
Abstract
Objective
Balloon kyphoplasty with polymethylmethacrylate (PMMA) represents the standard procedure for the treatment of thoracic and lumbar type A compression fractures. However, an increased degeneration in adjacent intervertebral disks following PMMA kyphoplasty has been demonstrated in elderly patients. Calcium phosphate cement (CPC) appears to be superior to PMMA for the intravertebral stabilization in younger patients. It remains unkown whether CPC kyphoplasty causes degeneration of adjacent disks in adolescents.
Design
Seven adolescents with thoracolumbar spine fractures underwent kyphoplasty at a mean age of 14.5 years (range 10-18). At a mean follow-up of 3.7 years (range 1 to 4.8) postoperatively, 3.0 Tesla magnetic resonance imaging (MRI) of the spine was performed to assess intervertebral disk degeneration by quantitative T2 relaxation maps and subjective ratings using modified Pfirrmann scores. A total of 56 intervertebral disks was analyzed. Initial computed tomography (CT) examinations served as basis to assess the severity of adjacent endplate injuries in terms of articular step-offs.
Results
Initial imaging detected 18 thoracolumbar vertebral body fractures of which 9 were treated with CPC kyphoplasty. Quantitative follow-up MRI revealed signs of degeneration in 10 (17.9%) of the examined 56 intervertebral disks, 7 of them adjacent to a previously fractured vertebral body. Signs of disk degeneration were significantly higher in caudal endplates with articular step-offs larger than 5 mm compared to fractured vertebral bodies without endplate step-offs.
Conclusions
Quantitative MRI follow-ups did not suggest CPC-related intervertebral disk degradations following thoracolumbar kyphoplasty in adolescents, but indicated disk alterations correlating to adjacent endplate fracture severity.
Keywords
Introduction
Balloon kyphoplasty either performed as a stand-alone technique or in combination with internal stabilization is a widespread and accepted procedure for the treatment of thoracic and lumbar vertebral body fractures. 1 Polymethylmethacrylate (PMMA) bone cement is the current treatment standard for vertebral augmentation in elderly patients due to its ease of handling, good mechanical properties and favorable long-term clinical data. 2 However, conventional PMMA is non-degradable and does not promote bone ingrowth, possibly leading to aseptic loosening between bone and PMMA implants. 3 In contrast to PMMA, calcium phosphate cement (CPC) demonstrates osteoconductive properties with good osseointegration behavior combined with slow degradation and a high biocompatibility. 4 Thus, CPC appears to be superior to PMMA cement for kyphoplasties in younger patients and is therefore increasingly used as an alternative in spinal surgery in these patients.5-7
Excellent outcomes of adolescents with type A fractures (
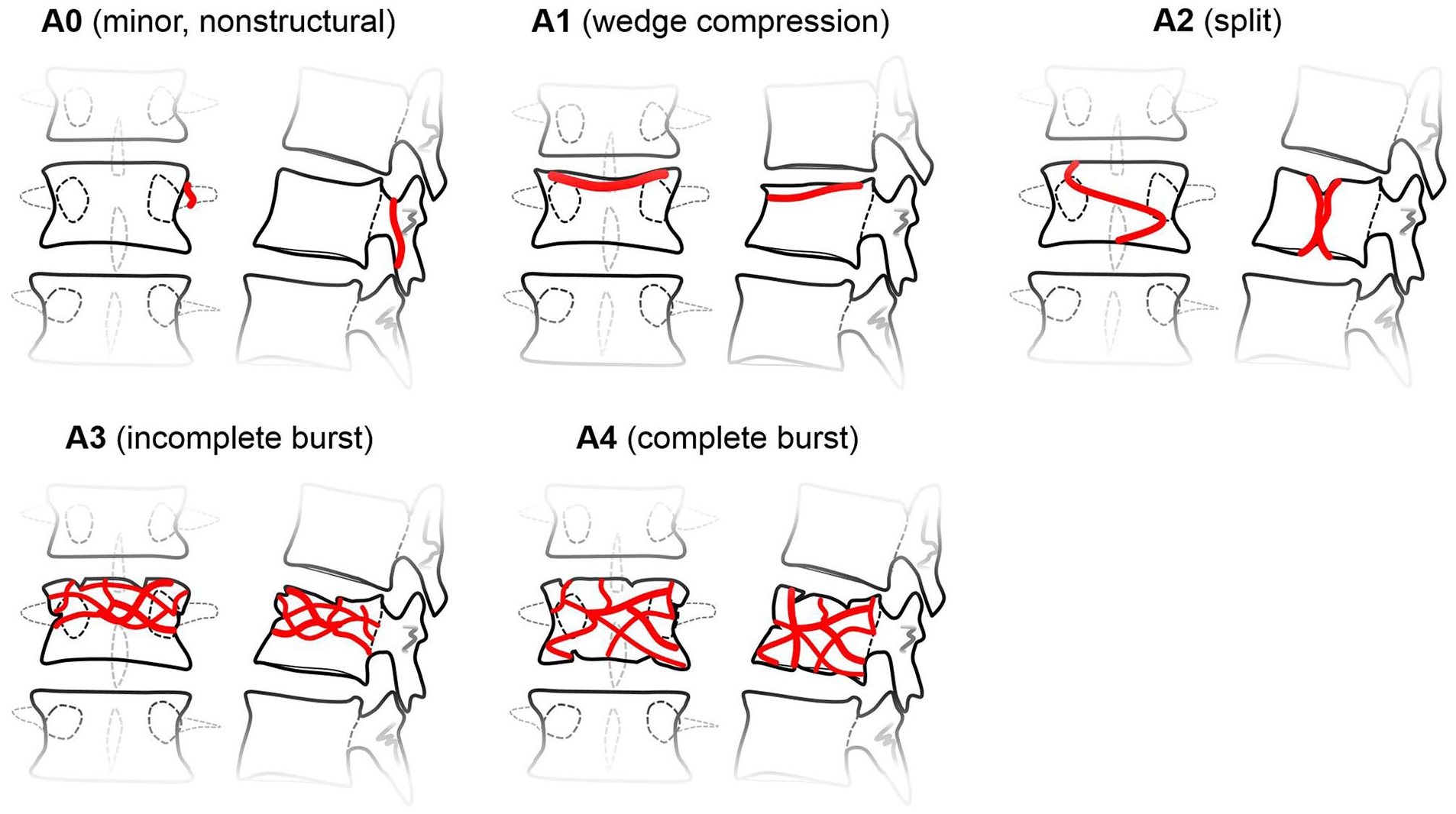
Schematic drawing of type A fractures of the spine. 10
With the expansion of indications for vertebral augmentation, procedure-related disk degeneration could reach clinical significance. In a recently published report, Pachowsky and coworkers have demonstrated increased degeneration in adjacent intervertebral disks following PMMA kyphoplasty in elderly patients. 11 However, the possibility of comparable procedure-related disk changes after vertebral balloon kyphoplasty using CPC in children and adolescents has not been examined yet.9,12 Therefore, the aim of our longitudinal long-term follow-up investigation was to assess the effect of balloon kyphoplasty with CPC on adjacent disks in a cohort of adolescent patients treated for thoracolumbar compression fractures.
