
Abstract
Objective
We sought to determine whether rates of postoperative arthrofibrosis following tibial tuberosity osteotomy (TTO) with complete mobilization of the fragment (TTO-HD) are comparable to TTOs where the hinge remained intact (TTO-HI).
Design
Patients who underwent TTO with concomitant cartilage repair procedure between January 2007 and May 2017, with at least 2 years of follow-up were included in this study. Postoperative reinterventions following TTO-HD and TTO-HI were assessed and multivariant logistic regression models were used to identify whether postoperative reinterventions can be attributed to either technique when controlled for defect size or defect number.
Results
A total of 127 patients (TTO-HD, n = 80; TTO-HI, n = 47) were included in this study. Significantly more patients in the TTO-HD group (31.2%) developed postoperative arthrofibrosis compared with TTO-HI (6.4%; P < 0.05). Multivariant logistic regression revealed that TTO-HD is an independent risk factor for predicting postoperative arthrofibrosis (OR 6.5, CI = 1.7-24.2, P < 0.05).
Conclusion
Patients who underwent TTO with distal hinge detachment and a proximally flipped tubercle for better exposure during concomitant cartilage repair were at a significantly higher risk of postoperative arthrofibrosis than patients with similar size and number of defects treated without mobilization of the tubercle. While certain procedures can benefit from larger exposure, surgeons should be aware of the increased risk of postoperative arthrofibrosis.
Level of Evidence
Level III, case-control study.
Introduction
Tibial tuberosity osteotomy (TTO) is a well-established treatment option for a broad range of patellofemoral joint disorders including patellofemoral instability, patellofemoral chondral lesions and osteoarthritis. 1 The Fulkerson anteromedialization TTO is a popular technique that allows for improvement of patellofemoral tracking and stability, while reducing joint contact forces.2,3 It can be performed in isolation or in conjunction with soft tissue patellar stabilization, biological treatment of chondral disease, or patellofemoral resurfacing.1,4 Chondral lesions of the patellofemoral compartment are common with a reported incidence of 11% and 6% of focal chondral and osteochondral lesions in the patella and trochlea, respectively among patients who underwent knee arthroscopy.5-7 Surgical repair of the chondral defect may become necessary after failure of nonoperative treatment in symptomatic patients. Currently, large full-thickness chondral and osteochondral defects are frequently treated with osteochondral allograft transplantation (OCA) or autologous chondrocyte implantation (ACI) resulting in high patient satisfaction rates and significantly improved functional outcomes.4,8-10 Generally, patellar and trochlear lesions are easily accessible through standard surgical approaches. However, in cases with multiple defects in several compartments, the distal cortical hinge of the tubercle can be detached during TTO (TTO-HD) and the tubercle fragment flipped proximally to facilitate wide exposure of the joint. 11 While this technique is frequently utilized in challenging cases, its safety and complication rates have not been investigated yet.
Arthrofibrosis is a fibrotic joint disorder characterized by excessive collagen production and adhesions that result in restricted joint motion and pain, which often causes significant disability. 12 Although the pathophysiology of joint contracture formation is not well elucidated, previous studies demonstrated that the Hoffa’s fat pad has a significant role in arthrofibrosis development due to its increased secretion of inflammatory cytokines.13-16 In TTO-HD when the tubercle is detached and flipped up, Hoffa’s fat pad is extensively traumatized, potentially increasing the risk of postoperative arthrofibrosis.
The purpose of this study was to determine whether TTO-HD is associated with a higher risk of postoperative arthrofibrosis compared with those TTOs where the hinge remained intact (TTO-HI) and therefore the fat pad was less traumatized. We hypothesized that patients with TTO-HD have a higher risk of developing postoperative arthrofibrosis.
Materials and Method
Patient Population and Inclusion Criteria
Our institutional review board approved this study, and informed consent was obtained from all patients at the time they were entered into our institutional database. In this retrospective review of prospectively collected data, we analyzed data from patients who underwent anteromedialization TTO with concomitant cartilage repair procedure (ACI or OCA) between January 2007 and May 2017 by a single surgeon. Patients with at least 2 years of follow-up and a complete dataset were included in this study. Patients with concomitant meniscus transplantation, anterior or posterior cruciate ligament reconstruction, medial patellofemoral ligament reconstruction, or high tibial/distal femoral osteotomy were excluded from this study. Cartilage repair with ACI or OCA was indicated in patients with one or more full-thickness chondral or osteochondral defects of the knee with symptoms matching the defect location. All patients were evaluated by physical examination, radiography, magnetic resonance imaging (MRI), and diagnostic arthroscopy before cartilage repair was considered. Contraindications for surgical treatment included inflammatory joint disease, unresolved or recent septic arthritis, metabolic or crystal disorders, or deficient soft tissue coverage.
