
Abstract
Objective
The purpose of the current study is to evaluate the clinical and radiographic outcomes at early to midterm follow-up between fresh precut cores versus hemi-condylar osteochondral allograft (OCAs) in the treatment of symptomatic osteochondral lesions.
Design
A retrospective review of patients who underwent an OCA was performed. Patient matching between those with OCA harvested from an allograft condyle/patella or a fresh precut allograft core was performed to generate 2 comparable groups. The cartilage at the graft site was assessed with use of a modified Magnetic Resonance Observation of Cartilage Repair Tissue (MOCART) scoring system and patient-reported outcomes were collected.
Results
Overall, 52 total patients who underwent OCA with either fresh precut OCA cores (n = 26) and hemi-condylar OCA (n = 26) were pair matched at a mean follow-up of 34.0 months (range 12 months to 99 months). The mean ages were 31.5 ± 10.7 for fresh precut cores and 30.9 ± 9.8 for hemi-condylar (P = 0.673). Males accounted for 36.4% of the overall cohort, and the mean lesion size for fresh precut OCA core was 19.6 mm2 compared to 21.2 mm2 for whole condyle (P = 0.178). There was no significant difference in patient-reported outcomes including Visual Analogue Scale, Knee Injury and Osteoarthritis Outcome Score for Joint Replacement, and Tegner (P > 0.5 for each), or in MOCART score (69.2 vs. 68.3, P = 0.93).
Conclusions
This study found that there was no difference in patient-reported clinical outcomes or MOCART scores following OCA implantation using fresh precut OCA cores or size matched condylar grafts at early to midterm follow-up.
Introduction
Chondral and osteochondral lesions of the knee are widely prevalent, with as many as two thirds of knee arthroscopies demonstrating focal lesions regardless of the initial indication for surgery.1-4 Injuries to the articular cartilage are often painful and may accelerate the development of osteoarthritis.5,6 A variety of factors including the size, location, and status of the underlying subchondral bone plate can assist surgeons in selecting the most appropriate management strategy, though there is no gold standard treatment for symptomatic chondral defects of the knee at the present time. Transplantation of osteochondral allografts (OCAs) has been shown to be beneficial for the treatment of chondral and osteochondral lesions, with various studies demonstrating a consistently favorable impact on functional outcomes, reliable survivorship, and high rates of return-to-play in athletes.7-11
OCA transplantation has historically been harvested from a size matched condyle intraoperatively to allow for orthotopic matching with the osteochondral defect site. However, in recent years tissue banks have been providing fresh precut allograft cores to increase graft availability and reduce matching times. Precut allograft cores have been utilized for lesions <2 cm as the potential for mismatch is reduced when treating smaller lesions. Additionally, it is unclear how much the orthotopic matching affects postoperative outcomes or if storage preparation between the 2 graft types affects viability. Therefore, early radiologic differences between the grafts may be a harbinger for potential failures.
The purpose of this study is to evaluate the clinical and radiologic outcomes between fresh precut OCA cores versus size matched hemi-condylar OCA in the treatment of symptomatic chondral and osteochondral lesions of the knee. We hypothesized that there would be no clinical or radiologic difference between fresh precut OCA cores and size matched condylar OCA as indicated by Magnetic Resonance Observation of Cartilage Repair Tissue (MOCART) scoring or patient-reported outcomes (PROs).
Methods
This study was approved by the local institutional review board (i20-01168). A retrospective review was performed from January 2011 to January 2019 for patients who underwent an OCA to treat a symptomatic chondral or osteochondral lesion of the knee. Inclusion criteria included patients with a preoperative diagnosis of a chondral defect of the knee who were treated with OCA and had an MRI (magnetic resonance imaging) at least 6 months postoperatively. Patients with a prior diagnosis of knee osteoarthritis or inflammatory joint disease were excluded, and patients were not excluded on the basis of alignment or associated meniscal or ligamentous pathology. Subsequently patient matching between those with OCA harvested from a size matched condyle/patella or a fresh precut allograft core was performed by the research team. Demographic factors such as age, gender, BMI (body mass index), lesion location, lesion size, concomitant surgery, and length of follow-up were all taken into consideration in order to generate 2 groups that were as comparable as possible.
