 × 106 cells) followed by a placebo injection at 6 months, and an “MSC-2” group consisting of 9 patients with a mean age of 56.7 ± 4.1 years that received a dose of UC-MSCs (20 × 106 cells) at both baseline and 6 months. 72 This study revealed at 12 months the patients in the MSC-2 group had 86% pain reduction and 89% disability reduction versus 38% and 50% in the control HA group. The efficacy of the UC-MSC injections was evident as only MSC-treated patients showed significant improvements in pain and function from baseline, as opposed to the control patients. The MSC-1 group showed a duration of improvement for up to 9 months but by the end of the study demonstrated a similar level of symptoms as the HA control group, which lost effect for pain, function, and total WOMAC scores at 6 months, only to show improvement after receiving a second HA injection. 72 However, the MSC-2 group continued to show improvement in WOMAC and VAS outcomes along with significant clinical changes until the end of the study. As a result, this trial concluded that repeated UC-MSC doses were safe for the treatment of long-term pain in knee OA patients.
Another larger, open-label study was conducted from July 2015 to December 2018 in Indonesia. 73 This clinical study aimed to show the benefits of UC-MSCs over HA for treating knee OA in a larger subject group than previous clinical studies. There were 29 subjects enrolled in this study with KL grades varying from I-II (mild) to III-IIII (severe). The subjects were injected 3 times in total: in the first session, they received an intra-articular injection with 10 × 106 UC-MSCs; then