
Abstract
Objective
This systematic review aimed to determine whether coronal angular corrections correlate with patient reported outcomes following valgus-producing high tibial osteotomy (HTO).
Design
Ovid MEDLINE, Embase, and Web of Science were systematically searched. Studies that reported hip-knee-ankle angles (HKA) or femorotibial angles (FTA), and the Oxford Knee Score (OKS), visual analogue scale (VAS) score, Knee Injury and Osteoarthritis Outcome Score (KOOS), or EQ-5D before and after valgus-producing HTO were eligible. Correlation analyses were performed where appropriate to investigate the relationships between variables. PROSPERO ID: CRD42019135467.
Results
This study included 39 articles including 50 cohorts. VAS was reported in 22 studies, OKS in 9, KOOS in 12 and EQ-5D in 2. The HKA angle was corrected from 7.1° ± 1.7° varus to 2.3° ± 1.7° valgus at final follow-up. The FTA changed from 3.0° ± 2.0° varus to 7.7° ± 1.3° valgus. Outcome scores improved with clinical and statistical significance postoperatively. Spearman correlations for nonparametric data revealed greater changes in knee alignment were moderately associated with larger improvements in VAS scores (r = 0.50). Furthermore, those who experienced greater changes in alignment showed larger improvements in the KOOS Activity and Quality of Life domains (r = 0.72 and r = 0.51, respectively).
Conclusion
On average, patients did not achieve the “ideal correction” of 3° to 6° valgus postoperatively. Nevertheless, statistical and clinical improvements in patient-reported outcome measure scores were consistently reported. This suggests that the “ideal correction” may be more flexible than 3° to 6°.
Introduction
Osteotomies of the knee have been shown to be suitable for the treatment of predominantly unicompartmental knee osteoarthritis (OA) in active and young patients. As a result, they are growing in popularity amongst clinicians and patients. 1 High tibial osteotomy (HTO) is the most commonly performed osteotomy in patients with isolated medial knee OA. HTO preserves the native joint by realigning the tibia to offload the worn areas of the knee and relieve pain by shifting the load bearing out of the diseased compartment. According to the United Kingdom Knee Osteotomy Registry (UKKOR) and Osteoarthritis Research International this intervention can delay the progression of OA, postponing the need for a knee replacement by up to 10 years in some patients, and preventing the need for further surgical intervention in others.1,2 However, realignment of the joint by HTO is a complicated procedure, as each knee is individual in terms of its natural anatomy and bony deformity. 3 The bony deformities that develop as a result of OA are also often multiplanar. This is problematic as surgeons may be limited to biplanar X-rays preoperatively. 4 Consequently, surgical planning of HTOs can be complex.
Traditionally, surgeons aim to correct the alignment of the knee so that the Mikulicz line, a straight line connecting the center of the hip and center of the ankle, passes through a point which is 62.5% along the tibial plateau from the medial edge. 5 This point is known as the Fujisawa point. Due to the precision needed to achieve this alignment, it is not surprising that HTOs can result in joint alignment other than what was planned, which in turn may increase the risks of failure and revision. 3
A recent systematic review on the accuracy of knee osteotomies found that of 966 HTO procedures, approximately 10% (9.9%) failed to achieve a limb alignment that was within 20% of the intended correction (typically a hip-knee-ankle angle of 3°-6° valgus 6 ).4,7,8 Furthermore, fewer than 40% (35.7%) achieved an alignment that was within 5% of the operative plan. 7 From the current literature, it remains unclear whether failing to achieve the ideal correction postoperatively impacts clinical outcome and patient satisfaction. 4 We therefore do not know whether achieving the “ideal correction” of 3° to 6° valgus for HTO is truly necessary for a good clinical outcome.
The aim of this systematic review was to determine whether correction angle correlates with clinical outcome following HTO for medial knee OA.
Methods
This systematic review was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. The protocol of this review is registered on PROSPERO [ID: CRD42019135467; https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=135467].
Search Strategy
Systematic searches of the literature were carried out in 3 databases: Ovid MEDLINE, Embase, and Web of Science. The resources used within each database were as follows: Ovid MEDLINE and Epub Ahead of Print, In-Process & Other Non-Indexed Citations, Daily and Versions 1946 to June 3, 2019; Embase 1974 to June 3, 2019; Web of Science All Years 1900 to June 3, 2019. PROSPERO was also searched for ongoing or unpublished systematic reviews. The databases were searched for a final time on October 27, 2020 to identify any relevant literature that may have been published between June 3, 2019 and October 27, 2020.
The search terms used in this systematic review: Osteoarthritis OR Knee Osteoarthritis [All Fields] AND Osteotomy OR Osteotomy OR Tibia osteotomy OR Tibia proximal osteotomy [All Fields].
Eligibility
Once primary searches of the databases had been completed, the studies were reviewed for inclusion. This was done in 2 phases—first, by title and abstract only (reviewers: GT and HS), and later by reviewing the entire publication (reviewers: GT and HS). A third independent reviewer (LB) was available where reviewers disagreed on whether a publication should be included in the review or not.
Studies were included in this systematic review if they fulfilled the following inclusion criteria:
Included patients who have undergone a HTO to treat medial knee OA of any severity.
Reported at least one predetermined patient-reported outcome measure (PROM) pre- and postoperatively (see below).
Reported pre- and postoperative alignment.
Reported mean age of participants.
Written in the English language.
Levels of evidence of I to IV.
The exclusion criteria for this systematic review were as follows:
Included patients who have undergone a HTO for any reason other than medial knee OA (e.g., trauma).
Included patients who have undergone HTO in combination with another procedure.
Cadaveric studies.
Animal or cell studies.
Computer or mathematical model studies.
Did not report any of the pre-determined PROMs (see below).
Did not report pre- and postoperative alignment.
Did not report mean age of participants.
Presented data in a format whereby the values could not be extracted from the article.
Studies where HTO was compared with another surgical treatment (most commonly unicompartmental knee replacement) were included if they fulfilled the inclusion criteria. Abstracts, case reports, book chapters, and conference proceedings were also reviewed for inclusion in this review.
Given the fact that there are numerous methods of quantifying functional outcome following HTO, it was important to predetermine our variables of interest. Studies that used at least one of the following PROMs and fulfilled all other inclusion criteria were included in this systematic review:
Oxford Knee Score (OKS)—A joint specific questionnaire that asks patients on the level of pain and function they believe to have in their affected knee.
EQ-5D—A questionnaire on patients’ perception of their overall health.
Visual analogue scale (VAS)—A scale of 0 to 100 for level of pain felt.