Surgical Technique and Rehabilitation Protocol
OCA was either harvested from a size matched condyle/patella or a fresh OCA core (JRF Ortho). The surgical technique was performed as previously described. 12 Following surgery, patients were kept non-weight-bearing and in a hinged knee brace for the first 6 weeks. Continuous passive motion was used for all patients during this time. Patients were then gradually progressed to full weight-bearing between weeks 6 and 12, with range-of-motion goals of 90° by week 6, 130° of flexion by week 8, and full/painless knee range-of-motion by 3 months postoperatively. Activities such as jogging were permitted at 4 to 6 months while return to athletic activity was permitted at 6 to 9 months postoperatively.
Clinical Outcomes
Visual Analogue Scale (VAS) scores for pain were taken preoperatively, as well as at final follow-up, in which patients were asked to designate a VAS score at rest as well as during activity. Knee Injury and Osteoarthritis Outcome Score for Joint Replacement(KOOS JR) is a 7-question version of the validated KOOS survey assessing for patient stiffness (1 item), pain (4 items), and functions of daily living (2 items). 13 Scores range from 0 to 100 with a score of 0 indicating total knee disability and 100 indicating perfect knee health. Tegner Activity Scale provides a standardized method to determine the level of activity prior to injury and level of activity postinjury that can be documented on a numerical scale. 14 Patients reported their level of activity using the Tegner Activity Scale both preoperatively and at final follow-up.
Radiological Evaluation
Postoperative MRI exams were performed on either 1.5-T (Magnetom Aera or Avanto, Siemens) or 3-T (Magnetom Skyra, Verio, or Biograph, Siemens) magnets utilizing a standard diagnostic knee imaging protocol. There was some variability between exam protocols, but all protocols included the following pulse sequences: sagittal T2 with fat suppression, sagittal proton density, coronal proton density with fat suppression, coronal proton density, and axial T2 images with fat suppression. Each MRI was independently reviewed by a fellowship trained, board-certified musculoskeletal radiologist with 5 years of experience (EA) who was blinded to the surgical procedure. The cartilage at the graft site was assessed with use of a modified MOCART scoring system.
Statistical Analysis
All statistical analysis was performed utilizing GraphPad Prism 8.3. For all continuous and categorical variables, descriptive statistics were calculated. Continuous variables were reported as weighted mean and estimated standard deviation, whereas categorical variables were reported as frequencies with percentages. Categorical variables were analyzed using Fisher’s exact or χ2 test. The independent or paired t test for normally distributed variables, or the nonparametric Mann-Whitney U test or Wilcoxon signed-rank test was performed to compare continuous variables. A value of P < 0.05 was considered to be statistically significant.
Results
Patient Demographics
Overall, it was possible to match 52 total patients who underwent OCA with either fresh precut OCA cores (n = 26) or size matched condylar/patella OCA (n = 26) at our institution who met our inclusion and exclusion criteria. Patient inclusion/exclusion flow chart can be found in Fig. 1 . The mean age in the whole condyle group and fresh precut groups, respectively, were 30.9 ± 9.8 and 31.5 ± 10.7 (P = 0.673). In both groups, 61.5% of the patients were male. The mean lesion size was 27.1 ± 5.1 compared to 27.3 ± 6.3 mm2 (P = 0.918). While the lateral femoral condyle (LFC) was the most common location of the lesion in both groups, there was no difference in lesion location overall. There were no significant differences in any patient demographic variables, including concomitant procedures. Patient demographics are further illustrated in Table 1 .
