
Abstract
Objective
To identify joint structural risk factors, measured using quantitative compositional and semiquantitative magnetic resonance imaging (MRI) scoring, associated with the development of accelerated knee osteoarthritis (AKOA) compared with a more normal rate of knee osteoarthritis (OA) development.
Design
From the Osteoarthritis Initiative we selected knees with no radiographic OA (Kellgren-Lawrence grade [KL] 0/1) that developed advanced-stage OA (KL 3/4; AKOA) within a 4-year timeframe and a comparison group with a more normal rate of OA development (KL 0/1 to KL 2 in 4 years). MRIs at the beginning of the 4-year timeframe were assessed for cartilage T2 values and structural abnormalities using a modified Whole-Organ Magnetic Resonance Imaging Score (WORMS). Associations of MRI findings with AKOA versus normal OA were assessed using multivariable logistic regression models.
Results
A total of 106 AKOA and 168 subjects with normal OA development were included. Mean cartilage T2 values were not significantly associated with AKOA (odds ratio [OR] 1.06; 95% confidence interval [CI] 0.82-1.36). Risk factors for AKOA development included higher meniscus maximum scores (OR 1.37; 95% CI 1.11-1.68), presence of meniscal extrusion (OR 6.30; 95% CI 2.57-15.49), presence of root tears (OR 4.64; 95% CI 1.61-13.34), and higher medial tibia cartilage lesion scores (OR 1.96; 95% CI 1.19-3.24).
Conclusions
We identified meniscal damage, especially meniscal extrusion and meniscal root tears as risk factors for AKOA development. These findings contribute to identifying subjects at risk of AKOA at an early stage when preventative measures targeting modifiable risk factors such as meniscal repair surgery could still be effective.
Keywords
Introduction
Knee osteoarthritis (OA) is the most common degenerative disorder of the knee and ranked as the one of the leading causes of global disability. 1 The disease is caused by a range of mechanical and biochemical disorders, collectively leading to structural and functional joint failure.2,3 While disease progression typically occurs gradually, over the course of many years, 4 accelerated knee osteoarthritis (AKOA) is a form of knee OA characterized by rapid OA onset and progression of structural damage, leading to severe to end-stage disease within 4 years or less. 5 AKOA has been described to occur in 3.4% of adults at risk of knee OA and is linked to significant pain and functional limitations.5,6 Clinical risk factors associated with AKOA have been studied previously. Driban et al.7-9 identified higher age, recent knee injury, greater coronal tibial slope, and elevated body mass index (BMI) in subjects younger than 63.5 years as risk factors for AKOA. However, identifying subjects at risk of AKOA remains challenging given that most clinical risk factors are also well-established risk factors for knee OA in general. 10 .
Imaging features frequently observed in knees developing AKOA include meniscal tears such as root and radial tears, meniscal extrusion, and subchondral insufficiency fractures.11-13 Moreover, meniscal tears and specifically medial meniscal root tears were frequently reported in knees developing spontaneous osteonecrosis. 14 Though several studies evaluated MR (magnetic resonance) risk factors for OA development in early structural disease,15-17 there appear to be no studies comparing differences in joint structural factors, between subjects at risk of AKOA, and those at with a more normal rate of OA development. Moreover, biochemical cartilage composition has not been assessed in subjects with AKOA. Water content and collagen architecture can be characterized with T2 relaxation time measurements, which has been shown to be a risk factor for incident knee OA18-22; however, it is unclear if it is also a risk factor for AKOA. Given the rapid pace of cartilage loss and limited opportunity to intervene, this knowledge may contribute to identifying subjects at risk of AKOA and initiate preventative measures.
The primary goal of this study was to assess the association of knee cartilage composition and joint morphological features in knees without radiographic OA, with subsequent development of AKOA compared with a more normal rate of OA development within a 4-year time frame. In addition, we describe differences of demographic and clinical characteristics of subjects with AKOA and a normal rate of OA development.