Surgical Technique
Exposure and Osteotomy
TTO-HI procedure
TTO-HI was performed as described previously. 17 Briefly, an incision was made just lateral to the tibial spine, extending approximately 8 cm distal to the tibial tubercle. The musculature of the anterior compartment was mobilized off the lateral tibia in a subperiosteal fashion, extending to the posterior corner of the tibia, without incision of the intermuscular septum. The senior author uses a cutting jig secured to the tibia with 2 pins (Mitek AMZ tracker system) to set the osteotomy angle. The osteotomy was performed with a small oscillating saw leaving the fragment hinged distally. Subsequently, a medial or lateral arthrotomy was performed depending on the location of the cartilage defect(s). On the lateral side, either a standard lateral parapatellar arthrotomy or lateral lengthening approach were performed depending on the tightness of the lateral retinaculum. 18 Following, the defect(s) were prepared and either OCA or ACI was performed as described in detail previously.19-22 The TTO fragment was then rotated anteromedially based on the preoperative plan and secured with two 4.5-mm screws in an anteromedialized fashion. Finally, demineralized bone matrix was placed around the osteotomy site before standard closure.
TTO-HD procedure
A midline incision was made 1 cm proximal to the patella to approximately 8 cm distal to the tibial tubercle. Patella tendon is exposed and a medial parapatellar arthrotomy is performed 0.5 cm from the medial margin of the patella starting from right below the medial patellofemoral ligament (leaving the ligament intact). On the lateral side either lateral parapatellar arthrotomy or lateral lengthening was performed depending on the tightness of the lateral retinaculum.
18
The patellar tendon is dissected free both on the medial and lateral aspect, and the fat pad is dissected off the anterior tibia, just anterior to the intermeniscal ligament. The muscles of the anterior compartment were then bluntly dissected off the bone to the posterolateral corner of the tibia. The simple cutting jig was secured to the proximal tibia with 2 pins to set the osteotomy angle in the aforementioned fashion. The osteotomy was performed with a small oscillating saw and the distal hinge of the tubercle was cut through. Following, the tibial tubercle fragment is flipped proximally to fully expose the knee joint and the articular surface of the patella (
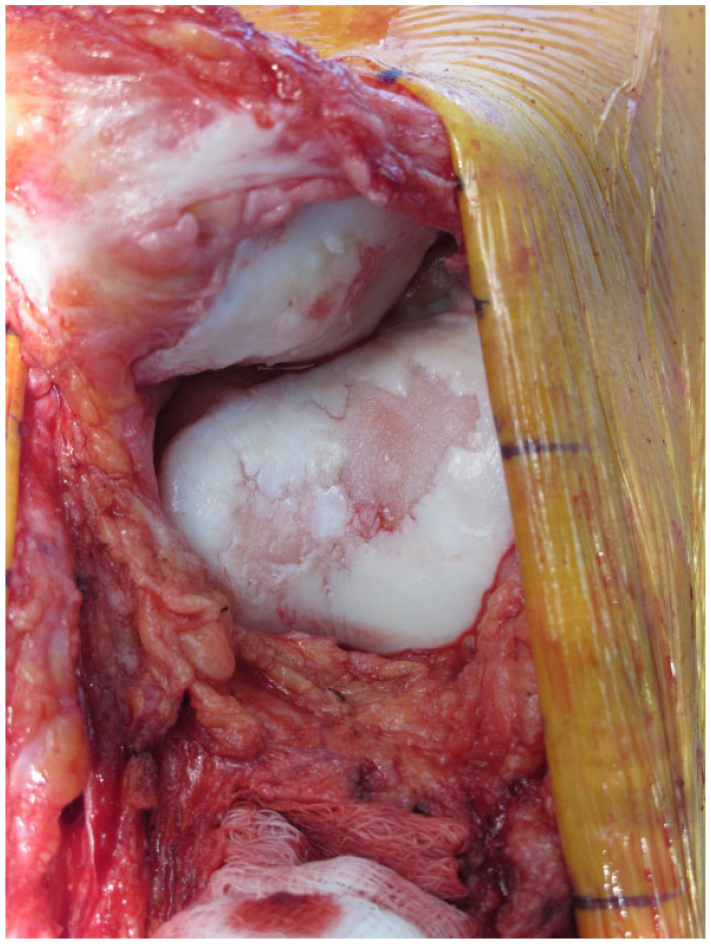
Perioperative image in a patient who underwent tibial tubercle osteotomy with distal hinge detachment and cartilage repair procedure for patella, trochlea, and medial and lateral femoral condyle defects. The image indicates the exposure that the flipped tubercle provided.