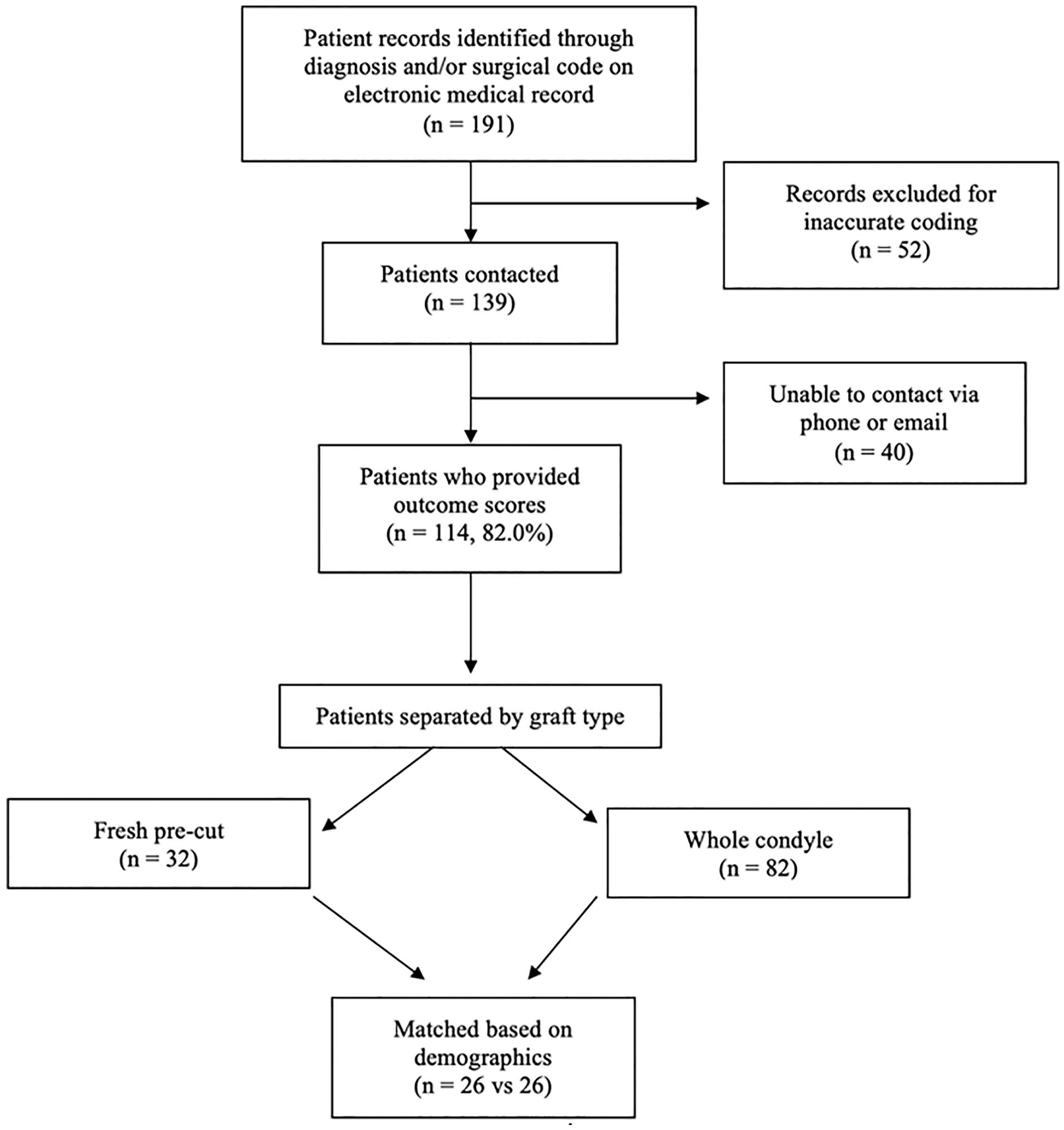
Flow chart of patient inclusion/exclusion.
Patient Demographics.