Methods
Subjects
We conducted a nested case-control study within the Osteoarthritis Initiative (OAI, http://www.oai.ucsf.edu). The OAI is a prospective, longitudinal, multicenter, observational cohort study enrolling 4,796 subjects with or at risk for symptomatic knee OA. Informed consent was obtained from all participants; the study was compliant with the Health Insurance Portability and Accountability Act and approved by the local institutional review boards of all participating centers. Participants were recruited from February 2004 until May 2006.
We used Kellgren-Lawrence (KL) grades, from the OAI baseline visit, 24, 48, 72, and 96 months to identify subjects with accelerated knee OA development (KL 0/1 to KL 3/4, AKOA group) and normal OA development (KL 0/1 to KL 2) within a 4-year period (normal OA group) at any time point within the observation period of the OAI. The starting time point of this 4-year time frame for those with AKOA and normal OA was defined as the index visit. The subject selection process is shown in Figure 1 .
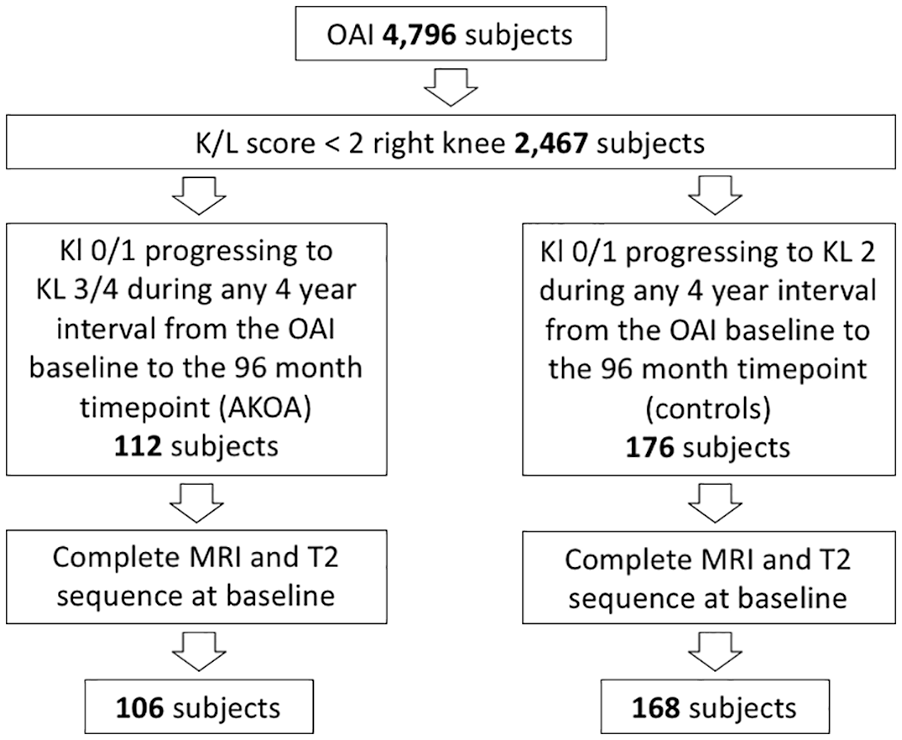
Subject selection flowchart.
Subject characteristics were assessed at the index time point. Assessed characteristics included age, sex, race, BMI, Physical Activity Score of the Elderly (PASE), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) pain and stiffness scores, presence of medial or lateral joint line tenderness and presence of knee effusion (bulge and patellar tap sign), and Knee Injury and Osteoarthritis Outcome Score (KOOS) pain scores for twisting/pivoting the knee, straightening or bending the knee fully. We also analyzed self-reported knee injuries limiting subjects’ ability to walk for at least two days and knee surgery.