Postoperative Rehabilitation
Patients underwent similar postoperative rehabilitation regardless of the procedure. In the first 4 to 6 postoperative weeks, partial weightbearing with knee brace was allowed and then advanced to weightbearing as tolerated. During this period, patients were permitted to begin unrestricted range of motion exercises, quadriceps sets, straight-leg raises, and patellar mobilization. Continuous passive motion was also used for 3 to 6 weeks. Patients were allowed to return to most activities of daily living at 3 months; return to nonimpact functional activities, including biking, and treadmill walking; progression to an elliptical trainer was allowed after 4 to 6 months. After 12 months, patients’ activities were progressed to in-line jogging. Full activities were allowed at 18 months if a physical examination demonstrated return of full motion and muscle tone, no effusion, and complete isotonic graft appearance with a lack of bone marrow edema on MRI. 23
Postoperative Reinterventions
Patients were considered to have developed postoperative arthrofibrosis if postoperative knee flexion was <75° and/or lack of extension was 15° or greater; and the patients underwent surgical intervention due to knee stiffness.24,25 All patients underwent arthroscopic lysis of adhesions; blind manipulation under anesthesia was not performed due to the risk of inadvertent damage to the graft. Besides arthrofibrosis, other postoperative reinterventions were also evaluated such as chondroplasty, debridement, meniscus surgery (meniscectomy, meniscal repair, and meniscal allograft transplantation), and graft failure.26-28 Graft failure was defined as a surgical removal of more than 25% of the graft area; revision cartilage repair of the treated defect, or prosthetic replacement. 29
Statistical Analysis
SPSS (version 21.0; IBM Corp.) was used for statistical analysis. Continuous variables are reported as mean ± standard deviation, whereas categorical variables are reported as numbers and percentages. Normal distribution of the data was confirmed using the Shapiro-Wilk test. Continuous data were compared with the independent-samples t test. Categorical data was compared with the chi-square test or the Fisher’s exact test, as appropriate. To identify whether reinterventions can be attributed to TTO-HD a multivariant logistic regression models were used controlling for defect size and defect number. The results of the multivariant logistic regression analyses are presented as odds ratios (ORs) with accompanying 95% confidence intervals (CIs). Results were considered to be statistically significant when the null value (1.00) was absent from the CI or P < 0.05.
Results
A total of 144 patients underwent cartilage repair with concomitant TTO between January 2007 and June 2017. Of these, 4 patients (2.8%) were excluded from this study due to incomplete data and 13 patients (9%) were lost during the follow-up period. Therefore, 127 (88.2%) met the inclusion criteria. Of these, 95 underwent TTO-HD (59%) and 66 TTO-HI (41%). The mean age at the time of surgery was 32.6 ± 9.5 years with a mean follow-up of 4.6 ± 2.6 years. Baseline demographic and clinical patient characteristics are reported in Table 1 . In the TTO-HD group, significantly larger cartilage defects were repaired (TTO-HD 8.8 ± 5 cm2 vs. TTO-HI 4.9 ± 2.4 cm2; P < 0.05) with greater number of defects (TTO-HD 2 ± 0.9 vs. TTO-HI 1.5 ± 0.7; P < 0.05) compared with the TTO-HI group ( Table 1 ).
Demographic Data of Patients Who Underwent Anteromedialization TTO.