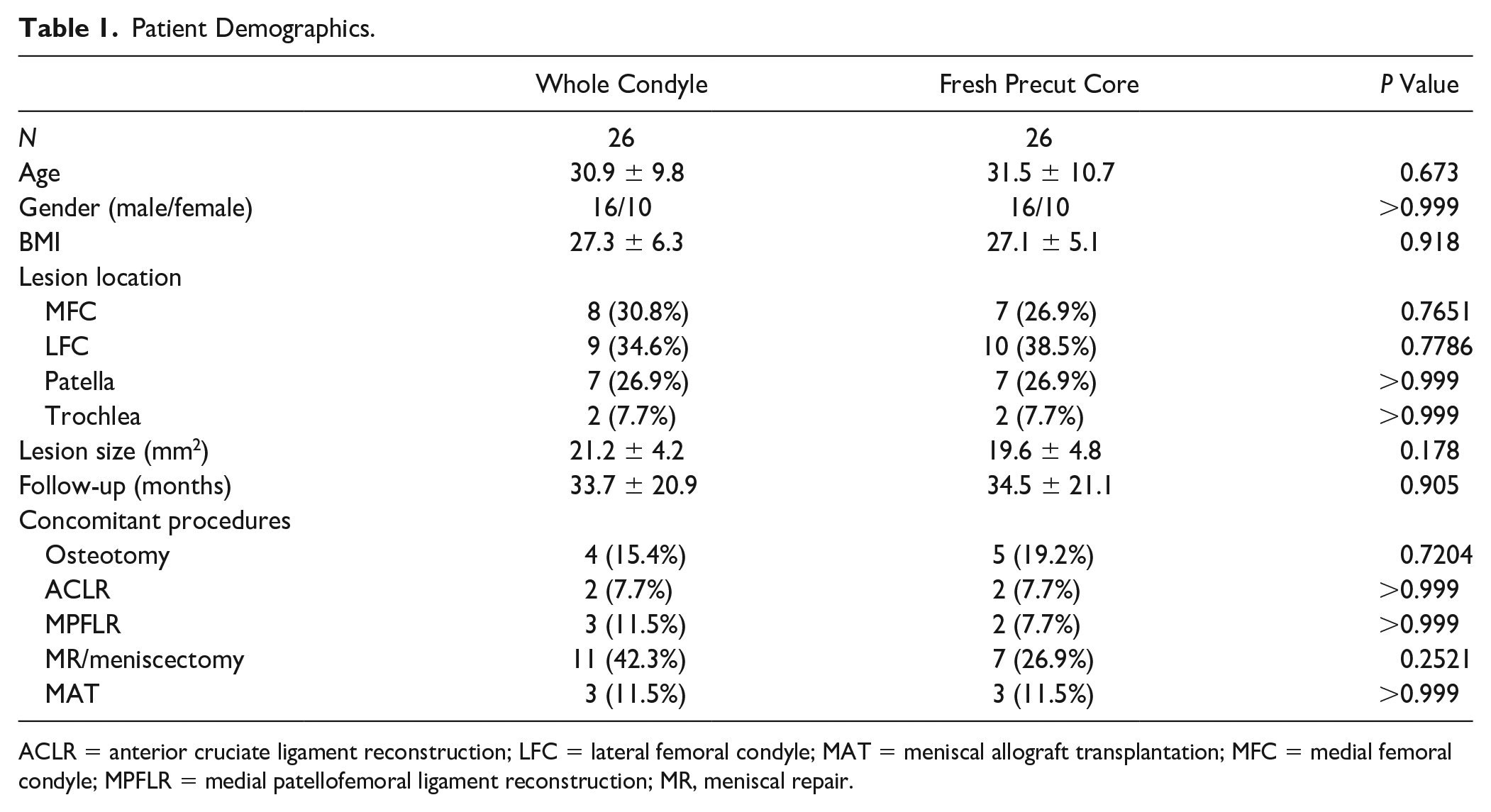
ACLR = anterior cruciate ligament reconstruction; LFC = lateral femoral condyle; MAT = meniscal allograft transplantation; MFC = medial femoral condyle; MPFLR = medial patellofemoral ligament reconstruction; MR, meniscal repair.
Patient-Reported Outcomes
At a mean follow-up of 33.7 ± 20.9 months and 34.5 ± 21.1 months (P = 0.905), there were no significant differences in any patient-reported outcomes ( Table 2 ).
Patient-Reported Outcomes.