Magnetic Resonance Imaging
MRIs were acquired on 4 identical 3-T scanners (Siemens Magnetom Trio; Siemens, Erlangen, Germany) using standard transmit-receive knee coils (USA Instruments, Aurora, OH, USA). A sagittal 2-dimensional (2D) multi-slice-multi-echo spin-echo sequence with 7 echo times (10 ms, 20 ms, 30 ms, 40 ms, 50 ms, 60 ms, 70 ms; repetition time = 2700 ms; slice thickness = 3 mm) was used to obtain cartilage T2 relaxation measurements. Sagittal 2D intermediate-weighted fat-suppressed turbo spin-echo sequences (repetition time, 3200 ms; echo time, 30 ms; slice thickness, 3 mm), coronal 2D intermediate-weighted non-fat-suppressed turbo spin-echo sequences (repetition time, 3700 ms; echo time, 29 ms; slice thickness, 3 mm) and sagittal 3D dual-echo in steady state with selective water excitation (repetition time, 16.3 ms; echo time, 4.7 ms; slice thickness, 0.7 mm) were used for the analysis of morphological/structural abnormalities. The acquisition protocol has been published previously. 23
MR Image Analysis
T2 relaxation times were measured at the index visit using an in-house, spline-based algorithm written in MatLab (MathWorks, Natick, MA, USA) for semiautomatic segmentation as described previously. 24 Compartments segmented included the patella, the medial and lateral femur and tibia. The trochlea was not segmented due to flow-artifacts in this region caused by the popliteal artery. T2 values were calculated for each compartment by using a monoexponential decay model as fitting function for the signal intensity using six echoes (echo times 20-70 ms) after excluding the first echo to reduce potential errors resulting from stimulated echoes and using 3 parameter fittings accounting for noise.25,26 A global T2 value was derived using the mean of all compartments.
All index visit images were individually and independently read by 2 radiologists (S.C.F. and Y.L., each with 4 years of experience), blinded to clinical data and group (AKOA or controls), using the modified semiquantitative WORMS score of the knee. 27 In case of disagreement, a consensus reading was performed with a third board-certified musculoskeletal radiologist (T.M.L., 25 years of experience). Morphological abnormalities graded included cartilage lesions and bone marrow edema pattern (BMEP) each graded over 6 subregions (patella, trochlea, medial and lateral femur and tibia) and meniscal abnormalities (3 medial and 3 lateral graded subregions: meniscus body, anterior horn and posterior horn). Maximum scores across all subregions were calculated for each WORMS category. In addition, meniscal tears were graded as vertical, horizontal, flap, complex, bucket handle, or root tears and presence or absence of meniscal extrusion was documented with a cutoff of 3 mm/2 mm for the medial and lateral meniscus, respectively.28,29
Inter-/Intrareader Reproducibility
Intra- and interreader reproducibility of WORMS grading by our group have been validated in multiple previous studies.18,30-33 In these studies, intraclass correlation coefficients were calculated in order to compare WORMS subscores for the meniscus and cartilage. Intraclass correlation coefficients for intrareader reproducibility ranged between 0.80 (0.69-0.95) 32 and 0.96 (0.94-0.97) 31 for the meniscus and between 0.81 (0.68-0.91) 32 and 0.99 (0.98-0.99) 31 for the cartilage. Interreader intraclass correlation coefficients ranged between 0.81 (0.76-0.88) 32 and 0.97 (0.95-0.98) 31 for the meniscus and between 0.79 (0.72-0.868) 33 and 0.97 (0.95-0.98) 31 for the cartilage.
Statistical Analysis
The statistical analysis was performed with Stata v. 14 software (StataCorp, College Station, TX, USA) using a 2-sided 0.05 level of significance. Differences in characteristics between the AKOA and normal OA groups were assessed at the index time point (beginning of the 4-year time frame) using Pearson’s chi-square tests for categorical data (gender, race distribution, risk factors for knee OA) and t tests for numeric variables (age, BMI, PASE, WOMAC). Logistic regression models were used to assess whether cartilage T2 and WORMS were associated with the development of AKOA, adjusting for age, sex, BMI, and race. Standardized T2 values were calculated by subtracting the mean from the variable and dividing it by the standard deviation.