Knee Injury and Osteoarthritis Outcome Score (KOOS)—Similar to the OKS, this is a joint-specific PROM. It covers themes in addition to pain and function, including activity, sports, and recreation.
These PROMs were specifically chosen over others, as they are recommended by UKKOR for reporting outcome following knee osteotomy. 1
Study Quality
The quality and risk of bias of all potentially eligible studies included in the full-text review were assessed by 2 reviewers (GT and HS) using the National Institute of Health Quality Assessment Tool. This tool can be tailored to numerous study designs, enabling researchers to evaluate the validity of any published study. At the researchers’ discretion, studies are graded “good,” “fair,” or “poor” based on answers given to a series of criteria relevant to research design and implementation. Eligible studies that were graded as “good” or “fair” were included in the review.
Data Extraction and Synthesis
All data were extracted independently by 2 reviewers (GT and HS) into a Microsoft Excel spreadsheet. Any discrepancies were settled by a third independent reviewer (LB). The data extracted included pertinent study information (author, year of publication, level of evidence, study design, published format, quality, length of follow-up), surgical information (type of HTO, fixation type), and participant information (mean pre- and postoperative valgus/varus alignment, number of males and females, mean age, mean body mass index [BMI], mean OA grade, and grading system used). The mean results from the above-stated PROMs were also extracted.
Statistical Analyses
All postoperative PROMs and radiographic alignments were tested for normality. Correlation analyses were carried out where sufficient data were available. Pearson correlations were carried out on normally distributed data to determine whether postoperative PROM scores correlated with postoperative correction. Spearman correlations were carried out on nonnormally distributed data. Correlations were classed as weak when r = 0.01 to 0.29, moderate when r = 0.30 to 0.49, strong when r = 0.50 to 0.90, and perfect when r = 0.91 to 1.00. 4 Statistical analyses were carried out in Microsoft Excel software.
Results
Search Results
Thirty-five articles initially fulfilled the inclusion criteria for this review, but after a final search of the literature in October 2020, 4 further articles were included ( Fig. 1 ). Six articles had a level of evidence of II (15.4%). Twenty-three (59.0%) had a level of evidence of III, and the remaining 10 (25.6%) had a level of evidence of IV ( Table 1 ). Five (12.8%) studies were randomized controlled trials, 23 (59%) were prospective cohort studies, and 8 (20.5%) were retrospective cohort studies. Three case series were included in this review (7.7%) ( Table 1 ).
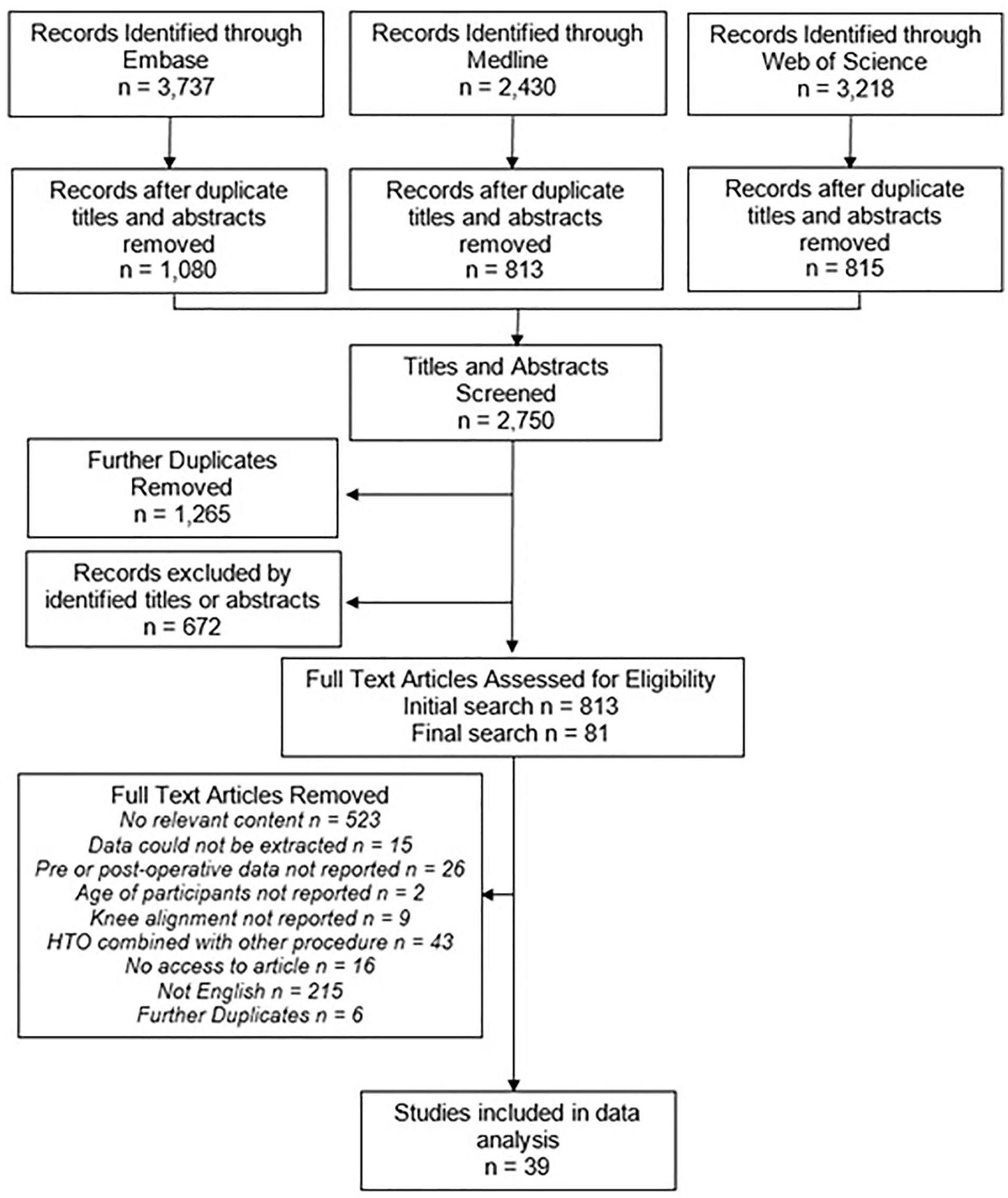
Flowchart of systematic search.
Pertinent Information About the Studies Included in This Systematics Review.