Methods
Seven adolescents (2 females, 5 males) were treated with balloon kyphoplasty and CPC augmentation (Kyphos, Medtronic, Minneapolis, MN) for traumatic compression fractures of lumbar and thoracolumbar vertebrae between 2012 and 2016 and were included in our long-term follow-up observational study consisting of postoperative follow-up magnetic resonance imaging (MRI) scans of the spine. The mean age at the time of surgery was 14.5 years (10-18 years range). The mean weight was 59.5 kg (range 36.1-71 kg).
Pre-Operative Imaging
Preoperatively, spinal computed tomography (CT) scans were obtained in all patients. Grading of spinal fractures included the amount of vertebral body height reduction (measured as sagittal index).13,14 Since articular step-offs are known to precede cartilaginous damage in other joints, we decided to additionally grade the severity of proximal and distal endplate injuries radiologically. A pediatric radiologist with 6 years of experience in musculoskeletal imaging (S.T.) performed this procedure. Due to the lack of a proper rating system, we arbitrarily created 4 grades (
grade 0 = no visible injury,
grade 1 = injury without endplate step-offs,
grade 2 = injury with a step-offs smaller than 5 mm,
grade 3 = injury with a step-offs greater or equal than 5 mm.
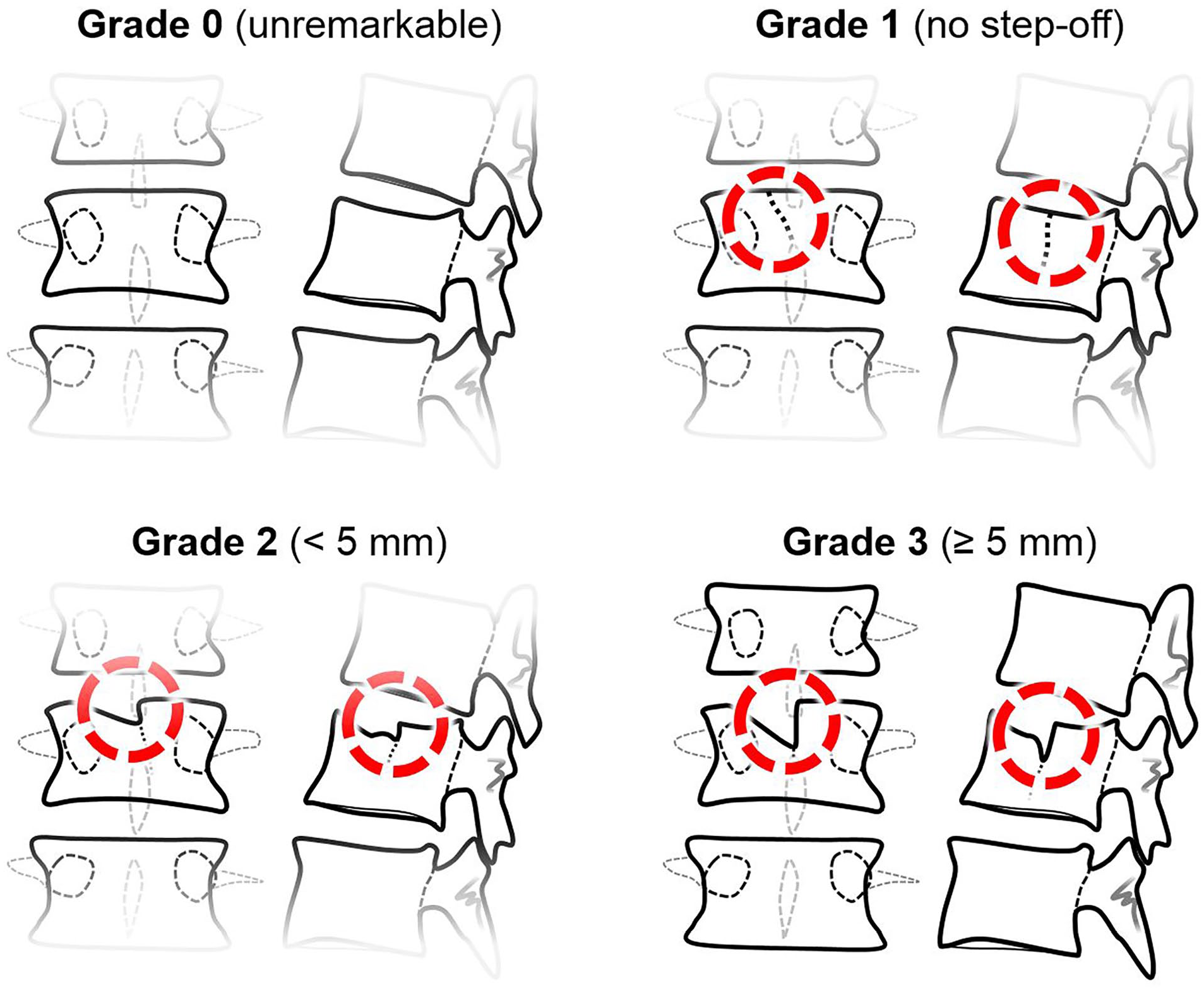
Schematic drawing of the 4 grades of articular step-offs.