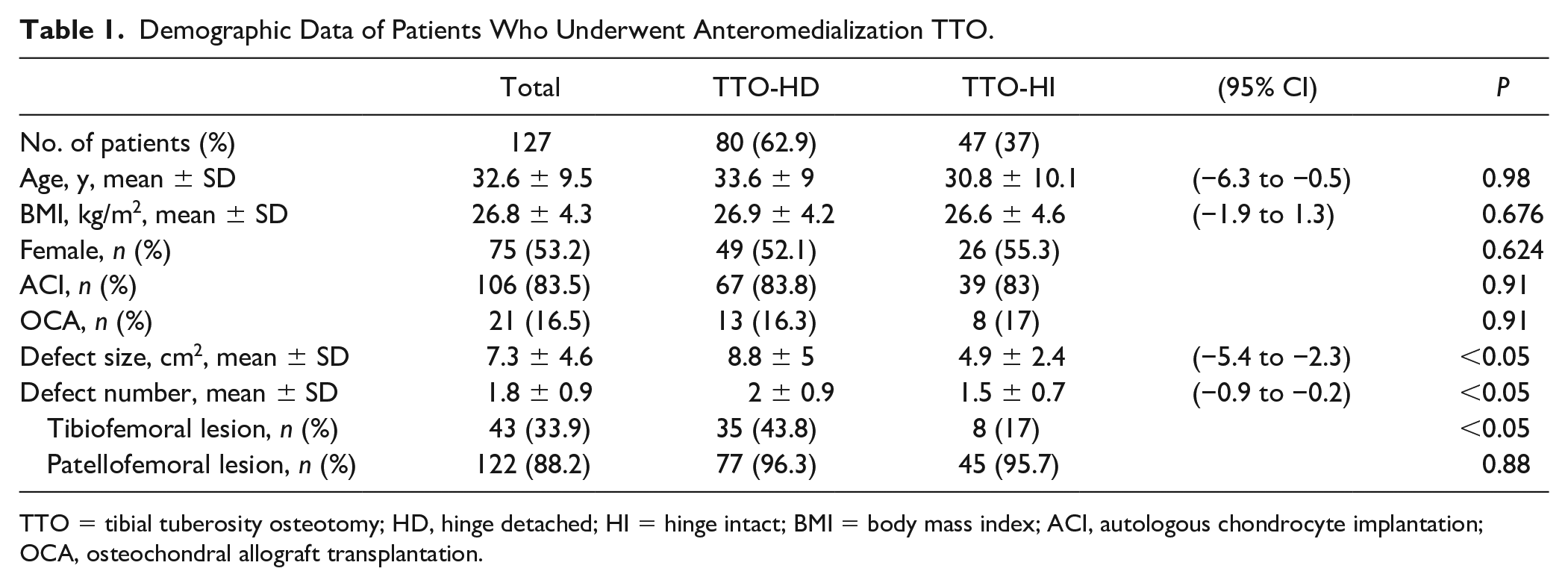
TTO = tibial tuberosity osteotomy; HD, hinge detached; HI = hinge intact; BMI = body mass index; ACI, autologous chondrocyte implantation; OCA, osteochondral allograft transplantation.
Subsequent Surgery
Significantly more patients presented with subsequent surgery following TTO-HD than TTO-HI (TTO-HD n = 45, 60% vs. TTO-HI n = 16, 34%; P < 0.05) ( Table 2 ). Among those patients who underwent TTO-HD significantly more patients developed postoperative arthrofibrosis (TTO-HD n = 25, 31.2% vs. TTO-HI n = 3, 6.4%; P < 0.05) compared with the TTO-HI group. The prevalence of other subsequent procedures was similar between both groups ( Table 2 ). Multivariant logistic regression models were used to identify whether these procedures can be attributed to TTO-HD when controlled for defect size and defect number. Multivariant logistic regression revealed TTO-HD as an independent risk factor for predicting postoperative arthrofibrosis (OR 6.5, CI 1.7 to 24.2, P < 0.05) ( Table 3 ).
Reasons for Subsequent Surgery.