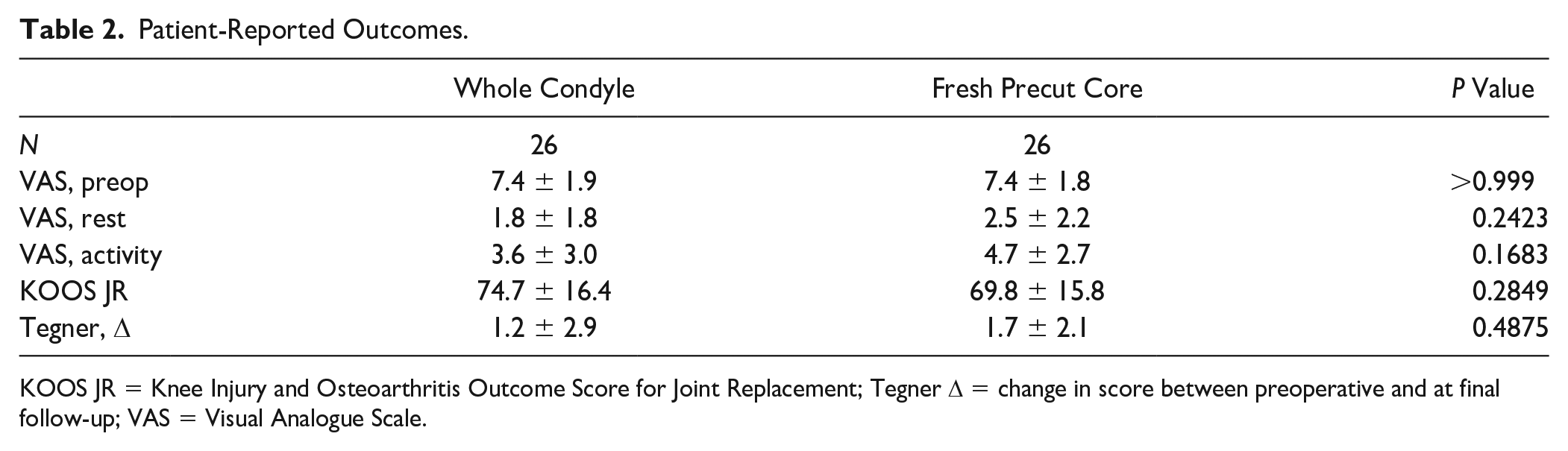
KOOS JR = Knee Injury and Osteoarthritis Outcome Score for Joint Replacement; Tegner Δ = change in score between preoperative and at final follow-up; VAS = Visual Analogue Scale.
Subgroup Patient Characteristics
Among the cohort of fresh precut core patients, 16 of the 26 (61.5%) received postoperative MRIs based on surgeon preference. This subgroup did not demonstrate statistical differences for any demographic parameter compared to the original cohort (P > 0.05). Of these 16 patients with MRIs, 11 could be appropriately matched to patients who had received whole condyle allografts based on age, follow-up, lesion size, lesion location, and BMI. The subgroup patient characteristics can be found in Table 3 .