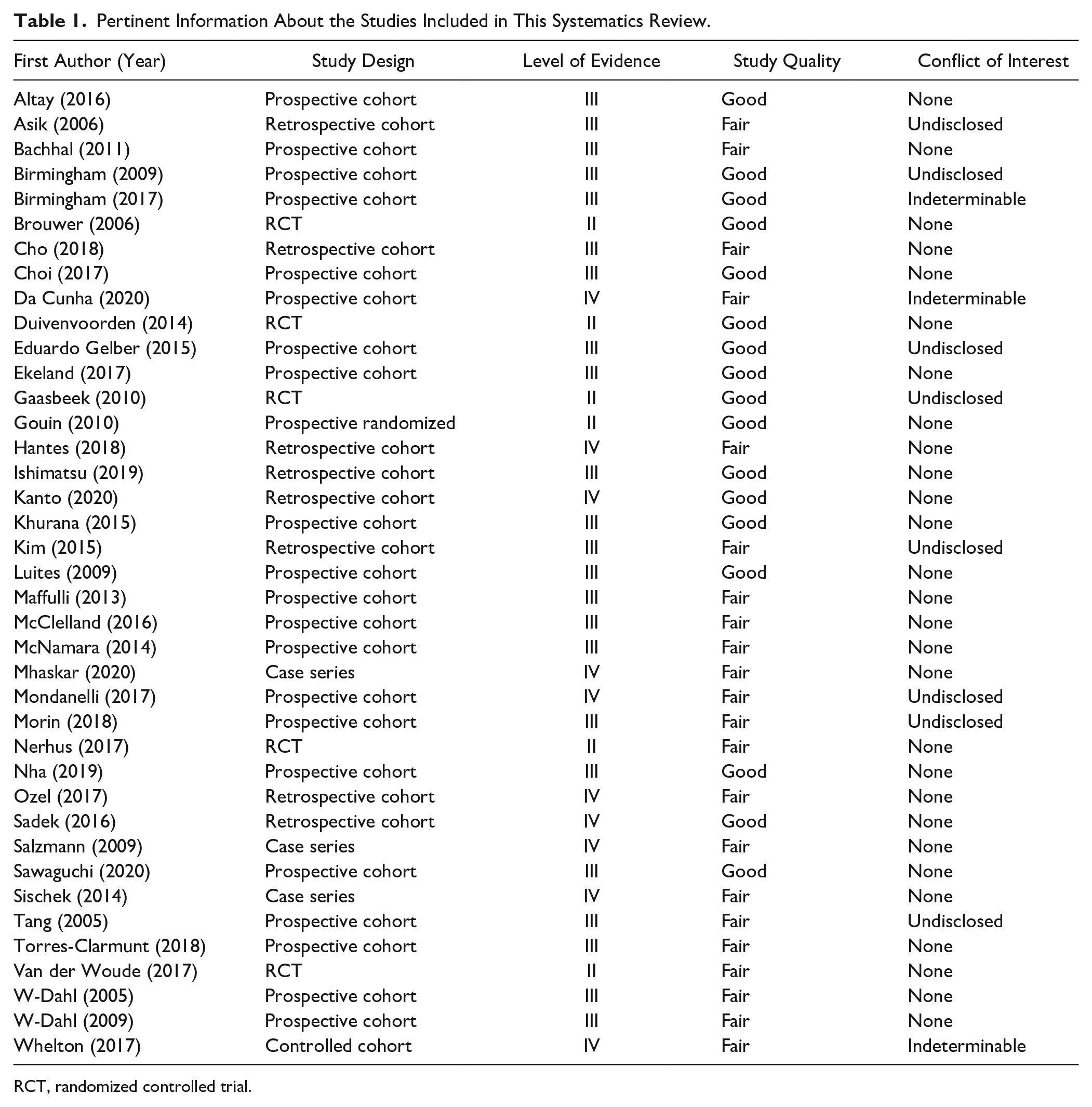
RCT, randomized controlled trial.
The most commonly reported PROM was the VAS (22/39, 56.4%). The OKS was reported in 9 articles (23.1%). KOOS subscores (KOOS Pain, KOOS Activity, KOOS Symptom, KOOS Sport, and KOOS Quality of Life) were reported in 12 articles (30.8%). An additional article reported the KOOS Pain score by itself (2.6%). The EQ-5D was reported in 2 studies (5.1%).
Eleven articles (28.2%) compared the outcomes of 2 cohorts of participants with HTO. As such, this review analyzed the results of 50 cohorts.
Quality Assessment
No articles were excluded from this review due to their quality being graded as “poor.” Twenty-two were graded as being of “fair” quality (56.4%), and the remaining 17 were determined to be of “good” quality (43.6%) ( Table 1 ). In general, articles scored well in their descriptions of the study aims and populations. They also scored well in questions on the methodology and participant retention in the study. However, the description of statistical analyses or sample size calculations were often poor or not reported. Furthermore, comparative studies rarely explained whether the researchers were blinded to the patient’s group, introducing a potential source of bias.
With regard to conflicts of interest, 28 (71.8%) studies declared not to have any ( Table 1 ). Eight studies (20.5%) did not disclose whether there was a conflict of interest or not. One study by Birmingham and colleagues disclosed that the authors were associated with the company Arthrex (specifically during conduct of study), Athrosurface, Smith & Nephew, and DePuy. 9 However, there was no mention in the article of whether the implant or instrumentation used in the study were manufactured by any of the named companies. Da Cunha et al. 10 declared paid consultancies with Smith & Nephew; the same company supplied the external fixators for the HTOs included in their research study. Finally, the source of funding in Whelton’s study was disclosed, but it was not clear whether there was a conflict of interest. 11 Consequently, potential sources of bias in this review may result from the undisclosed or unclear conflicting interests in 10 of the studies.
Participant Characteristics
Demographics
This systematic review included 2,341 patients across 50 cohorts. The numbers of males and females in 3 cohorts was not provided12,13 ( Table 2 ). However, of the remaining 47 cohorts, there were 1,429 males and 785 females (64.5% vs. 35.5%). The average age across all cohorts was 50.8 ± 6.4 years (range: 29-66 years). The average BMI was estimated at 27.6 ± 1.9kg/m2 (range: 23.6-30.9 kg/m2); however, BMI was only reported for 38 cohorts (76.0%) ( Table 2 ).
Demographics of the Patients Included in the Research Studies Eligible for This Systematic Review.