in both the second and third week, they received injections with only 2 ml of HA. 73 The results of this study showed that VAS scores were significantly decreased in patients with severe knee OA at 6-month follow-up compared with their initial scores. Improvement continued in VAS scores until 12 months out in both the mild and severe OA groups; however, it was not statistically significant. WOMAC scores also improved and were significantly lower in both mild and severe OA from initial evaluation to 6-month follow-up. 73 As a result, this study concluded that hUC-MSCs have the potential to be a new regenerative treatment for OA with their maximum effect achieved after 6 months. 73 These results, along with data from other perinatal MSC studies mentioned in this article, can be found summarized in Tables 3 and 4 .
Summary of Preclinical Studies Evaluating the Efficacy of Perinatal MSCs to Mitigate OA.
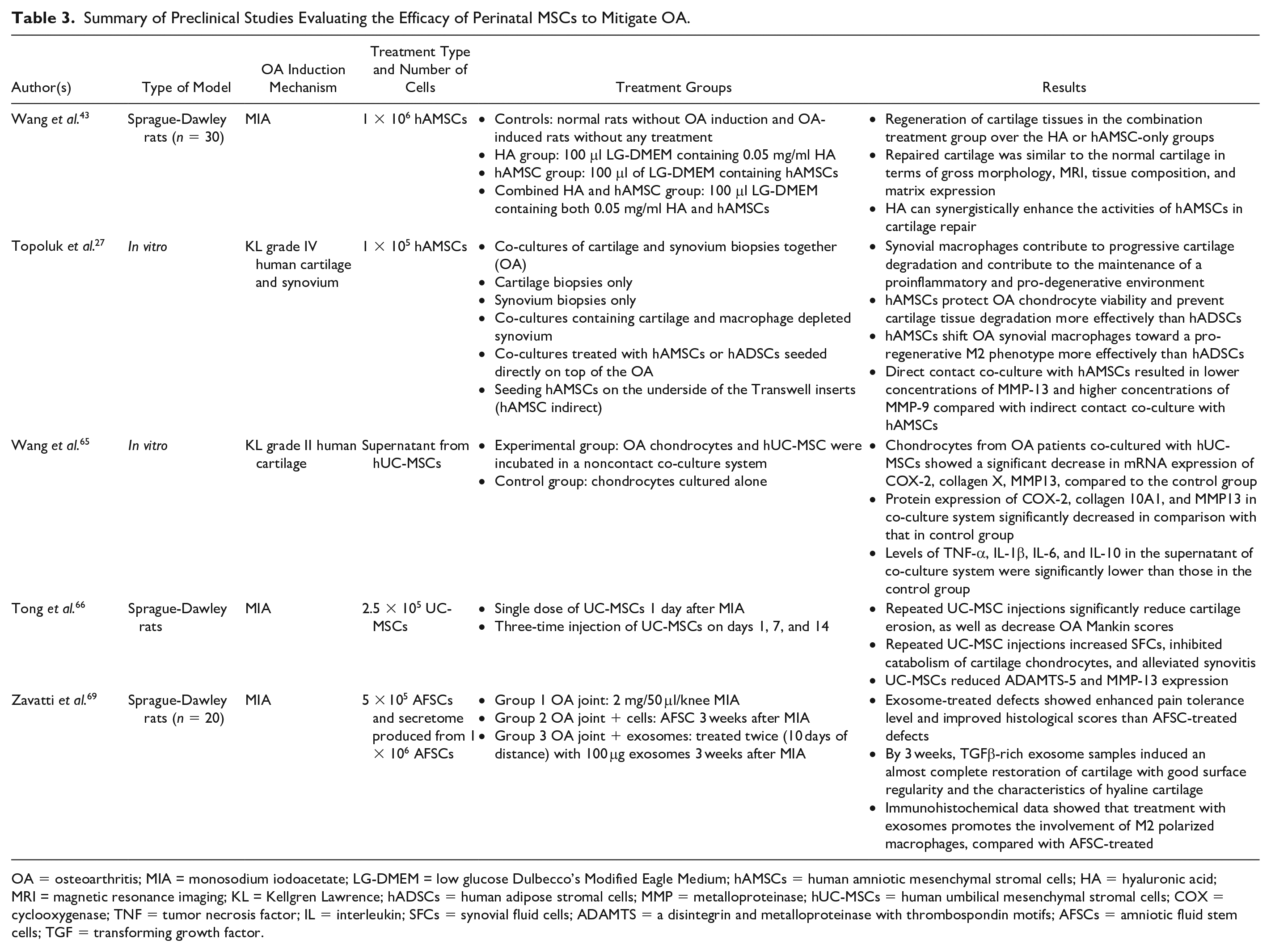
OA = osteoarthritis; MIA = monosodium iodoacetate; LG-DMEM = low glucose Dulbecco’s Modified Eagle Medium; hAMSCs = human amniotic mesenchymal stromal cells; HA = hyaluronic acid; MRI = magnetic resonance imaging; KL = Kellgren Lawrence; hADSCs = human adipose stromal cells; MMP = metalloproteinase; hUC-MSCs = human umbilical mesenchymal stromal cells; COX = cyclooxygenase; TNF = tumor necrosis factor; IL = interleukin; SFCs = synovial fluid cells; ADAMTS = a disintegrin and metalloproteinase with thrombospondin motifs; AFSCs = amniotic fluid stem cells; TGF = transforming growth factor.
Summary of Clinical Studies Evaluating the Efficacy of Perinatal MSCs to Mitigate OA.