Results
Subject Demographics and Clinical Correlates of AKOA
The final study population selected from the OAI consisted of 106 subjects with AKOA (KL 0/1 to KL3/4 within a 4-year period) and 168 with normal OA (KL 0/1 to KL 2 within a 4-year period). The starting timepoint of the 4-year time frame was defined as the index visit. Subject characteristics are presented in Table 1 .
Subject Characteristics.
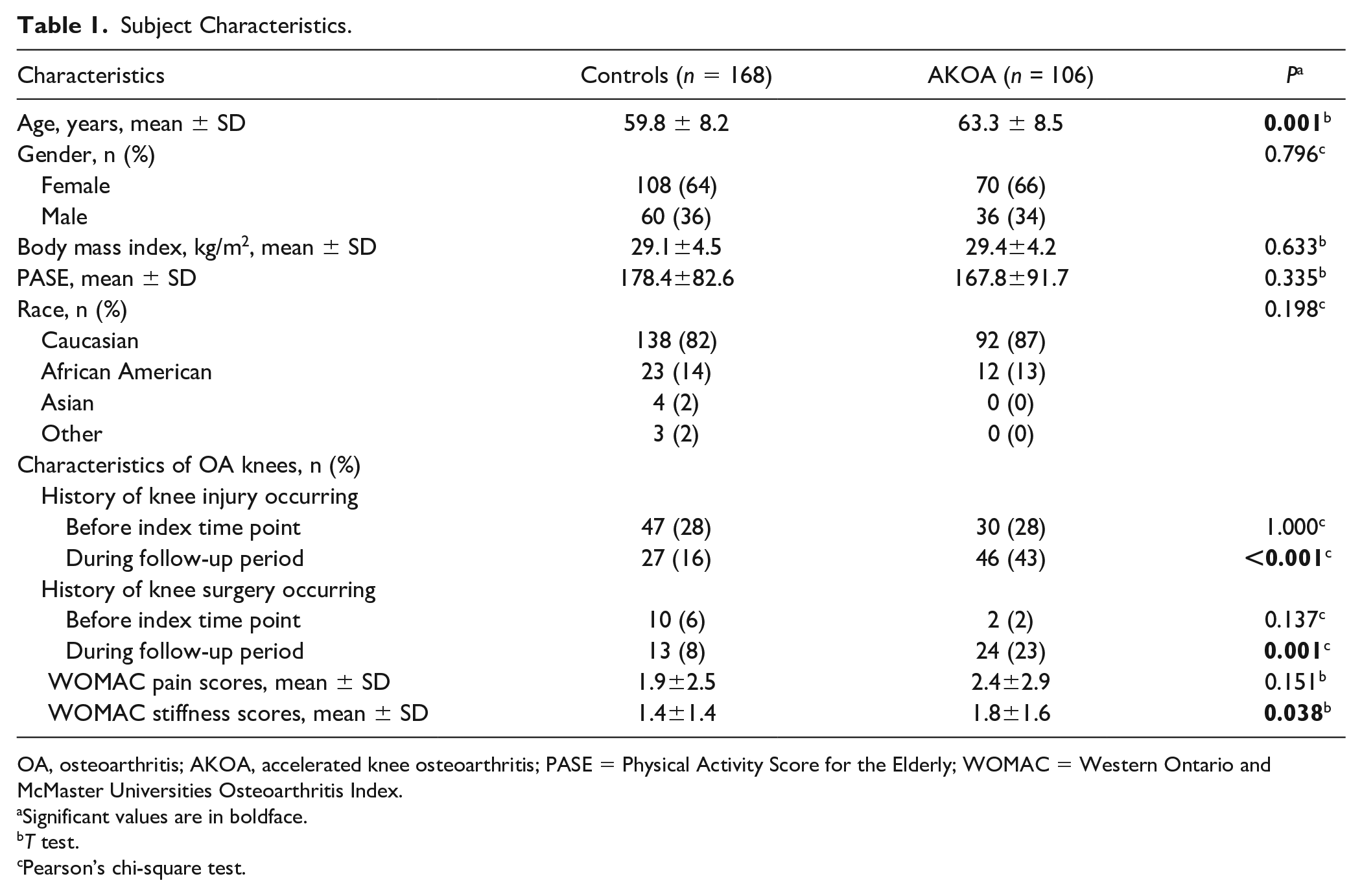
OA, osteoarthritis; AKOA, accelerated knee osteoarthritis; PASE = Physical Activity Score for the Elderly; WOMAC = Western Ontario and McMaster Universities Osteoarthritis Index.