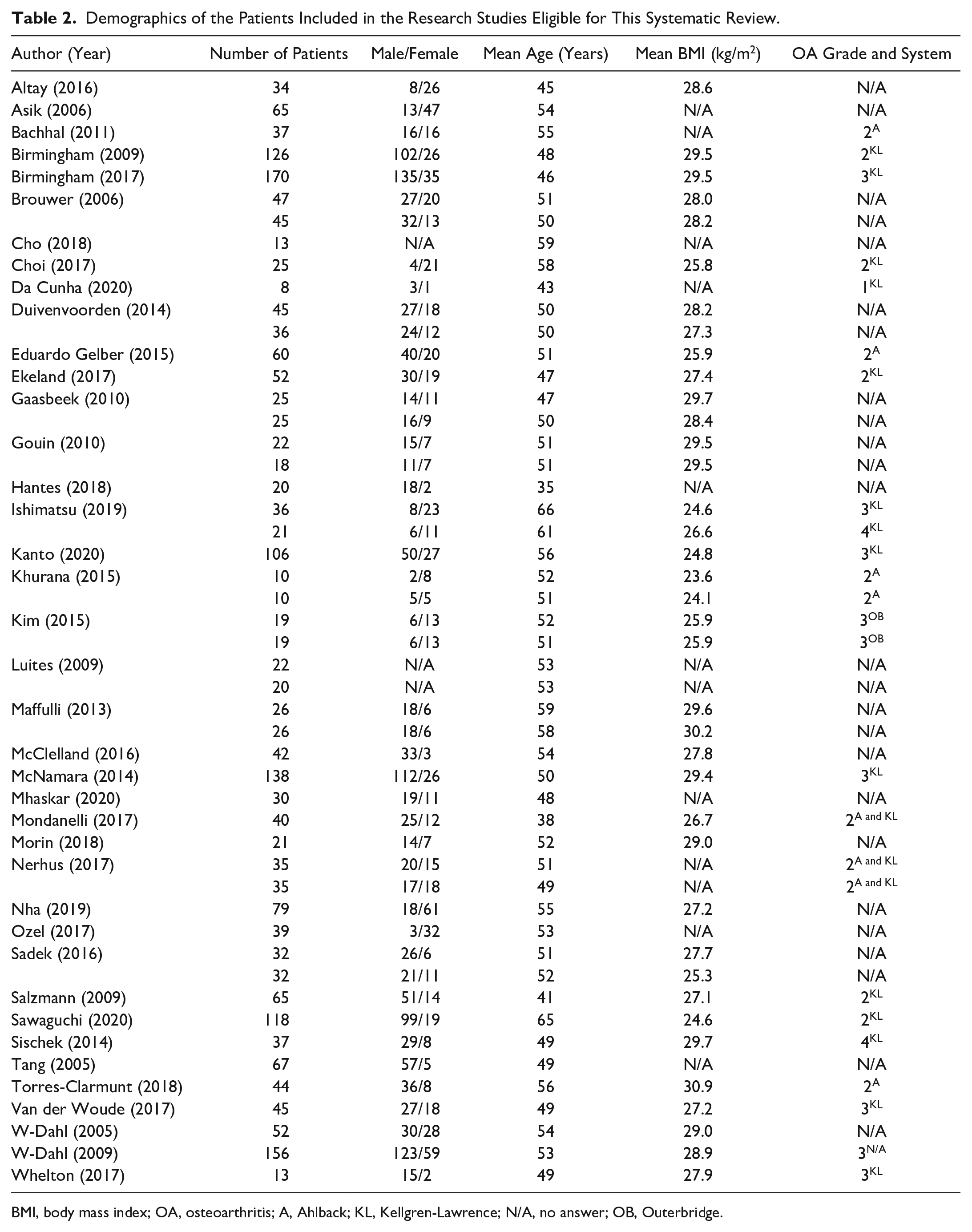
BMI, body mass index; OA, osteoarthritis; A, Ahlback; KL, Kellgren-Lawrence; N/A, no answer; OB, Outerbridge.
Osteoarthritis Severity
The graded severity of osteoarthritis in the knee was described for 24 cohorts (48.0%) ( Table 2 ). Seventeen cohorts (34.0%) were graded by the Kellgren-Lawrence score. The mean grade was 2.5 ± 0.8 across the cohorts (range: 1-4). Eight cohorts (16.0%) were graded with the Ahlback score. The mean grade was reported as 2 in each cohort. Finally, the Outerbridge score was used with 2 cohorts (4.0%). Both cohorts had a mean score of 3.
Surgery and Follow-Up
The mean follow-up was 46.8 months (range: 8-170 months), although 1 study did not report the length of follow-up ( Table 3 ). 10 Thirty-seven of the cohorts (74.0%) underwent a medial open wedge HTO (MOWHTO), 9 underwent a lateral closing wedge HTO (18.0%) (LCWHTO), 3 underwent a hemicallostasis (6.0%), and 1 underwent a hybrid LCWHTO (2.0%). Only 1 cohort had their HTO performed with computer navigation (2.0%) ( Table 3 ).
Study-Specific Data and Results of Studies Included in This Systematic Review a .
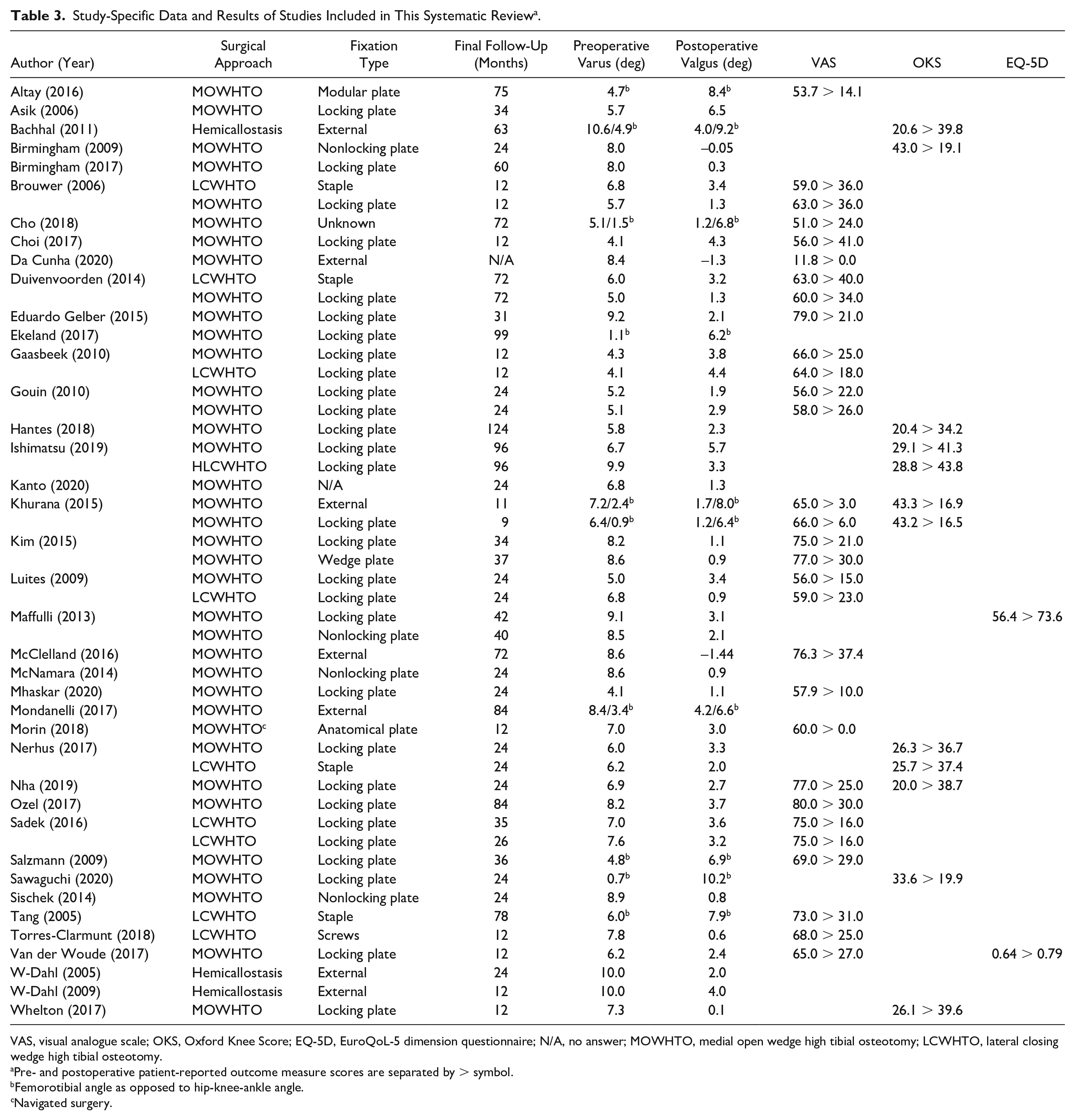
VAS, visual analogue scale; OKS, Oxford Knee Score; EQ-5D, EuroQoL-5 dimension questionnaire; N/A, no answer; MOWHTO, medial open wedge high tibial osteotomy; LCWHTO, lateral closing wedge high tibial osteotomy.
Pre- and postoperative patient-reported outcome measure scores are separated by > symbol.
Femorotibial angle as opposed to hip-knee-ankle angle.
Navigated surgery.
In general, locking plate and screws were used to fix the HTO (29/50, 58.0%). External fixation was used in 7 cohorts (14.0%) (one specifying it being a dynamic axial fixator 14 ), staple fixation in 4 (8.0%), and a nonlocking plate and screws in 4 cohorts (8.0%). The remaining 4 cohorts used screws, a modular plate and screws, an anatomical plate, a wedge plate, and screws. Two articles (4.0%) did not describe the fixation type used with their patient cohorts ( Table 3 ).12,15
Radiographic Outcomes
Pre- and postoperative hip-knee-ankle (HKA) angles were reported in 45 of the 50 cohorts (90.0%). The femorotibial angle (FTA) was reported in 10 cohorts (20.0%) ( Table 3 ). The HKA angle is defined as the angle formed at the intersection between the mechanical axes of the femur and tibia. The mechanical axis of the femur is measured as a straight line between the hip joint center and knee joint center, whereas the mechanical axis of the tibia is measured as a straight line between the knee joint center and the ankle joint center. The HKA angle is thus measured from anteroposterior full-limb plain radiographs. The FTA is defined as the angle formed at the intersection of the anatomical axes of the femur and tibia. The anatomical axis of the femur is measured as a straight line down the femoral shaft, and the anatomical axis of the tibia is measured as a straight line down the tibial shaft. The anatomical axes of the femur and tibia are usually measured 10 cm proximal and 10 cm distal from the knee joint surfaces on anteroposterior standing plain radiographs, respectively. 16