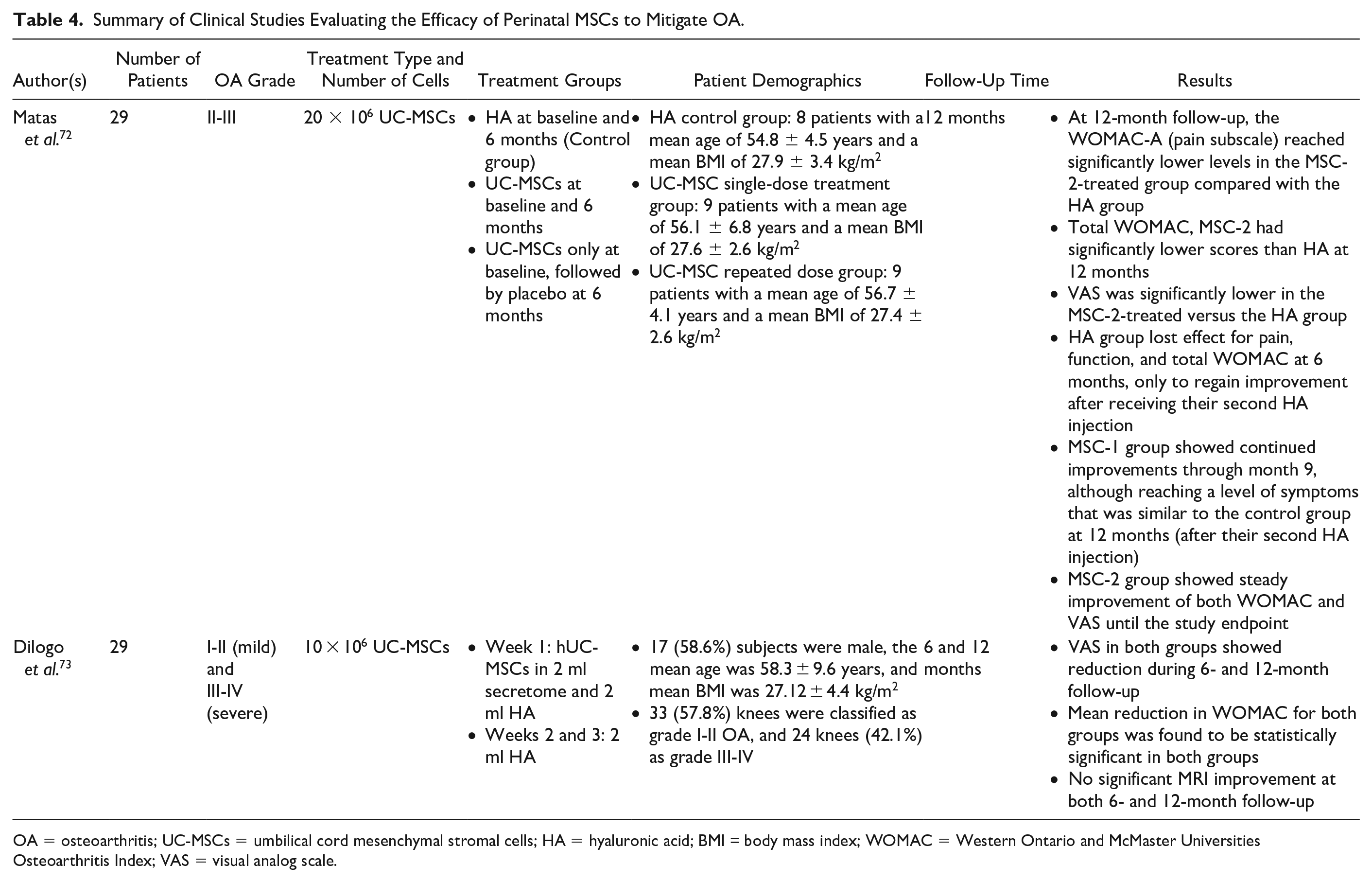
OA = osteoarthritis; UC-MSCs = umbilical cord mesenchymal stromal cells; HA = hyaluronic acid; BMI = body mass index; WOMAC = Western Ontario and McMaster Universities Osteoarthritis Index; VAS = visual analog scale.
Discussion
This review summarizes the evidence surrounding the use of perinatal tissue allografts and MSCs for their potential therapeutic management of OA; thus, the data summarized in this review support the “anti-OA” properties of perinatal tissues and MSCs. In general, available studies demonstrated the ability of these tissues and cells to reduce the levels of inflammatory cytokines and mitigate cartilage degradation and lesions. Perinatal tissues as well as MSCs derived from these tissues appear to be superior to both HA and steroid treatments in terms of modulating pain, improving physical joint function, and reducing patient-reported stiffness.