Surgical Procedure
The surgical procedures were performed with the patients in prone position on a radiolucent carbon operating table. Firstly, balloon kyphoplasty (Kyphon, Medtronic ) and injection of CPC (Kyphos, Medtronic) were performed. To attribute the strong pediatric bone, kyphoplasty was realized very carefully raising the pressure stepwise (50 pounds per square inch [PSI] increments to a final pressure of 250-300 PSI) and pausing until the pressure declined to a stable value. Repeated intra-operative x-rays confirmed adequate reduction of the fractured vertebra. The void was then augmented with CPC under image intensifier control. No cement leakage was detected. Thereafter, dorsal percutaneous instrumentation of the adjacent segments using the Medtronic Longitude system (Medtronic) was performed. The fascia was carefully closed to avoid subcutaneous hematoma. Postoperatively, the patients had bed rest for 24 h according to the choice of the surgeons followed by mobilization with full weight bearing and without brace. Sports activities were prohibited for 3 months.
Radiological Follow-Up
The follow-up MRI images were acquired on a 3 Tesla (T) Prisma® scanner (Siemens Healthineers, Erlangen, Germany) with integrated spine coils. Patients were scanned in supine position. All slices were generated with an identical field of view of 260 mm, 16 slices, and 4 mm slice thickness to enable stacking. T2 maps were generated inline by MapIt (Siemens Healthineers, Erlangen, Germany). The length of the imaging protocol was 8 min and 34 s. Turbo spin echo (TSE) sequences as specifically listed in
Overview of the MRI Sequences Used.
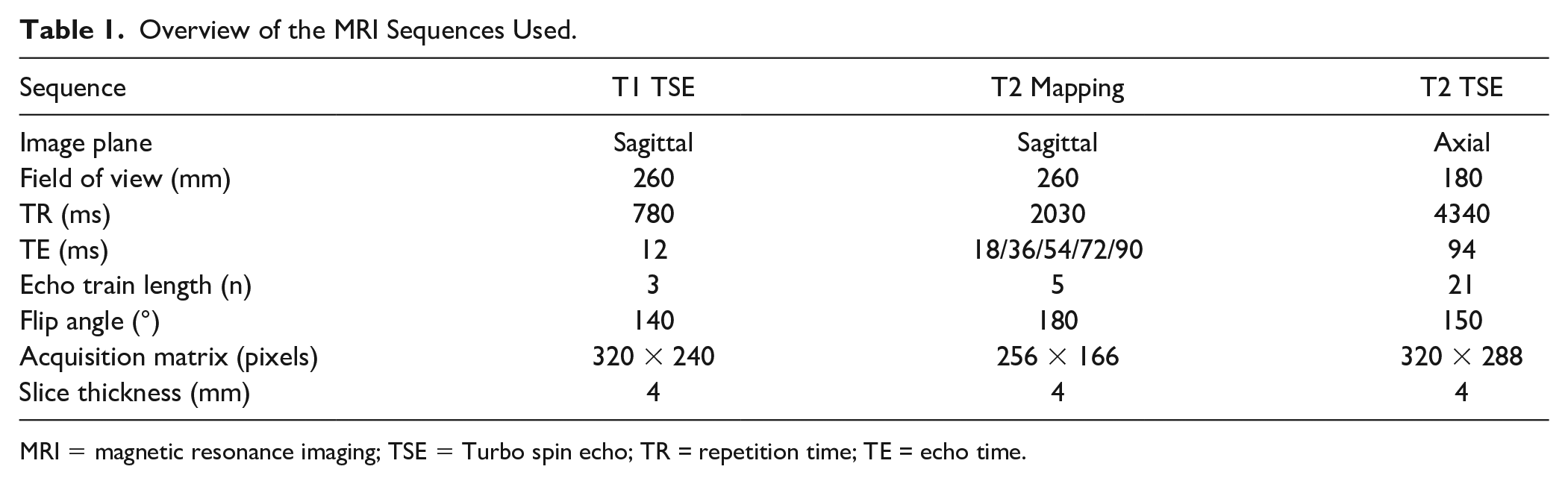
MRI = magnetic resonance imaging; TSE = Turbo spin echo; TR = repetition time; TE = echo time.
The MRI studies were analyzed both subjectively and objectively. Subjectively, intervertebral disk conditions were rated based on the 8-graded modified Pfirrmann score.