The mean preoperative HKA angle was 7.1° ± 1.7° varus (range: 4.1°-10.6°). This was corrected on to a mean of 2.3° ± 1.7° valgus at final follow-up (range: −1.4° to +6.5°); a difference of 9.4° ± 2.2° (range: 5.2°-14.6°). The mean preoperative FTA was 3.0° ± 2.0° varus (range: 0.7°-6.0°). This improved to an average 7.7° ± 1.3° valgus postoperatively (range: 6.2°-10.2°); a difference of 10.7° ± 2.5° (range: 7.3°-14.1°).
Clinical Outcomes
Visual Analogue Score
The mean preoperative VAS across all cohorts was 63.8 ± 12.9 (range: 11.8-80.0). This improved to 22.7 ± 11.3 (range: 0.0-41.0) at final follow-up ( Table 3 ); a difference of 41.1 ± 13.6 (range: 11.8-62.0). This is greater than the minimum clinically important difference, which has previously been estimated to be between 22.6 and 30.0.17,18
Spearman correlations revealed a weak relationship between HKA alignment and postoperative VAS (r = 0.11) across the 27 eligible cohorts. The correlation between postoperative VAS and FTA was also weak (r = −0.09, Spearman correlation).
However, there was a moderate to strong correlation between the differences in pre- and postoperative HKA alignment and VAS (r = 0.50, Spearman correlation), implying that greater changes in alignment are associated with larger improvements in pain scores. The change in pre- to postoperative FTA alignment did not correlate with the pre- to postoperative changes in VAS, however (r = −0.14, Spearman correlation).
Many studies included in this review investigated the outcomes of MOWHTO.12,19-25 Although the populations and approaches varied between studies, statistically significant improvements in the VAS were observed in the majority of cohorts postoperatively. Da Cunha and Mhaskar also found the VAS to improve following bilateral MOWHTO. The improvements observed in VAS in Mhaskar’s study were statistically significant.10,26 However, 1 patient from Cho’s study underwent a subsequent knee replacement due to severe postoperative pain, highlighting that pain scores do not improve universally for all patients. 12
Gouin and colleagues compared the outcomes of MOWHTO with calcium phosphate ceramic spacers to autologous bone grafts. 27 Patients who had autologous bone grafts had significantly better pain scores at 3 months (P = 0.04), but these differences were insignificant after 6 months.
Khurana et al. 14 compared the outcomes of MOWHTO with Tomofix (plate) and Orthofix (external fixator). Statistical analyses were not carried out on the VAS results, but significant improvements were observed in both groups. 14 Similar findings were reported by Kim et al., 28 who also compared different types of fixators (wedge plate vs. locking plate), and by McClelland et al., 29 whose fixator of choice was external.
Multiple studies compared the outcomes of MOWHTO and LCWHTO.13,30-33 VAS scores were shown to improve in all cohorts postoperatively, but there were no differences between MOWHTO and LCWHTO as long as 6 years postoperatively.