Of the studies mentioned in this article, very few identify a mechanism in which these treatments act to repair cartilage. In addition, there have been no studies published comparing perinatal tissue allografts and MSCs for the treatment of OA. While the process to manufacture perinatal tissue allografts may result in a loss of viable cells, the grafts retain the growth factors, anti-inflammatory cytokines, exosomes, and tissue inhibitor of metalloproteinases (TIMPs) produced by viable cells that were once present in the native tissue. This retention of bioactive factors is considered to be critical to the clinical efficacy and tissue regeneration potential of perinatal allografts 57 and is likely the same mechanism in which perinatal MSCs act to attenuate OA symptoms. Furthermore, unpublished work by our group has illustrated that perinatal tissue–derived MSC residence time within the joint following intra-articular administration is in the order of 1 to 2 weeks in preclinical models. This suggests that therapeutic benefit is likely due to release of soluble factors and not ECM production.
While preliminary data are plentiful, detailed clinical safety and efficacy studies need to be performed for perinatal tissue allografts and MSCs. The dose- and time-dependent effects of perinatal tissues and cells also need to be explored fully. An important area of investigation that needs to be further explored includes evaluating the safety and efficacy of repeat injections of perinatal tissue allografts or MSCs. As mentioned previously, Matas et al. illustrated that repeat injections of UC-MSCs did not result in more frequent or serious adverse events compared with a single dose of MSCs or HA alone, but did yield more sustained improvements in pain and function scores. 72 In contrast, Magatti et al. expressed concern for repeated transplantation of perinatal tissue–derived MSCs after noting that amniotic cells may have immunostimulatory properties after multiple administrations. 74 There has also been conflicting evidence as to the efficacy of single versus repeat injections of non-perinatal tissue–derived allogeneic MSCs and their potential to induce a humoral immune response, particularly following repeat injection.75,76
Magatti et al. also highlighted that adverse joint conditions might have an impact on AM cells after implantation. Amniotic cells might struggle to survive in vivo due to the lack of nutrients, lower levels of oxygen, and lower pH, 74 which are conditions often associated with osteoarthritic joints. Thus, defining the impact of the chemical environment of the osteoarthritic joint on perinatal MSC survival and effector function is also required. In addition, more studies aimed at identifying the intracellular pathways involved in the therapeutic response to perinatal tissue–derived therapies and their impact on the pathogenesis of OA need to be undertaken to better understand how to treat this disease in the future.
The quality, consistency, and potency of any injectable OA treatment, including those derived from perinatal tissues and cells, should also be standardized and reproducible. This has remained a significant challenge for autologous biological therapies including BMAC and adipose MSC injections. Large, multicenter studies evaluating the efficacy of perinatal tissue allografts and MSCs compared with other treatments including corticosteroids, HA, and other biologic treatments such as PRP, BMAC, and ADSCs need to be completed. Finally, recent studies suggest that physical characteristics of perinatal tissue allografts (i.e., particulate size) also need to be studied as such characteristics may impact efficacy. 77
Conclusion
Perinatal tissue–derived allografts and MSCs have demonstrated considerable promise as potential therapeutics for mitigating OA progression in preclinical and clinical studies. However, further research is warranted to fully characterize and define the therapeutic mechanism(s) of action of these biological therapies.
Footnotes
Acknowledgments and Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors would like to acknowledge the generous support from the John Witherspoon Gilpin M.D., ’82 Endowment as well as the SC BioCRAFT COBRE Center supported by the National Institute of General Medical Sciences (NIGMS) of the National Institutes of Health under award number P30 GM131959.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: ES, NW, and GO declare they have no conflict of interest. JM is the Chief Scientific Officer of Samaritan Biologics, LLC.
Ethical Approval
Ethical approval was not sought for the present study.