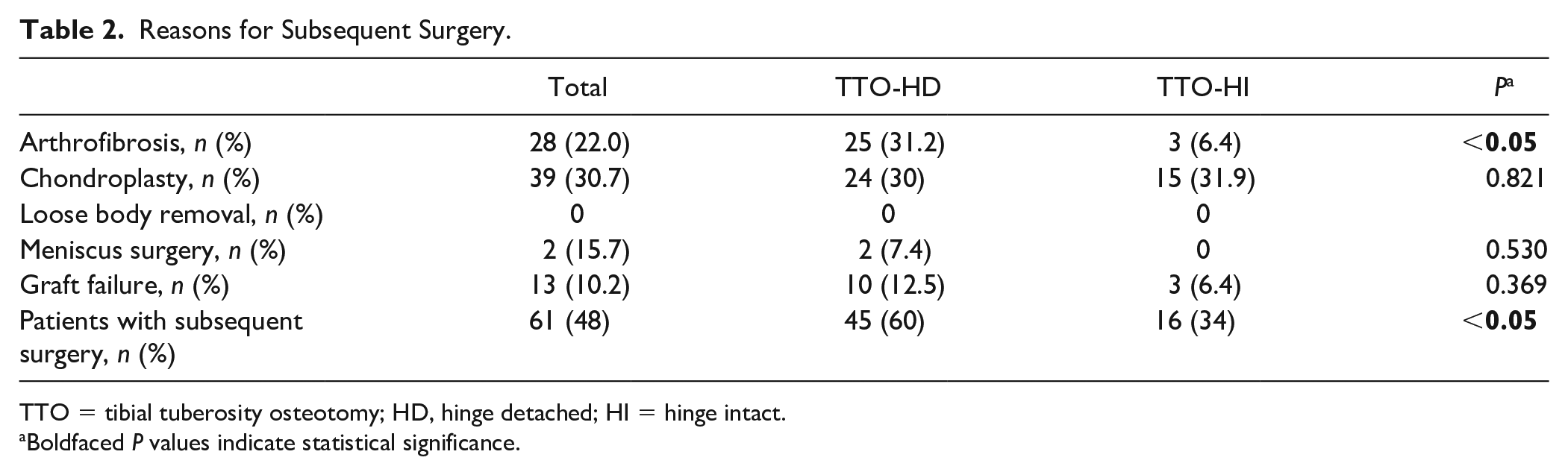
TTO = tibial tuberosity osteotomy; HD, hinge detached; HI = hinge intact.
Boldfaced P values indicate statistical significance.
Multivariant Logistic Regression for Predicting Arthrofibrosis Following TTO with Concomitant Cartilage Repair Procedure.
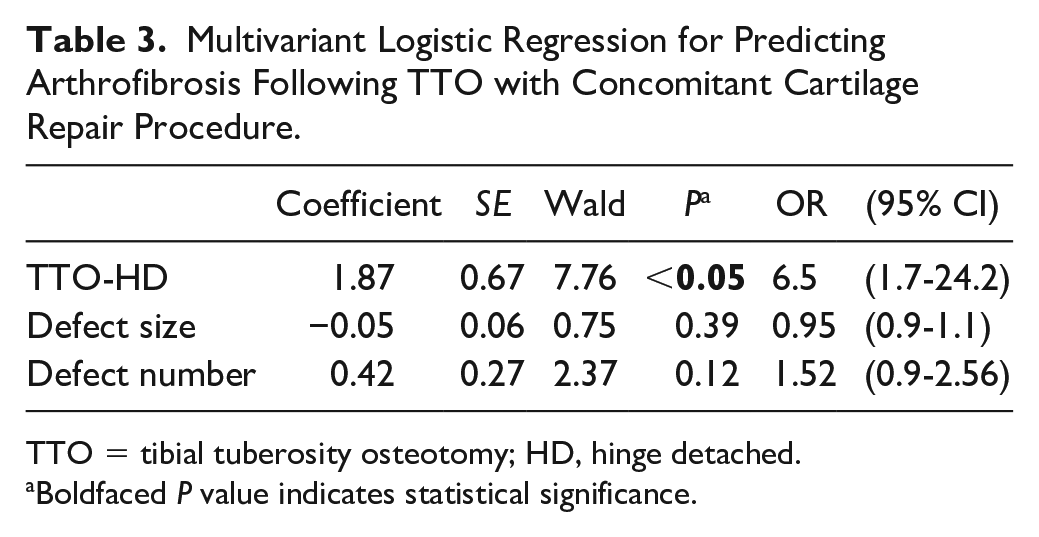
TTO = tibial tuberosity osteotomy; HD, hinge detached.
Boldfaced P value indicates statistical significance.
Discussion
The key finding of this study is that TTO-HD is a significant independent risk factor for predicting postoperative arthrofibrosis (P < 0.05). Patients with tubercle mobilization for exposure were almost 6.5 times more likely to develop postoperative arthrofibrosis than patients where the tubercle was not mobilized proximally.
TTO is a common surgical procedure to treat patients with patellar instability and/or patellofemoral chondrosis.1,4 A variety of TTO techniques (i.e., Elmslie-Trillat, Maquet, Fulkerson) have been described with good to excellent outcomes ranging from 66% to 96%.1,4,30,31 The most frequently used TTO technique in current clinical practice is the Fulkerson anteromedialization osteotomy.