In their study on survival of LCWHTO, Tang and colleagues reported that 9% of patients reported an increase in pain or no change in pain scores postoperatively, but on average the scores improved significantly over time. 34 Statistically significant improvements following LCWHTO were also observed by Torres-Claramunt et al. 35 and Sadek et al. 36
Oxford Knee Score
Of the 9 studies that reported the OKS, 6 used the current scoring system, which has a maximum and best score of 48 ( Table 3 ). The mean preoperative OKS across these 6 studies was 24.6 ± 3.8 (range: 20.0-29.1).11,21,37-40 This increased to 38.9 ± 2.9 postoperatively (range: 34.2-43.8); a difference of 14.3 ± 3.0 (range: 10.4-19.2). This is greater than the minimum clinically important difference, which has previously been estimated to be between 4.0 and 5.0 in similar populations.41,42
The 3 remaining studies used the old scoring system for the OKS, which gives an overall score of 12 to 60, with 12 being the best outcome.28,43,44 The mean OKS improved from 40.8 ± 4.8 (range: 33.6-43.3) preoperatively to 18.1 ± 1.7 (range: 16.5-19.9); an improvement of 22.7 ± 5.3 (range: 13.7-26.7).
There were moderate correlations between postoperative HKA with current OKS (r = 0.48, Spearman correlation). Correlations between the differences in HKA and current OKS were also moderate (r = 0.33, Spearman correlation).
Two studies (4 cohorts) that had reported the OKS using the old scoring system reported both HKA and FTA alignments, while an additional study reported only the FTA. A perfect positive correlation was observed between postoperative HKA and FTA alignments and the old OKS (r = 1.00 for HKA and r = 1.00 for FTA, Spearman correlations). This suggested a more valgus alignment postoperatively was associated with a worse OKS result. Furthermore, strong to perfect negative relationships were found between the differences in alignments and old OKS (HKA r = −1.00 and FTA r = −0.80, Spearman correlations), suggesting that a greater change in alignment was associated with a worse score. This contradicted the findings of the current OKS.
Asik et al., 37 Nha et al., 21 Sawaguchi et al., 44 and Whelton et al. 11 all reported statistically significant improvements in OKS following MOWHTO (P < 0.001). Hantes and colleagues 38 also reported significant improvements in OKS post-MOWHTO, but their patients were younger than 45 years and active at the time of surgery (P < 0.05). This score was sustained until the final follow-up 12.3 years postoperatively.
Khurana and colleagues compared 2 cohorts of MOWHTO patients: One group underwent MOWHTO with a dynamic axial fixator (Orthofix) and the second group underwent MOWHTO with a locking compression plate (Tomofix). 14 Statistically significant and clinically important improvements were observed between baseline and final follow-up, but differences between groups did not reach significance.
Ishimatsu et al. 39 compared the outcomes of MOWHTO and hybrid LCWHTO. As in Khurana’s study, both groups experienced statistically significant improvements in OKS, but there were no significant differences between the groups postoperatively. This was also observed by Nerhus and colleagues; Patients were followed up for 2 years, and at no point were the differences in OKS between cohorts statistically significant ( Table 3 ). 41 On average, the score improved to a clinically significant extent in both groups, but improvements were only statistically significant between cohorts during the first postoperative year.
Bachhal et al. 43 reported the outcome of HTO by hemicallostasis and external dynamic fixator. In this study, the OKS improvement in score was statistically significant between 1 and 2 years postoperatively.
Knee Osteoarthritis Outcome Score
Twelve studies reported the KOOS’s 5 domains, and a further study reported the KOOS pain score in isolation ( Table 3 ). All subscores improved by a clinically important degree postoperatively (Table 4). 45
Mean KOOS Subscores Across All Eligible Articles.
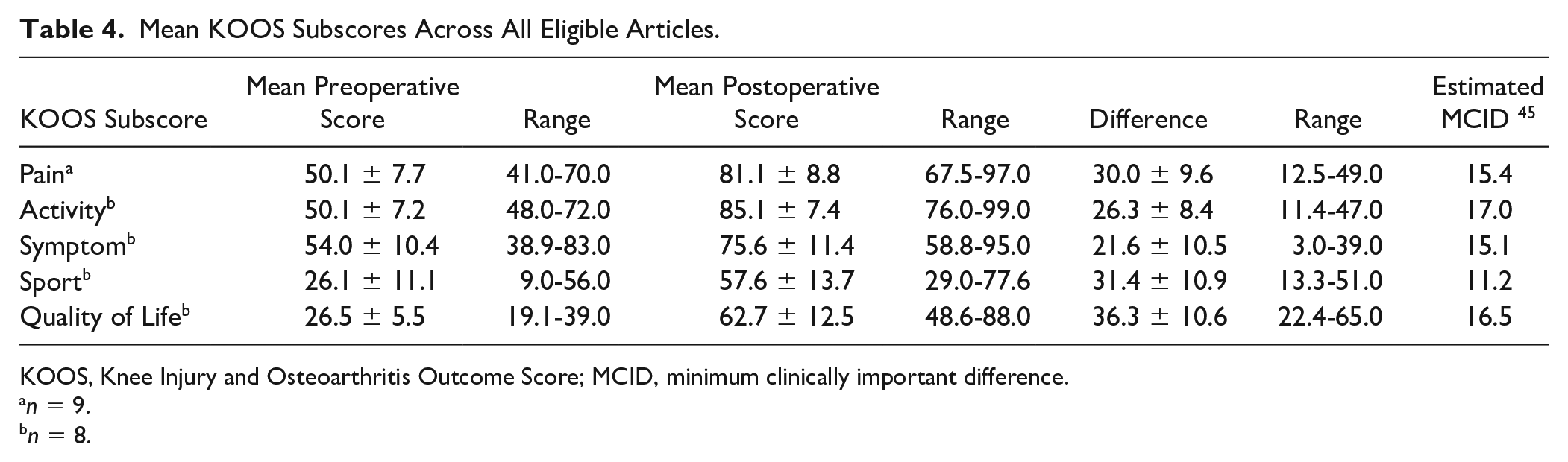
KOOS, Knee Injury and Osteoarthritis Outcome Score; MCID, minimum clinically important difference.
n = 9.
n = 8.
Correlation analyses between postoperative HKA and KOOS Pain scores were calculated using data from 11 studies.9,10,15,19,33,46-52 A moderate correlation was identified at r = 0.35 (Spearman correlation). A moderate correlation was also observed when the differences between pre- and postoperative HKA and KOOS Pain scores were analyzed (r = 0.38, Spearman correlation), suggesting that greater valgised HKA alignments and greater changes in HKA alignment were moderately associated with better KOOS Pain scores.