15
To assess T2 relaxation times (ms) as surrogate parameter of objective disk degeneration, intervertebral disks were manually segmented in all slices of the sagittal T1-weighted sequence by using polygonal regions of interest (ROIs). These ROIs were afterwards applied onto the corresponding sagittal T2 maps (
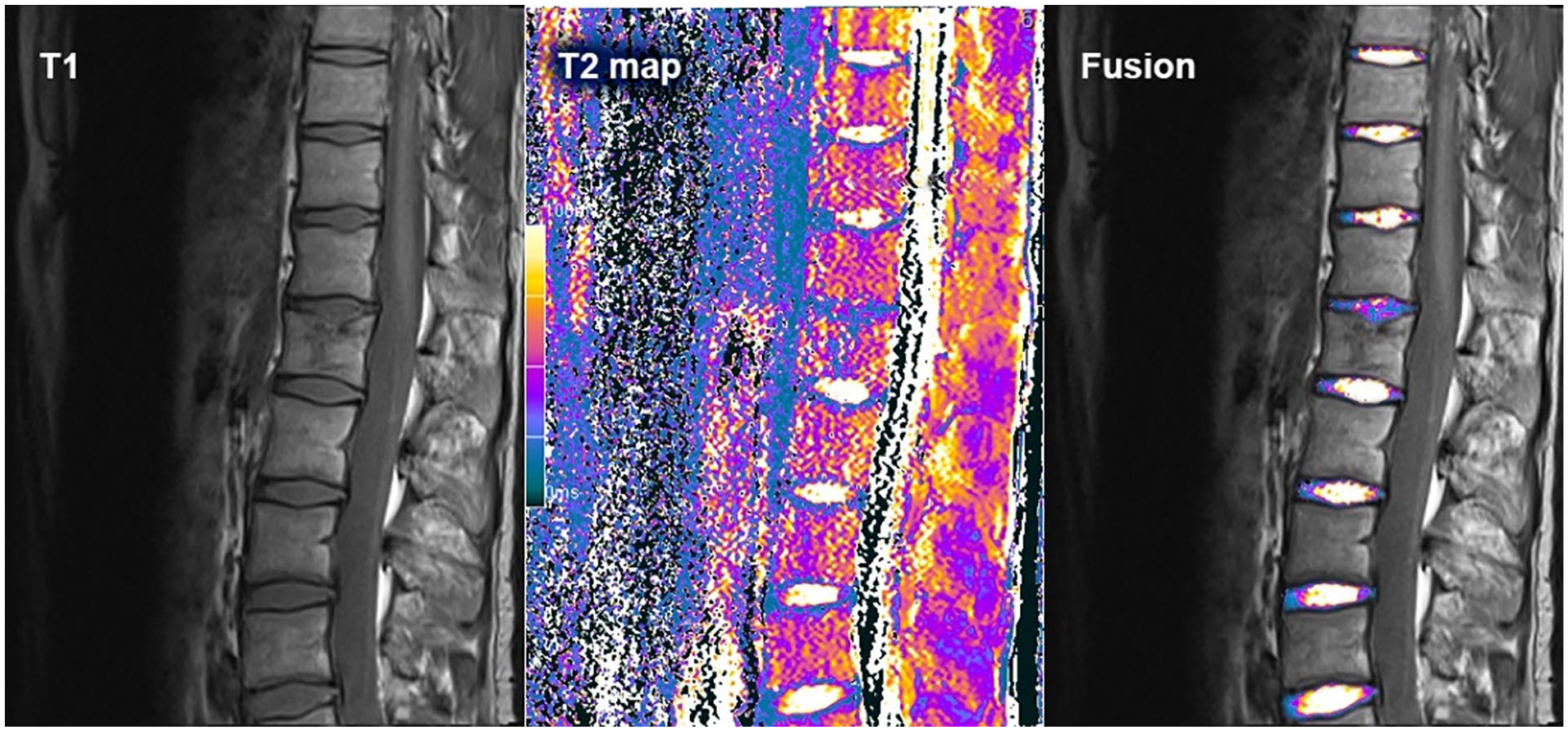
A single-segment intervertebral disk degeneration in a patient with an adjacent proximal endplate fracture. Sagittal T1 sequence on the left, T2 map in the middle, and the fused image on the right.
Statistical Analysis
Statistical tests were computed with SPSS v21 (SPSS Inc., Chicago, Illinois). Descriptive statistics and Pearson’s correlations were used to explore and describe the data. Due to the limited number of samples per sub-group and potentially lacking normal distributions nonparametric Mann–Whitney U tests was chosen for group comparisons. P-values lower than 0.05 were considered statistically significant.
The sagittal indices measured preoperatively, postoperatively and at follow-up were compared with the Friedman test. Post hoc analysis with Wilcoxon signed-rank tests was conducted with a Bonferroni correction applied, resulting in a significance level set at P < 0.017.
Ethical Statement
The Medical University of Graz’ local ethics committee (IRB00002556) approved this prospective study (No. 28-442 ex 15/16). All patients and/or their legal guardians gave written informed consent to participate in this study.
Results
At the time of injury all seven patients were healthy and without a history of back pain.
Basic Patient Characteristics, Information About the Level and Time Point of Kyphoplasty and Internal Stabilization, as Well as Sagittal Indices Pre-, Post-Operative and at Follow-Up.
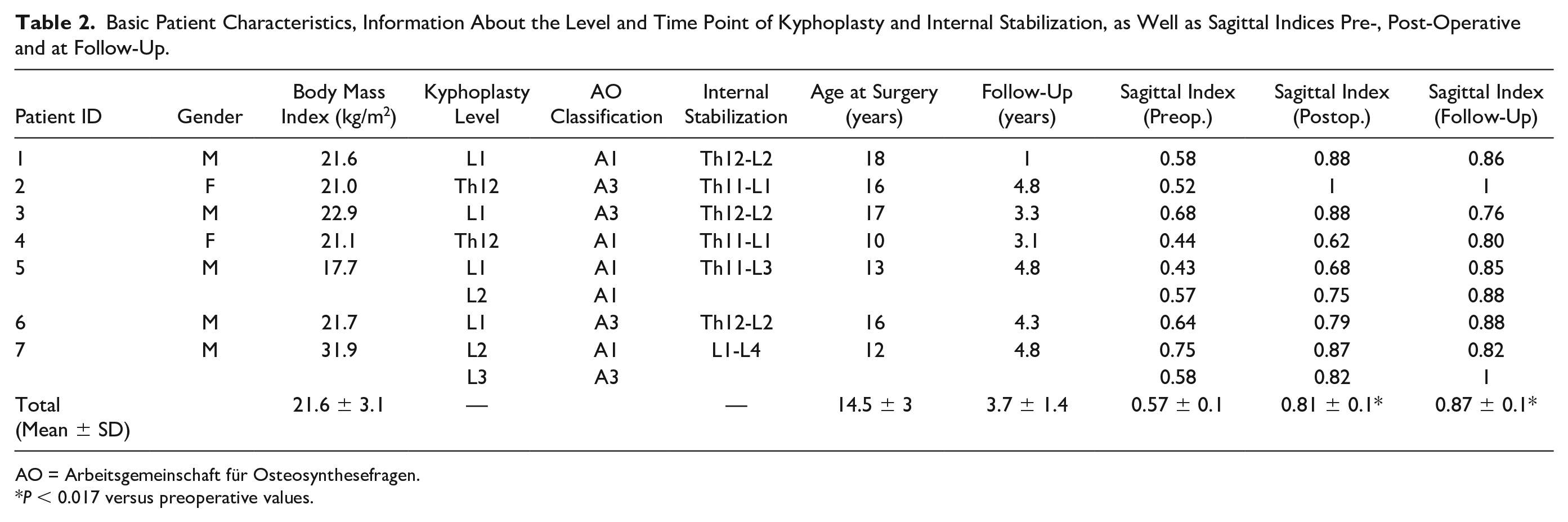
AO = Arbeitsgemeinschaft für Osteosynthesefragen.