Significant values are in boldface.
T test.
Pearson’s chi-square test.
The mean age of subjects in this study was 61.1 ± 8.5 years, with a mean BMI of 29.2 ± 4.4 kg/m2 and more females (65%) than males. In comparison to normal OA, the AKOA group was older (63.3 ± 8.5 vs. 59.8 ± 8.2 years; P = 0.001), while the mean BMI (29.5 ± 4.3 vs. 29.3 ± 4.6 kg/m2; P = 0.663) and PASE (167.8 ± 91 vs. 178.4 ± 83; P = 0.335) were similar in both groups. Moreover, both groups had a similar distribution for sex and race.
Incident knee injury or surgery during the four years following the index visit were more frequent in the AKOA group (knee injury: 43% vs. 16%; P < 0.001; knee surgery: 23% vs. 8%; P = 0.001). History of knee injury or surgery before the index visit was not significantly more often present in the AKOA group or the control group (P > 0.137). During the 4 years following the index visit, all surgery types reported were arthroscopic partial meniscectomy surgeries. The surgery types reported before the index visit included n = 2 arthroscopic partial meniscectomy surgeries for the AKOA group; and n = 7 arthroscopic partial meniscectomy surgeries, n = 1 ligament repair surgery, and n = 2 prior arthroscopies for the normal OA group.
We also found differences between both groups comparing clinical symptoms at the index visit: WOMAC knee stiffness scores were significantly higher in the AKOA group, while differences in overall WOMAC pain scores were not significant (P = 0.151). Severe-extreme knee pain when fully bending the knee at the index visit was more often present in the AKOA group (9%, 9/106 vs. 2%, 3/168; P = 0.013). No significant differences were found for pain scores for twisting/pivoting the knee or straightening the knee fully (P > 0.05).
Morphological Knee Abnormalities
Results for WORMS features assessed at the index visit for each group are summarized in Tables 2 and 3 . Meniscal damage was the morphological feature most consistently associated with AKOA development compared with normal OA development. The majority of WORMS meniscus features showed significantly higher scores at the index visit in subjects later developing AKOA. Specifically, knees with higher maximum scores of the medial and lateral meniscus (adjusted odds ratio [OR] per 1 unit increase, 1.37; 95% confidence interval [CI] 1.11-1.68; P = 0.003), higher scores of the medial and lateral meniscus body (adjusted OR per 1 unit increase, 1.37; 95% CI 1.08-1.75; P = 0.010 and adjusted OR per 1 unit increase, 1.42; 95% CI 1.08-1.87; P = 0.011, respectively) and higher scores of the lateral posterior horn (adjusted OR per 1 unit increase, 1.50; 95% CI 1.10-2.05; P = 0.010) were at higher odds of developing AKOA ( Fig. 2 ).