Subgroup Patient Characteristics.
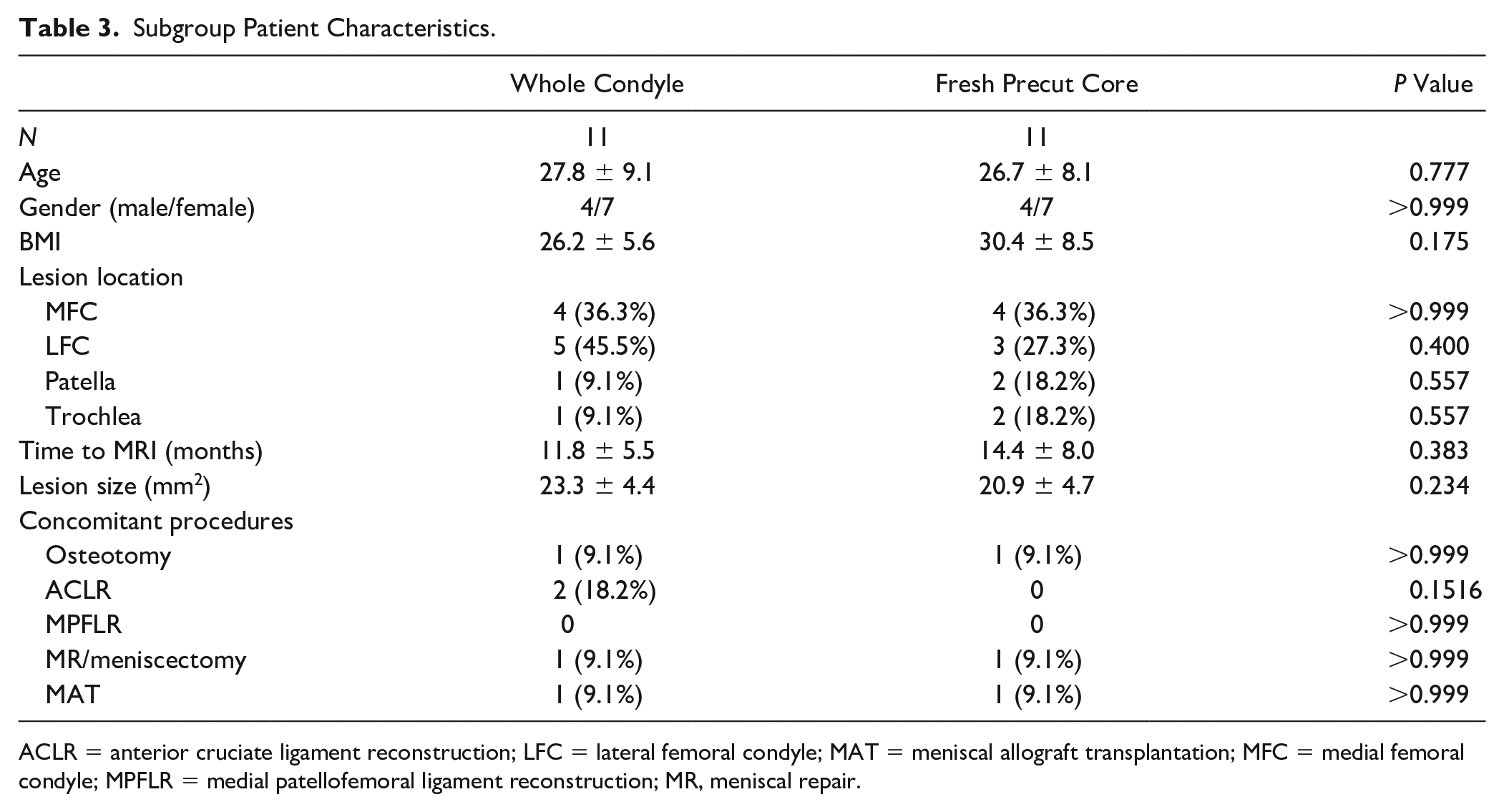
ACLR = anterior cruciate ligament reconstruction; LFC = lateral femoral condyle; MAT = meniscal allograft transplantation; MFC = medial femoral condyle; MPFLR = medial patellofemoral ligament reconstruction; MR, meniscal repair.
Radiographic Analysis
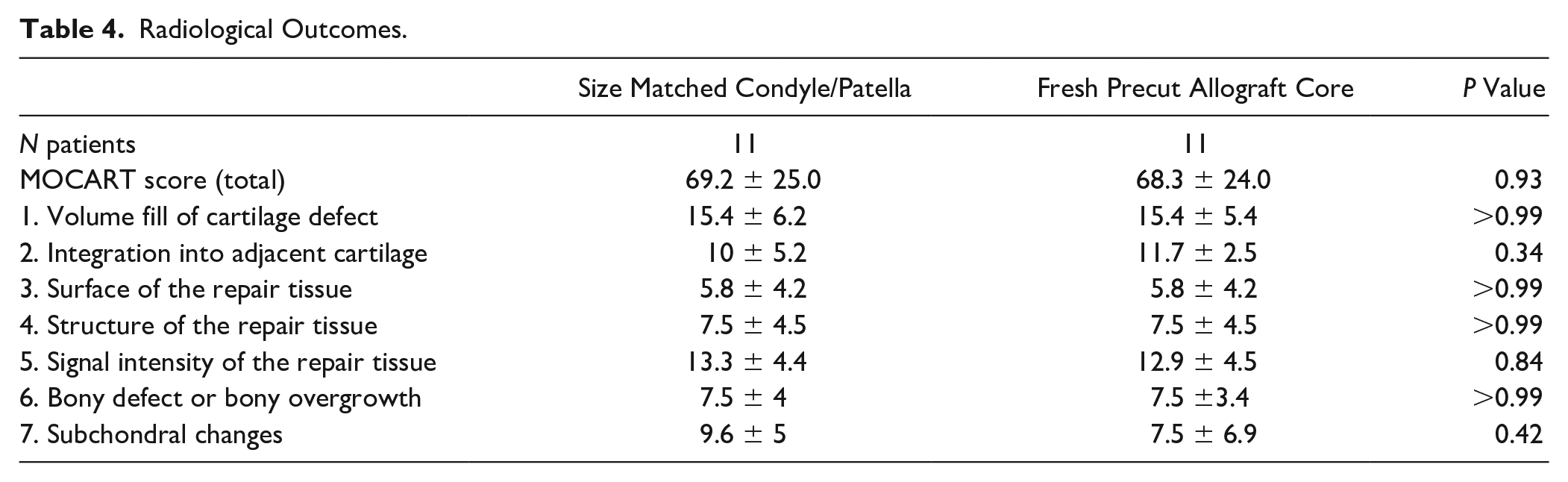
There was no significant difference in total MOCART score (69.2 vs. 68.3, P = 0.93), or in any subscore (P > 0.05 for all) between the treatment groups. Further details are illustrated in Table 4 .