P < 0.017 versus preoperative values.
The long-term follow-up MRI scans of the spine were performed at a mean of 3.7 years (range: 1.0-4.8 years) postoperatively. We acquired sagittal sequences with a constant field of view, cranio-caudally centered to the kyphoplasty locations (n = 9). Monovertebral kyphoplasties had been performed in 5 patients. In 2 patients 2 vertebral bodies had been treated with kyphoplasty. The resulting 16 intervertebral disks adjacent to a vertebral body with kyphoplasty, together with all other entirely visible disks (n = 40) were included into the analyses, totaling into 56 disks ranging from T8-9 and L5-S1. A median of 8 (range: 7-9) disks were imaged per patient.
MRI revealed that 10 (17.9%) of the examined 56 intervertebral disks demonstrated varying signs of degeneration. Three of these altered disks were noted at the lumbosacral junction, lacking a perceptible relationship to the spinal fractures. However, the 7 remaining degenerated disks were adjacent to a previously fractured vertebral body (1 above, 3 below, and 3 on both neighboring levels) and were used for further analyses.
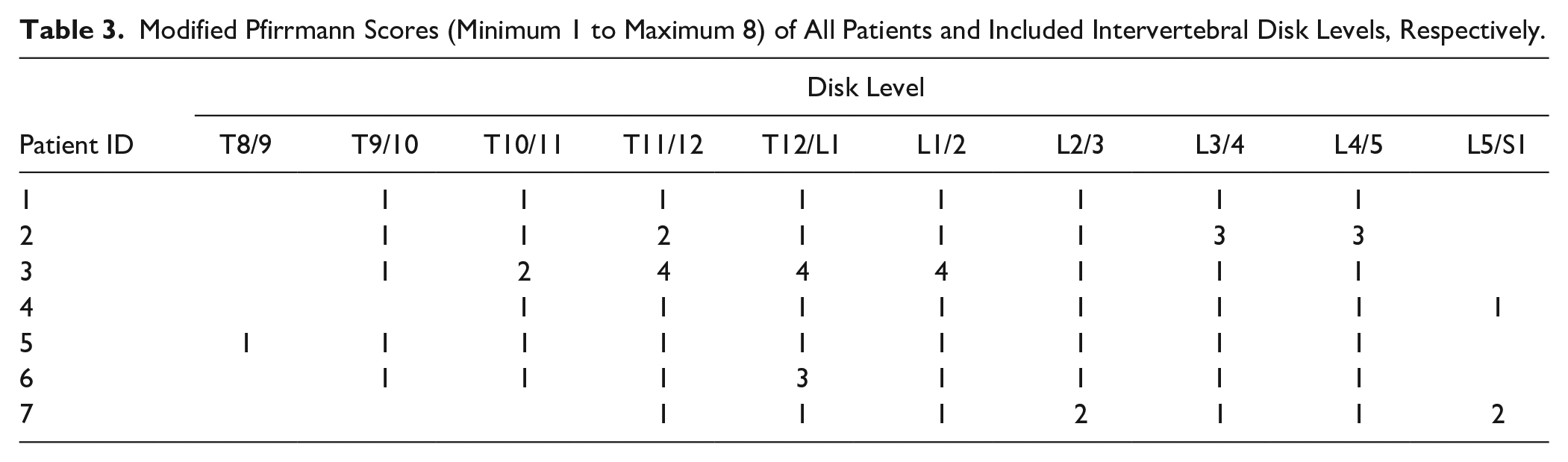
Semi-objective (T2 times) and subjective (modified Pfirrmann scores,
Modified Pfirrmann Scores (Minimum 1 to Maximum 8) of All Patients and Included Intervertebral Disk Levels, Respectively.
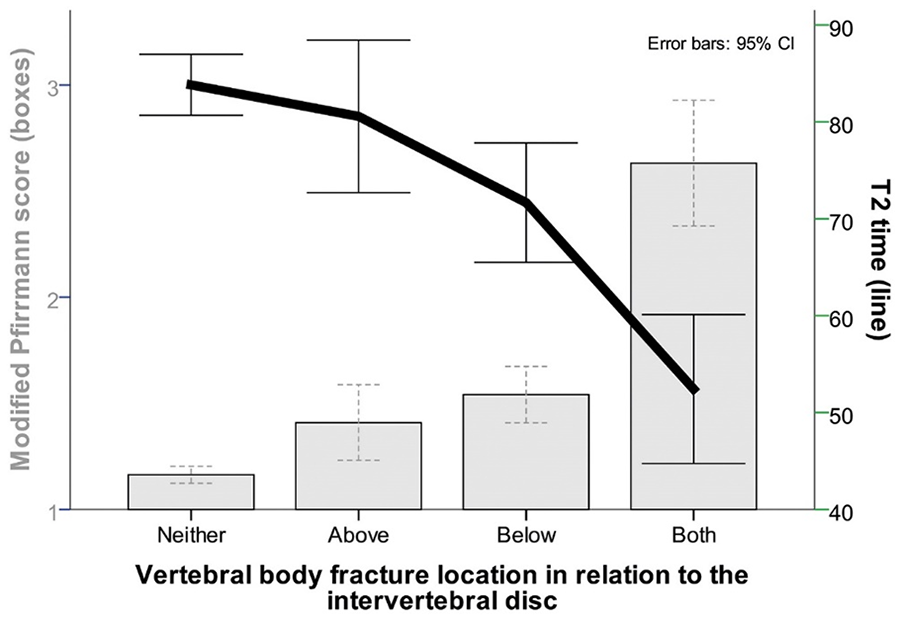
A combined chart shows vertebral body fracture locations related to the respective intervertebral disks for mean modified Pfirrmann score (boxes) and mean T2 time (line) in ms (milliseconds). 32 disks had no adjacent vertebral body fracture; 6 only above, 7 only below, and 11 above and below. 95% CIs with error bars are displayed. CI = confidence interval.