Magnetic Resonance Imaging Features. a
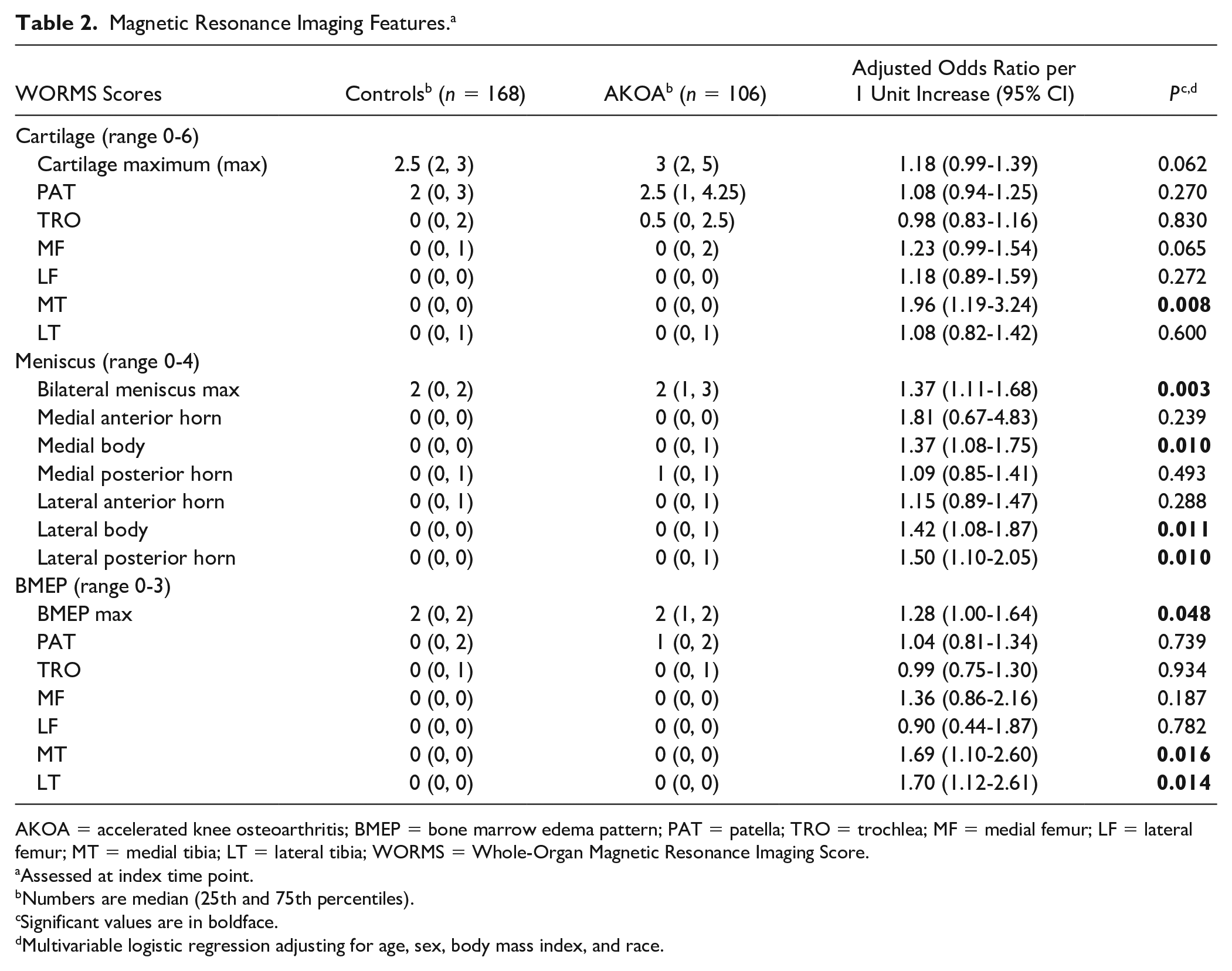
AKOA = accelerated knee osteoarthritis; BMEP = bone marrow edema pattern; PAT = patella; TRO = trochlea; MF = medial femur; LF = lateral femur; MT = medial tibia; LT = lateral tibia; WORMS = Whole-Organ Magnetic Resonance Imaging Score.