Radiological Outcomes.
Discussion
The most important finding in our study was that there was no difference in MOCART or PRO scores between fresh precut OCA cores and size matched condylar/patella OCA following osteochondral transplantation. The findings of the current study indicate no difference in early to midterm graft healing between either method. However, these findings are limited to the initial postoperative phase and it is still unclear whether the lack of early radiologic differences translate to equivalent clinical outcomes in long-term follow-up.
The literature has shown OCA to be an excellent option for patients with chondral lesions. A recent study by Frank et al. 15 found 87% survivability of condylar OCA at 5 years following transplantation. Furthermore, a systematic review Assenmacher et al. 16 found a 75% survivorship following OCA at a minimum of 10 years. Beyond excellent rates of survivorship, patients have demonstrated improvement in pain, function, and PRO scores following OCA. 17 Similarly, our study identified significantly improved PRO scores from preoperative to postoperative evaluation, regardless of graft type. Furthermore, there was no difference found in the PRO scores between fresh precut and size matched condylar/patella OCA groups. Our findings parallel previous literature on condyle-specific matching for OCA, which demonstrated no difference in midterm outcomes between patients who underwent orthotopic versus nonorthotopic OCA.18,19
Our study suggests the noninferiority of fresh precut OCA cores when compared to size matched condylar/patella OCA. Magnetic resonance evaluation of our patients’ implantation sites revealed no statistically significant difference between the size matched condylar/patella grafts and precut OCA cores as measured by MOCART scores. Imaging assessments have shown that early and midterm evaluation of graft stability may reveal clinically relevant information regarding the overall results of cartilage restoration procedures like OCA.20,21 Although the literature comparing imaging assessments between orthotropic and nonorthotopic OCA is exceedingly limited, the existing studies have displayed comparable scores between the two.20,22-25 This aligns with the findings in our study demonstrating no difference in the imaging analysis of fresh precut OCA cores compared to size matched condylar grafts.
Fresh precut allograft cores offer an advantage with regards to expediency of surgery. 26 Prolonged wait times for surgery are a concern particularly in the young, active population, in whom the literature has shown that continued weight-bearing on the lesion can cause possible progression in size and severity.27,28 Recent studies have demonstrated that nonorthotopic grafts can still achieve excellent surface matches at the recipient site. Precut OCA cores can therefore reduce surgical delays by obviating the need for orthotopic, size matched grafts.18,19 Surgeries can also be scheduled at convenience for the patient, as the precut grafts can be stored for up to 35 days, and negate the waiting time for donor OCA matching. 26 Furthermore, in high-volume centers, grafts can be stored with minimal potential risk of waste. However, it is still unclear how the different storage mediums and storage times affect OCA viability. Merkely et al. 29 found in a 5-year retrospective analysis that hemicondyle grafts stored for 25 days or fewer were 3.4 times less likely to fail compared to grafts with prolonged storage, but it is unclear if this prolonged storage time also affects precut OCA graft failure. Furthermore, there is a difference in storage mediums used between the OCA preparations, and in those with precut OCA the subchondral bone and cartilage-bone interface is exposed to the medium which could impact cellular viability.