Data from 3 studies were used to investigate the relationship between postoperative FTA and KOOS Pain. Moderate negative correlations were observed between the postoperative variables and in the differences in both variables over time (both rs = −0.50, Spearman correlations); contradicting the relationship between HKA alignment and KOOS Pain scores.
Birmingham and colleagues reported improvements in the KOOS Pain subscore 5 years following MOWHTO. 9 This sustained improvement was shown to be clinically important when combined with data from other KOOS subscores and knee biomechanics. These findings supported an older study by the same authors, which showed that improvements in KOOS pain scores following MOWHTO were statistically significant. 48 More important, however, the improvements were correlated with reductions in the first peak adduction moment during gait.
Research by Ekeland, McNamara, Mondanelli, Sawaguchi, Sischek, and Van der Woude echoed the above, reporting statistically significant improvements in KOOS Pain score in patients undergoing MOWHTO.33,44,49-52 These improvements were also found to be clinically important and acceptable for a younger population than total knee replacement. However, Ekeland stated that the improvements in KOOS Pain scores plateaued after 1 year. Furthermore, postoperative scores were significantly better in those who presented with OA grades of 1 or 2 than those with OA grades of 3 or 4 preoperatively.
Statistically significant improvements in KOOS Pain scores were also reported in W-Dahl’s patient population, 46 who underwent HTO by the hemicallostasis technique, and by Morin et al. 19 who used surgical navigation to execute their procedures.
Eleven studies reported the remaining subscores. Of these, 9 also reported the HKA angle, and 3 reported the FTA.44,49,51
Strong correlations were observed between postoperative HKA and FTA and Symptom subscores (HKA r = 0.62 and FTA r = 0.50; Spearman correlations), suggesting that greater valgus alignments were associated with better Symptom subscore. However, the correlation between differences in HKA and FTA and Symptom scores were none to moderate (HKA r = 0.39 and FTA r = 0.00; Spearman correlations).
Weak correlations were found between HKA and Activity and Sports subscores (Activity r = 0.24 and Sports r = 0.11; Spearman correlations). However, the differences in HKA and Sports scores were moderately correlated (r = 0.37, Spearman correlation), and the correlation between the differences in HKA alignment and KOOS Activity was strong at r = 0.72 (Spearman correlation). This suggests that greater improvements in Activity and Sports scores may be more dependent on the change in alignment rather than the actual alignment achieved.
A moderate to strong correlation was observed between the Quality of Life subscore and HKA at r = 0.51 (Spearman correlation). The correlation between differences in HKA alignment and Quality of Life was weak, however (r = 0.21, Spearman correlation).
Converse to the results of KOOS subscores and HKA alignment, associations between FTA and Activity, Sports or Quality of Life subscores were negative to a moderate-to-strong degree (r = −0.50 for all 3 subscores; Spearman correlations). This was also true for differences in FTA and Activity, Sports, or Quality of Life subscores (r = −0.50 for all 3 subscores; Spearman correlations). These results suggest that greater valgus alignments are moderately associated with poorer scores in Activity, Sports, and Quality of Life domains, and that greater changes in FTA alignment are associated with smaller changes in these KOOS scores.
Birmingham and colleagues reported statistically significant improvements in all KOOS subscores 2 years following MOWHTO, supporting their hypothesis that the procedure has clinically important implications for patients. 48 Da Cunha, Ekeland, Kanto, McNamara, Morin, Sischek, and Van der Woude et al. also found that average subscores improved significantly postoperatively.10,15,19,33,49,50,52 In Ekeland’s study, the Symptoms, Activity, Sports, and Quality of Life scores were found to improve over 1 year by 54%, 40%, 131%, and 115%, respectively. With improvements in score totaling at least 10 points in each domain, the improvement can be said to be clinically important. These improvements were sustained until final follow-up, at 10 years. According to Kanto et al. 15 improvements in scores beyond 1 year were only significant in the Sports domain; however, the patients in their study were highly active preoperatively.
Sischek investigated the outcome of staged bilateral MOWHTO and found that the KOOS scores of patients who underwent the second procedure within 12 months of the first recovered faster than those who did not get their second procedure within the same year. However, there was not enough evidence to support their hypothesis that the outcome at final follow-up was better in patients who underwent both procedures within 12 months. 52
W-Dahl reported gradual improvements in all KOOS subscores over the course of 2 years following HTO by hemicallostasis. 46 The differences between baseline and final follow-up scores were statistically significant for Quality of Life and Function subscores (P < 0.001). Importantly, the most significant improvements were observed in the early postoperative stage, when the external fixator was still in use. Statistically significant improvements in all KOOS subscores were also found in Mondanelli’s study of MOWHTO with a monoaxial dynamic external fixator. 51
Sawaguchi et al. 44 compared the outcomes of patients who had undergone MOWHTO for osteoarthritis to patients who had opted to continue conservative treatment. Both groups showed significant improvements in all KOOS subscores postoperatively. There were no differences between the groups at final follow-up (2 years), but the group demographics were not comparable.
EQ-5D
Only 2 eligible papers reported the EQ-5D ( Table 3 ). Maffulli and colleagues compared the outcomes of HTO with a xenograph locking plate to HTO with a tricalcium phosphate nonlocking plate. They observed statistically significant improvements in both groups. 53 However, there were no clinically significant differences between fixation types.
Van der Woude et al. 33 reported a preoperative score of 0.64 ± 0.20 in patients who had undergone a HTO. This improved to 0.79 ± 0.30 postoperatively; a difference that was clinically significant at 1 year. 33
After transcribing the data from Maffuli’s study onto a scale of 0.00 to 1.00, the mean preoperative EQ-5D score across both studies was estimated at 0.60 ± 0.06. This improved postoperatively to a mean of 0.76 ± 0.03; a difference of 0.16 ± 0.01.
Discussion
It is commonly stated that satisfaction and good clinical outcomes following HTO are dependent on the alignment achieved postoperatively. A recent review reported that approximately 10% of HTOs failed to achieve a limb alignment, which was within 20% of the intended correction, raising the question whether failure to achieve the target alignment translates into poor patient reported clinical outcome. 7 This systematic review aimed to correlate postoperative joint alignment against 4 PROM scores, to investigate the importance of postoperative knee joint alignment on clinical outcomes.