Assessed at index time point.
Numbers are median (25th and 75th percentiles).
Significant values are in boldface.
Multivariable logistic regression adjusting for age, sex, body mass index, and race.
Meniscal Abnormalities. a
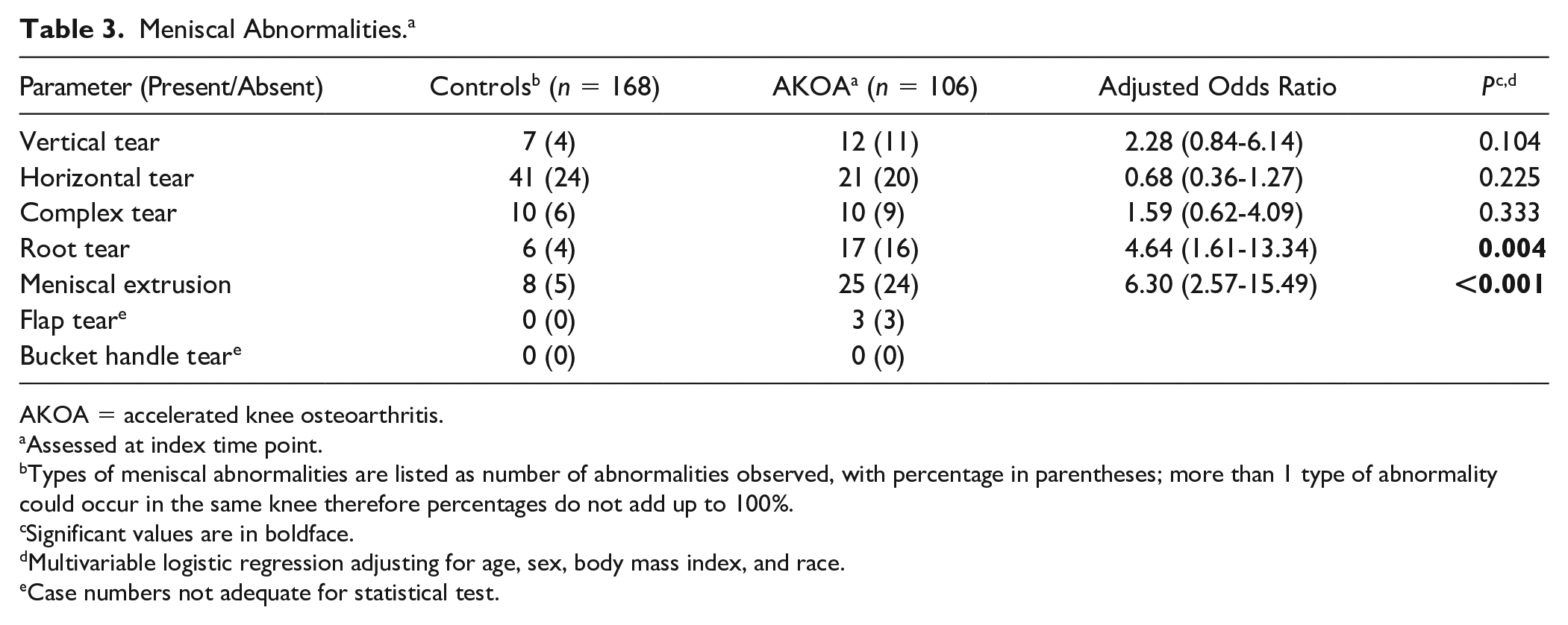
AKOA = accelerated knee osteoarthritis.
Assessed at index time point.
Types of meniscal abnormalities are listed as number of abnormalities observed, with percentage in parentheses; more than 1 type of abnormality could occur in the same knee therefore percentages do not add up to 100%.
Significant values are in boldface.
Multivariable logistic regression adjusting for age, sex, body mass index, and race.
Case numbers not adequate for statistical test.