Arthrofibrosis is a rare but potentially devastating complication after cartilage repair surgery with a reported incidence of 5% to 22%.32-36 Prognostic factors leading to the development of arthrofibrosis are not completely understood but may include previous injuries (anterior cruciate ligament), decreased preoperative range of motion, poor surgical technique, early-onset osteoarthritis, or inadequate postoperative rehabilitation. 37 Arthrofibrosis can be noninflammatory or inflammatory. In most of noninflammatory arthrofibrosis, congenitally impaired connective tissue development is responsible for joint contracture, while inflammatory joint contractures are more common in posttraumatic conditions followed by prolonged joint immobilization. 25 In inflammatory arthrofibrosis there is an imbalance in chemical mediators that regulate the normal resolution of inflammation and the fibroblastic proliferative phase of healing. 38 This inflammation stimulates the proliferation of activated cells resulting in the production of extracellular matrix macromolecules that form fibrotic tissue that is deposited into the capsule, with a joint contracture as the final outcome. 39
In patients with symptomatic cartilage lesions the process of early osteoarthritis (OA) has already initiated.40-42 Early OA is a risk factor for developing arthrofibrosis after injury or surgery. In this condition, a proinflammatory and profibrosis environment exists due to the elevated interleukin-6 (IL-6), and tumor necrosis factor-α (TNF-α) levels within the joint. TGF-β, a well-known initiator of fibrosis is also increased in OA patients’ subchondral bone and synovial cells.12,40-44 Consequently, we believe that patients who undergo cartilage repair procedures, especially those with large lesions, are already at risk to develop postoperative adhesions. We found that patients who underwent TTO-HD had a 6.5 odds ratio to develop postoperative arthrofibrosis requiring surgical intervention than patients with less extensive manipulation of the tubercle fragment and therefore fat pad. The bursae around the knee joint, especially the Hoffa’s fat pad, store and produce inflammatory cytokines, macrophages, T cells, B cells, and mast cells that can be locally activated by an insult to secrete inflammatory cytokines, particularly TNF-α and IL-6.13-15 Previous studies have shown that these activated macrophages can be detected even 20 weeks after surgery and play a key role in arthrofibrosis development.13,16 Moreover, activated by joint inflammation, adipose cells within the Hoffa’s fat pad can transform into fibrosus tissue leading to abnormal functioning of the Hoffa’s fat pad, ultimately resulting in joint stiffness and pain. 13 During TTO-HD, the fat pad is dissected off the patella tendon and proximal tibia before flipping the tubercle proximally, and more exposed to room air allowing it to dry out more than when the tubercle is not flipped. We believe that this trauma to the fat pad and greater traction on the patella tendon induce an inflammatory response that may contribute to the increased risk of postoperative stiffness after TTO-HD seen in the current study.
In general, tubercle mobilization is rarely necessary for isolated patellofemoral resurfacing. Larger exposure results in more postoperative complications and therefore opening the joint should be avoided whenever it is possible. 45 However, adequate exposure is of utmost importance for successful surgery and this procedure can be useful when visualization and access are challenging. Yet the treating surgeon should be aware of the potential for reinterventions, indicate tubercle mobilization only judiciously, and carefully monitor patients postoperatively for signs of motion restrictions.
Limitations
In our study, patients were not randomized to tubercle detachment versus hinge preservation, but this was rather based on the necessary exposure. However, the procedures were performed by the same surgeon in the same technique besides the step of the tubercle detachment and fat pad transection. In addition, this study included patients with different concomitant cartilage repair procedures (ACI or OCA) with TTO, although the number and distribution of these procedures was similar between both TTO groups ( Table 1 ) with similar arthrofibrosis rates following ACI (n = 27, 22.5%) and OCA (n = 6, 28.6%) (P = 0.554). Finally, postoperative arthrofibrosis was only used as a dichotomous variable (yes/no) depending on whether the patient required surgical intervention due to knee stiffness, which may underestimate rate of arthrofibrosis in those where reintervention is not performed.
Conclusion
Patients who underwent TTO with distal hinge detachment and a proximally flipped tubercle for wide exposure were at a significantly higher risk of postoperative arthrofibrosis than patients with similar size and number of defects treated without mobilization of the tubercle. Certain procedures may require better exposure and therefore the utilization of TTO-HD. However, treating surgeon should be aware of the increased risk of postoperative arthrofibrosis.
Footnotes
Authors’ Note
Investigation performed at the Cartilage Repair Center, Brigham and Women’s Hospital, Harvard Medical School, Boston, MA, USA
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Institutional review board approval (No. 2019P000430) was obtained for the prospective registry used in this study.
Informed Consent
Informed consent was obtained from all patients at the time they were entered into our institutional database.
Trial Registration
Not applicable