According to this review, the average postoperative HKA at final follow-up was 2.3° ± 1.7° valgus (range: −1.4° to +6.5°). This is lower than the “ideal correction” of 3° to 6° valgus, suggesting that the ideal valgus alignment is not achieved in the average patient following HTO. This finding corroborates a recent study by Yin et al., 4 whose computational study concluded that MOWHTO using the Fujisawa point led to a postoperative HKA angle of 2.4° valgus. Based on their research, the authors suggested the Fujisawa point should be moved laterally to 71.9% along the tibial plateau if the ideal correction of 4.5° (midpoint of 3°-6°) is to be achieved. 4 However, this may not be necessary for patients to achieve a good clinical outcome.
This systematic review has shown that failure to achieve an average of 3° to 6° valgus following HTO does not negatively affect patient-reported clinical outcome. The studies included in this review consistently reported statistically and clinically important improvements in PROMs postoperatively. This suggested that the ideal correction for good clinical outcome may in fact be more flexible than 3° to 6° valgus, and instead could be closer to 2° to 6° valgus.
When considering the PROMs individually, there was no correlation between postoperative pain reported by VAS and postoperative alignment. This was consistent with previous research by Luites and colleagues, who reported no relationship between clinical outcomes, including the VAS, and postoperative alignment. 13 However, there was a moderate to strong correlation between the differences in pre- and postoperative HKA alignment and VAS suggests that patients whose alignment was altered to a greater extent postoperatively showed greater improvements in pain scores. This relationship was also observed with the KOOS Pain score. These results suggest that the change in alignment may be more important for postoperative pain improvement than the actual achieved alignment. Contrary to these findings however, W-Dahl found no association between the preoperative KOOS Pain score and HKA angle nor between the postoperative change in KOOS Pain Score and HKA angle, suggesting that alignment and pain are discreet variables.46,47 Contradictory findings were also observed in this review when differences in FTA over time were correlated against differences in KOOS Pain scores. A moderate negative relationship between these variables suggested that reductions in pain level were greater when the change in alignment was smaller. However, this calculation included data from only 3 studies.
In this review, the OKS was found to correlate moderately with postoperative alignment. These results suggest that knees that were corrected to a higher degree of valgus, and knees that underwent greatest change in alignment, resulted in better knee pain and function as per the OKS. These finding are supported by research by Bachhal and colleagues, who found positive relationships between the OKS and HKA and the OKS and FTA in patients who underwent HTO by hemicallostasis (Pearson correlations HKA: r = 0.68 and FTA: r = 0.49). 43
Some studies included in this review used the old version of the OKS to report clinical outcome of HTO. The results from these correlation analyses contradicted those of others, by suggesting that joints with greater valgus correction had poorer outcomes. One explanation for this is the small sample size. However, it is also possible that the surgeons operating on these cohorts performed large corrections on their patients, which led to excessive valgus alignments post-operatively. These excessive valgus alignments may have resulted in poorer postoperative scores. This interpretation can be supported by the fact that of the 3 studies that reported the old OKS, one of them reported the greatest mean postoperative valgus FTA of all studies (10.2°), 44 and another reported the greatest changes in alignment in both HKA and FTA across all studies (14.6° and 14.1°, respectively). 43
Symptom KOOS subscores (which cover knee stiffness, swelling, and sensations of grinding, clicking, or giving-way) were the only PROM to strongly correlate with postoperative alignment. However, the correlation between differences in HKA and Symptoms were only moderate, and there was no correlation between the differences in FTA and Symptom score. These results suggested that the actual HKA alignment of the knee, rather than the difference in knee alignment, is more important for postoperative symptom relief.
The postoperative HKA angle did not correlate with Activity and Sports scores. However, the differences in HKA alignment and KOOS Activity and Sports scores were moderate to strong, suggesting that larger changes in knee alignment are associated with greater improvements in activity and sporting ability postoperatively. The opposite relationship was observed when KOOS Quality of Life scores were correlated against HKA, suggesting that the actual alignment achieved postoperatively was more important than the difference in alignment for greater quality of life scores.
However, the correlations between KOOS subscores and FTA produced contradictory findings. Statistical analyses of the FTA against the Activity, Sports, and Quality of Life subscores suggested that higher scores and greater improvements were associated with knees with lesser valgus alignments. This reflected the relationship between the FTA and KOOS Pain score. As previously mentioned, this difference may be attributed to the small sample size for these particular analyses. Thus, caution must be taken when interpreting these results.
This systematic review highlighted the fact that the EQ-5D is rarely utilized to report the outcome of HTO, despite it being recommended as a key PROM by UKKOR and a useful score in assessing health cost utility. As such, it was not possible to determine whether the score correlates with postoperative alignment. However, significant improvements in the score were reported postoperatively in both studies.33,53
Limiting the searches of this review to the PROMs recommended by UKKOR has resulted in the findings of this review being applicable only to patients whose outcomes have been reported by these specific PROMs. Many of the papers excluded from this review reported other PROMs such as the Lysholm, Western Ontario and McMaster University Osteoarthritis Index (WOMAC), Hospital for Special Surgery Knee Score (HSS), and Knee Society Score (KSS). Given the exclusion of these data, this review cannot be used to determine whether all aspects of clinical outcome following HTO correlates with postoperative alignment or not. For example, Altay et al. 24 reported correlations between the change in FTA and the WOMAC and Lysholm scores. Their results suggested that improvements in clinical scores were a result of the realignment. 24 Research by Eduardo Gelber also reported weak negative correlations between preoperative alignment and improvements in Western Ontario Meniscal Evaluation Tool and Kujala PROMs (Pearson correlation r = −0.304 and r = −0.320, respectively). 25 This led the authors to suggest that greater corrections in alignment may be correlated with better clinical outcomes in these 2 PROMs. In this review, we also decided not to report the KOOS as an aggregate score, despite it being reported in 5 articles.10,15,19,33,38 This decision was taken as these scores are not designed to be aggregated, and instead encouraged to be analyzed and interpreted as 5 discreet scores. 54
The diversity of research methods observed in the published research makes it difficult for clinicians and researchers to interpret the findings of this growing body of literature. This field of research would therefore benefit from an agreed standardized set of PROMs to report the clinical outcomes of HTO, as suggested by UKKOR.
In conclusion, while the “ideal alignment” of 3° to 6° valgus was not achieved in the average patient cohort included in this review, the chosen PROM scores improved postoperatively with clinical significance. These findings suggest that the range defined as the “ideal correction” for HTO is more flexible than the often-quoted 3° to 6° valgus. This could have a clinical implication in the way that HTO outcomes are assessed. Nevertheless, it should be borne in mind that the alignment achieved influences more than patient-reported outcomes, and that variables such as survivorship need also to be considered when planning a HTO.
Footnotes
Acknowledgment and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This systematic review used publicly available literature. Consequently, this research did not require institutional ethical approval.