There was a significant negative Pearson correlation between T2 time and the radiological severity score of adjacent endplate injuries caudal to an intervertebral disk (R = -0.487, P < 0.001), but not for neighboring cranial endplate injuries (R =- 0.106, P = 0.436). Both T2 times and the modified Pfirrmann scores were significantly different between disks below an endplate with and without fracture-related step-offs (U test, P = 0.003 and P = 0.015, respectively). Semi-objective and subjective disk degeneration parameters were significantly worse in caudal endplates with step-offs larger than 5 mm, when compared to injured vertebral bodies without endplate step-offs (U test both P < 0.001). We did not see significant T2 time and modified Pfirrmann score differences between caudal endplates with step-offs smaller or larger than 5 mm (U test P = 0.149, and P = 0.178) (
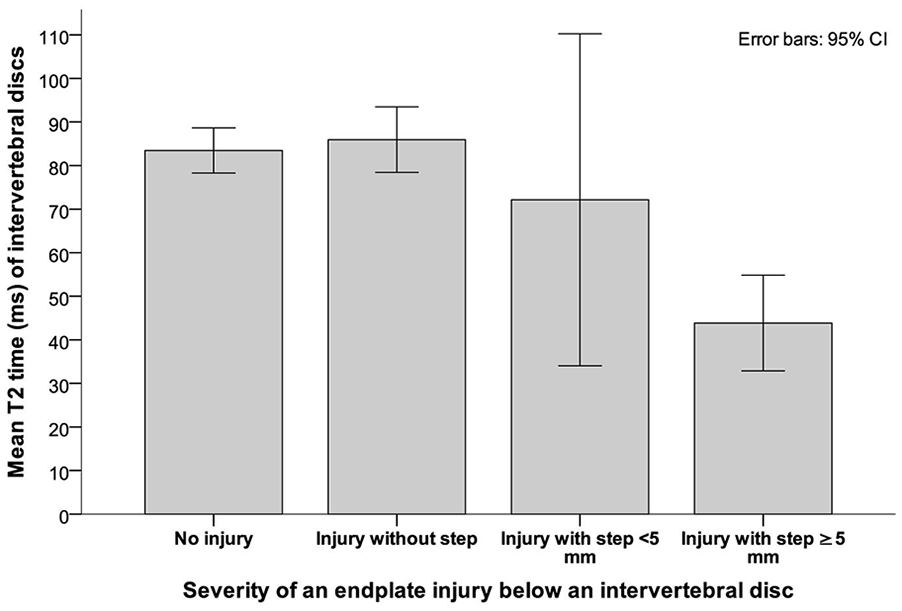
A bar chart displaying mean T2 times of intervertebral disks compared to the severity of an adjacent endplate injury below. 39 caudal endplates showed no signs of injury, 9 had no step-off, 4 had a step-off smaller, and 4 greater than 5 mm. 95% CIs with error bars are shown. CI = confidence interval.
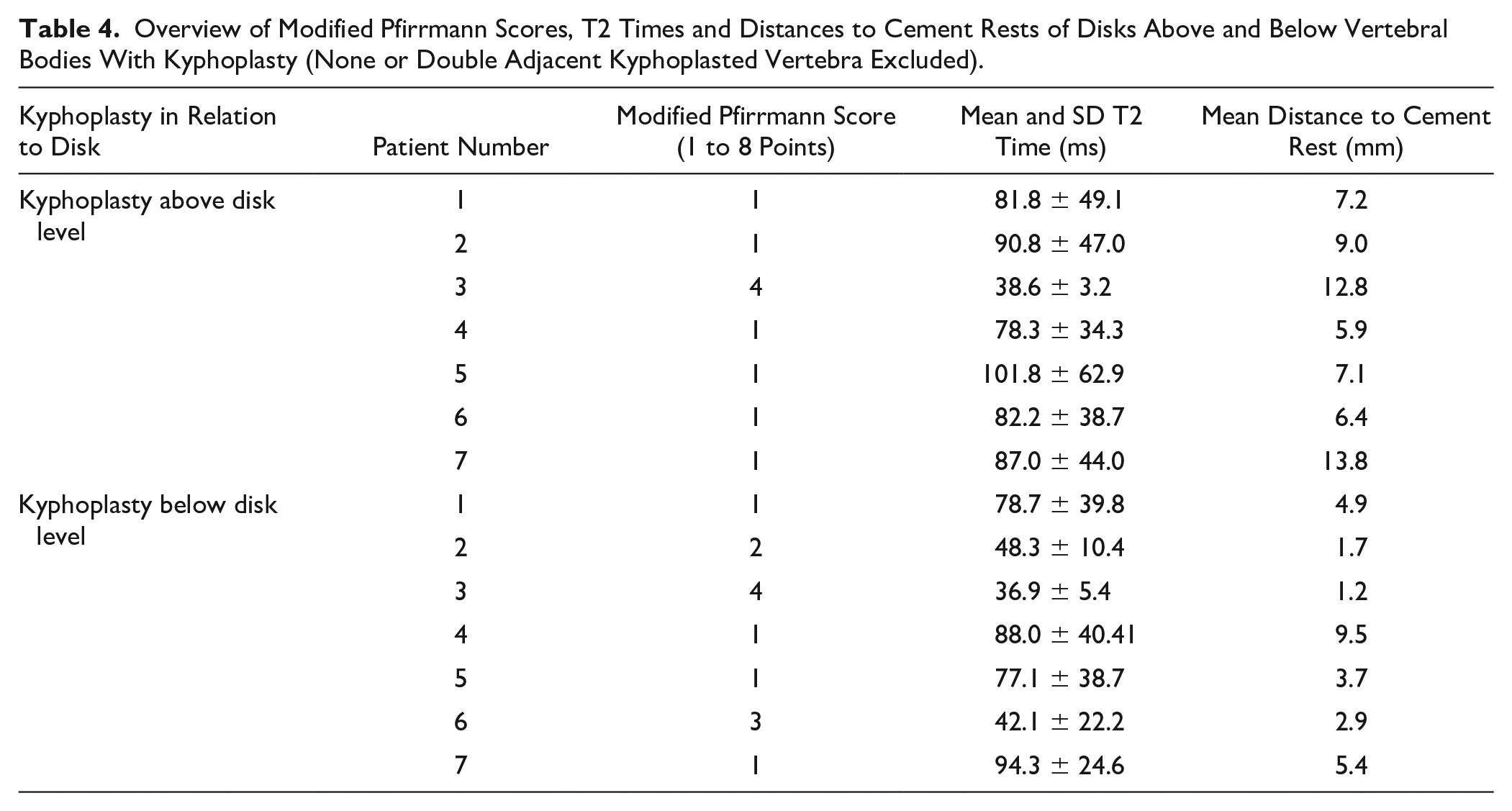
All kyphoplasted vertebral bodies demonstrated cement rests on follow-up MRI examinations, ranging from 8.9% to 53.2% with a median of 21.2% of the intra-operatively injected amounts. There was a significant correlation of mean distance to a cement rest with T2 times (R = 0.766, P < 0.001), inducing further analyses to differentiate between kyphoplasty-related and trauma-induced intervertebral disk damage by specifically excluding the disks (n = 2) between the 2 double kyphoplasties (
Overview of Modified Pfirrmann Scores, T2 Times and Distances to Cement Rests of Disks Above and Below Vertebral Bodies With Kyphoplasty (None or Double Adjacent Kyphoplasted Vertebra Excluded).