Furthermore, there are significant cost differences between precut OCA cores and hemicondyles used for OCA transplantation. Despite the similar outcomes, precut OCA cores were found to be a fraction of the cost of the hemicondylar grafts, with a 10 mm plug costing approximately one fifth the price of a hemicondyle. 26 Furthermore, while a majority of graft requests are for lesions of the medial femoral condyle, lateral condyles comprise an estimated three quarters of available grafts. Consequently, as many as 13% of these harvested condyles are unable to be utilized in the mandatory time frame and must be discarded. 18
Further study is still needed to assess the utilization and optimization of different OCA grafts, which could lead to both improvements in clinical outcomes and decreased costs. Recent studies have sought to optimize the storage of OCA grafts, to have a longer shelf life and higher cell count for viability, which may lead to improved cartilage quality in the implanted graft.30,31 Beyond this, there are differences in storage and preparation between the fresh precut OCA cores and condylar OCA, which could impact outcomes and cell viability. However, despite our study showing no difference in the early radiologic outcomes, further optimization is still of great interest. Studies with longer term follow-up and clinical outcomes are needed to assess whether or not a true difference exists, as despite the short-term benefits studies have shown that a quarter of patients will have a failure at 10 years of follow-up. Finally, the MOCART 2.0 knee score was introduced within the past 2 years. 32 It does not have a significant amount of literature validating it as of yet, with most current literature still utilizing the original MOCART scoring system. Thus, the use of the original MOCART scoring system remains valid. However, it would be interesting to see if using the MOCART 2.0 system substantially impacts the results of this study. Further study is warranted.
Limitations
This study is limited due to the relatively small cohort and short-term follow up. Furthermore, follow-up times may be skewed by a handful of patients with relatively long-term follow-up. The patients were matched by the research team retrospectively. While not all demographic factors could be matched perfectly, it was of utmost importance to match the 2 groups as closely as possible. It has been shown that storage time can impact outcomes after OCA 29 ; however, the graft storage times for the included patients were not available and may impact the demonstrated findings. The absence of radiologic differences within the early follow-up period may not have been present were the cohorts examined at a greater interval from transplantation. It is unclear then whether the similarity in radiologic outcomes would continue to be observed in future evaluation.
Additionally, the nonuniform utilization of both 1.5 T and 3 T magnets may be another limitation. However, it should be noted that it is common to see utilization of both magnet strengths within the same study throughout the existing literature.18,20,21,23,24 Although uniformity is certainly preferable, the apparent interchangeability in the current literature suggests the difference between 1.5 T and 3 T magnets is unlikely to significantly impact our findings. The use of one radiologist as opposed to two can be considered a limitation, though is unlikely to impact the current findings.
Another limitation of this study was that only approximately two thirds of patients within the cohort underwent MRI. This study was performed at a large academic institution, as such patients may undergo OCA with a number of surgeons within the sports medicine department. As each surgeon has a different preferred protocol for follow-up, not all surgeons routinely require follow-up MRIs. Furthermore, if patients move out of the area, they are unable to come back for imaging. As a retrospective unfunded study, we did not feel it was viable (particularly given the COVID-19 pandemic) to bring patients back only for the purposes of research MRI. Therefore, we had to utilize the MRIs that were available. We have run subgroup analyses prior, indicating that there is no statistical significance in any patient demographic between those who underwent MRI and those who did not (P > 0.05).
Finally, a subgroup post hoc analysis for each outcome was performed determining that 178 patients would be required (alpha 0.05, power 0.8) to determine any difference in subgroup MOCART score. Additionally, a post hoc analysis of clinical outcomes determined that 234 patients would be required (alpha 0.05, power 0.8) to determine any difference in VAS score.
Conclusion
This study did not appreciate a difference in patient reported clinical outcomes or MOCART scores following OCA implantation using fresh precut OCA cores or size matched condylar grafts at early to midterm follow up.
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the local institutional review board (i20-01168).
Informed Consent
Verbal informed consent was obtained from all subjects before the study.