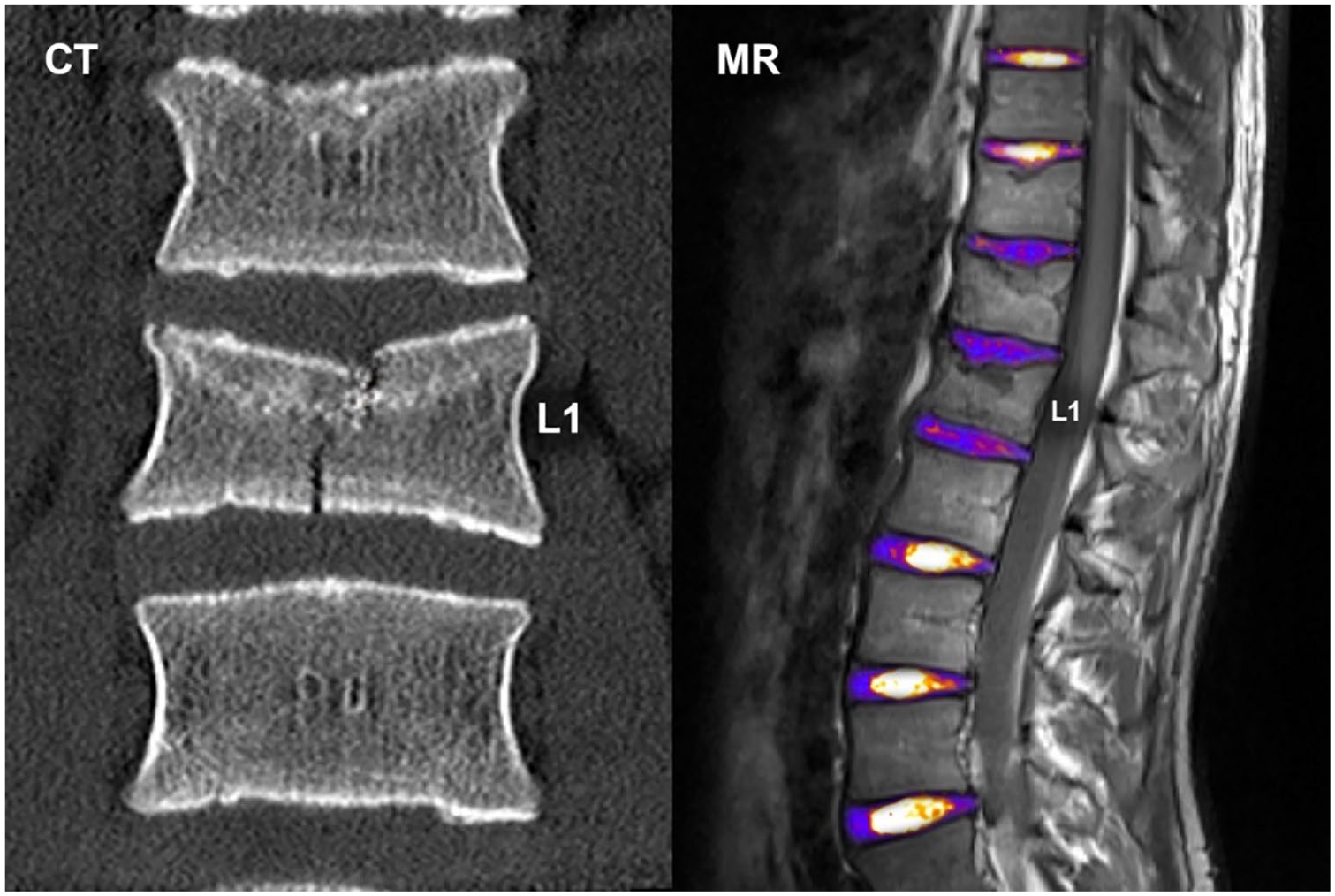
One patient (ID 3) presented with a disk degeneration below the level of kyphoplasty. This patient also sustained the only single vertebral fracture clearly affecting a caudal endplate. The initial CT on the left depicts the endplate fracture at L1 level reaching both endplates. MR (fusion of T1 and color-coded T2 mapping) on the right with obvious disk degeneration below the fractured and kyphoplasted L1 vertebra. CT = computed tomography; MR = magnetic resonance.
Discussion
In this study, we performed MRI follow-ups of adolescent patients after post-traumatic thoracolumbar kyphoplasty with CPC augmentation. Intervertebral disk damages were noted in 4 out of seven patients. However, our results favor primarily trauma-induced causes over CPC-related disk degradation.
In case of spinal compression fractures, there is a trend toward combined treatment consisting of balloon kyphoplasty with cement augmentation and percutaneous dorsal instrumentation.17,18 Advantages are the minimally invasive approach and good mechanical support,19,20 making kyphoplasties suitable for a large group of patients. However, knowledge about sequelae is still limited.21-23
Drawbacks of the traditionally used PMMA are linked to the potential toxicity of methyl methacrylate, the lack of bioactivity and the exothermic setting after application, which can induce local inflammatory reactions with concomitant osteonecrosis. 2 Moreover, the exothermic setting after implantation with PMMA may also potentially damage the spinal cord and nerves if bone cement leaks into the spinal canal. 24 A recently published study using quantitative MRI reported disk degeneration adjacent to vertebral bodies with PMMA kyphoplasty in patients with osteoporotic fractures. 11 In contrast to PMMA, CPC is osteoconductive with proven osseointegration behavior and good biocompatible.5-7 Thus, CPC is increasingly used in younger patients with vertebral compression fractures. 2 However, the long-term effects of cementing on the status of adjacent disks have not been studied. Intradiscal leakage, high temperature generated during application and the interference with nutrient transport could all possibly influence disk degeneration. 25 Moreover, possible adverse effects to adjacent disks following balloon kyphoplasty with cement augmentation still cannot be ruled out. 9 Qian and coworkers reported 97 patients with accelerated disk degeneration in a short-term follow-up of 2 years after kyphoplasty. 12 The 52.6% of the intervertebral disks next to the PMMA augmented vertebrae showed degenerative changes. However, no information is given regarding existing disk degeneration prior to cement augmentation and therefore no conclusion can be drawn if the procedure accelerated the process of disk degeneration. Additionally, their patient collective was older than in the current study (mean age 65.3 years versus 15.2 years).
König et al. presented a 94.3 months follow-up of 7 patients after cement augmentation with PMMA due to thoracic and lumbar compression fractures. Compared to the pre-existing degenerative changes in a short-term follow-up MRI after 15.2 months they found a progression of Pfirrmann score by 1 grade only in 1 out of 20 adjacent disks. The authors concluded that PMMA cement augmentation does not seem to accelerate disk degeneration dramatically, indicating safe usage. 9 However, one drawback of this study was the relatively high age of the patients (mean 67.1 years, range: 58-77 years) with pre-existing degenerative changes in thoracolumbar disks. Disk nutrition via endplates is already affected at this age and therefore the actual effect of cement within the body cannot be estimated. 25
In contrast to the previous study published by Pachowsky et al., 11 we did not find signs of kyphoplasty-related disk damages. The authors have examined intravertebral disks of 14 elderly patients following kyphoplasty using PMMA with quantitative T2 mapping and could demonstrate increased degeneration in adjacent intervertebral disks following kyphoplasty. 11 However, the mentioned study assessed PMMA instead of CPC and did not estimate or consider severity of traumatic endplate injuries. Therefore, they might come to a divergent conclusion compared to our data. In case of kyphoplasty-related damaging effects, intervertebral disks adjacent to a kyphoplasty would be expected to be more regularly affected. However, this was not the case in our patients. Moreover, one would think that both adjacent disks (below and above the kyphoplasty) would be degenerated. We believe that the significant correlation between cement rest to proximal endplate distances with disk degeneration is caused by the traumatic endplate impaction, resulting in a loss of vertebral height and a lower distance of the cement to the endplate. This theory is supported by a significantly higher grade of endplate injuries adjacent to a degenerated disk. It also should not remain uncommented that all patients in the present study were young and did not exhibit any pre-traumatical spinal complaints. We hypothesize that the rate of degenerative disk changes is lower than in the above mentioned studies performed in adult and elderly patients. Overall, we did not find definite signs that would favor CPC kyphoplasty over trauma or degeneration as cause for the observed intervertebral disk tears.
We decided to perform MRI follow-ups with quantitative techniques like T2-mapping, which might be able to detect disk degeneration at an earlier stage than conventional MRI.26-29 The results might also be affected by the individual MRI scanner and software used. However, as all of our patients were scanned on the same machine, the images and results should be safe for comparisons among themselves. It needs to be mentioned that artifacts (mainly caused by patient motion and pulsation) might distort the mean T2 times in the mapping procedure. This effect is commonly seen in clinical routine, could be of great influence on the results, but is rarely discussed in the respective literature. 30 In our assessments, we used median T2 times of each included image slice and calculated the mean across all individual slices. The robustness of this procedure is supported by a significant negative correlation with the modified Pfirrmann scores.
The main limitation of this study is the small sample size, which implicates the necessity for further research. Additionally, a preoperative MRI to correlate our follow-up MRI findings was not available in our patients with type A compression fractures lacking signs of spinal cord injuries. Therefore, we cannot exclude with certainity that the degenerative disk changes already existed before the trauma. However, the fact that our patients were much younger than the patients of other studies (mean 14.5 years versus, for instance, Pachowsky et al. 11 mean age 64.5 years and Qian et al. 12 65.3 years) and did not complain about preoperative back pain decrease the probability of preexisting disk degenerations and add an important novel aspect to consider within this research topic. Moreover, this investigation explicitly focused on disk degeneration after balloon kyphoplasty and augmentation with CPC. Therefore, no attempt was made to correlate clinical outcome, grade of height restoration or kyphosis angle with MRI findings. Another drawback is the moderate follow-up period of roughly 4 years on average.
In conclusion, follow-up MRI studies did not suggest CPC-related intervertebral disk degradations after post-traumatic thoracolumbar kyphoplasty in adolescents, but indicated that traumatic disk injuries might be linked to adjacent endplate fracture severity in terms of endplate step-offs.
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
]The Medical University of Graz’ local ethics committee (IRB00002556) approved this prospective study (No. 28-442 ex 15/16). All patients and/or their legal guardians gave written informed consent to participate in this study.