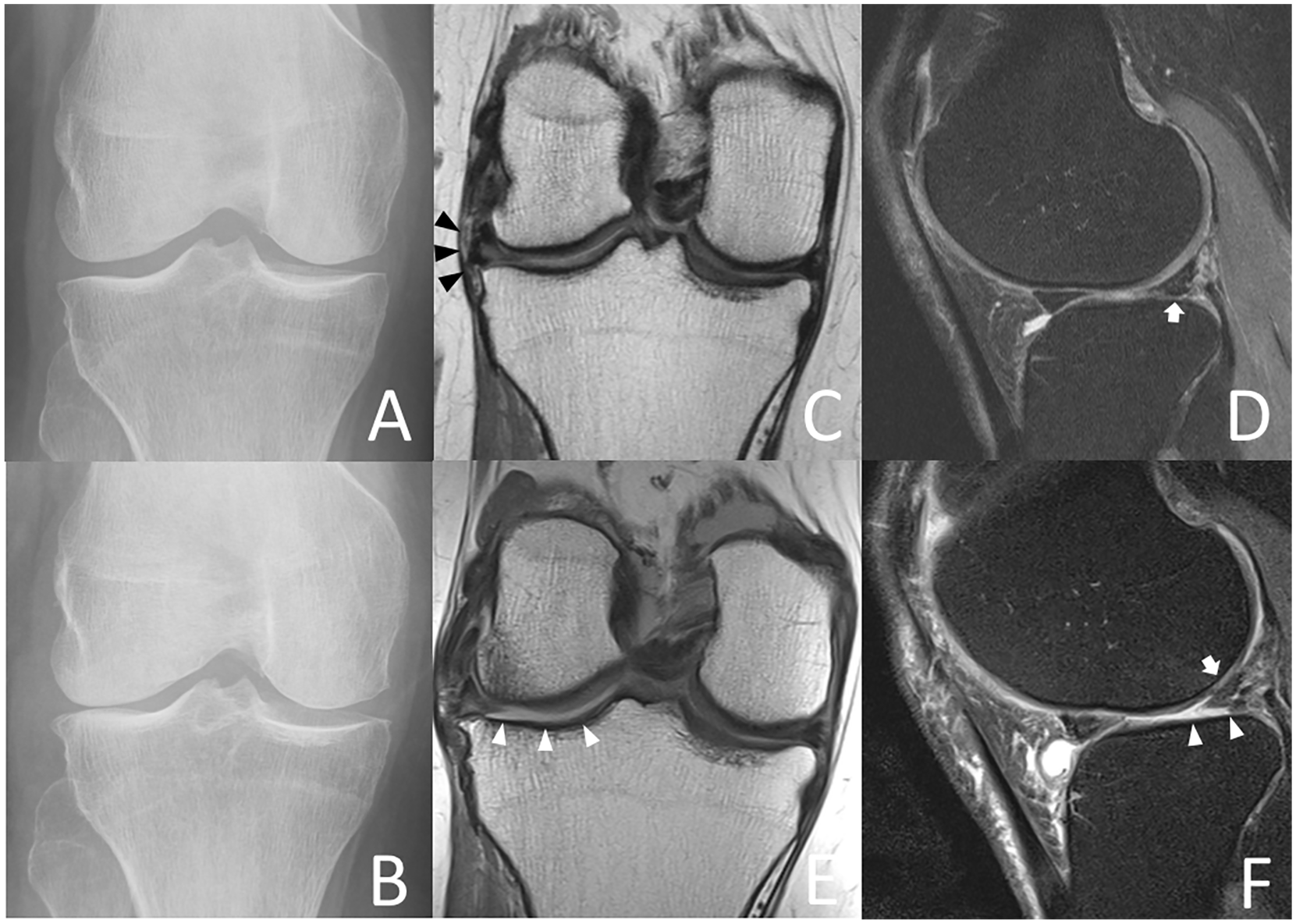
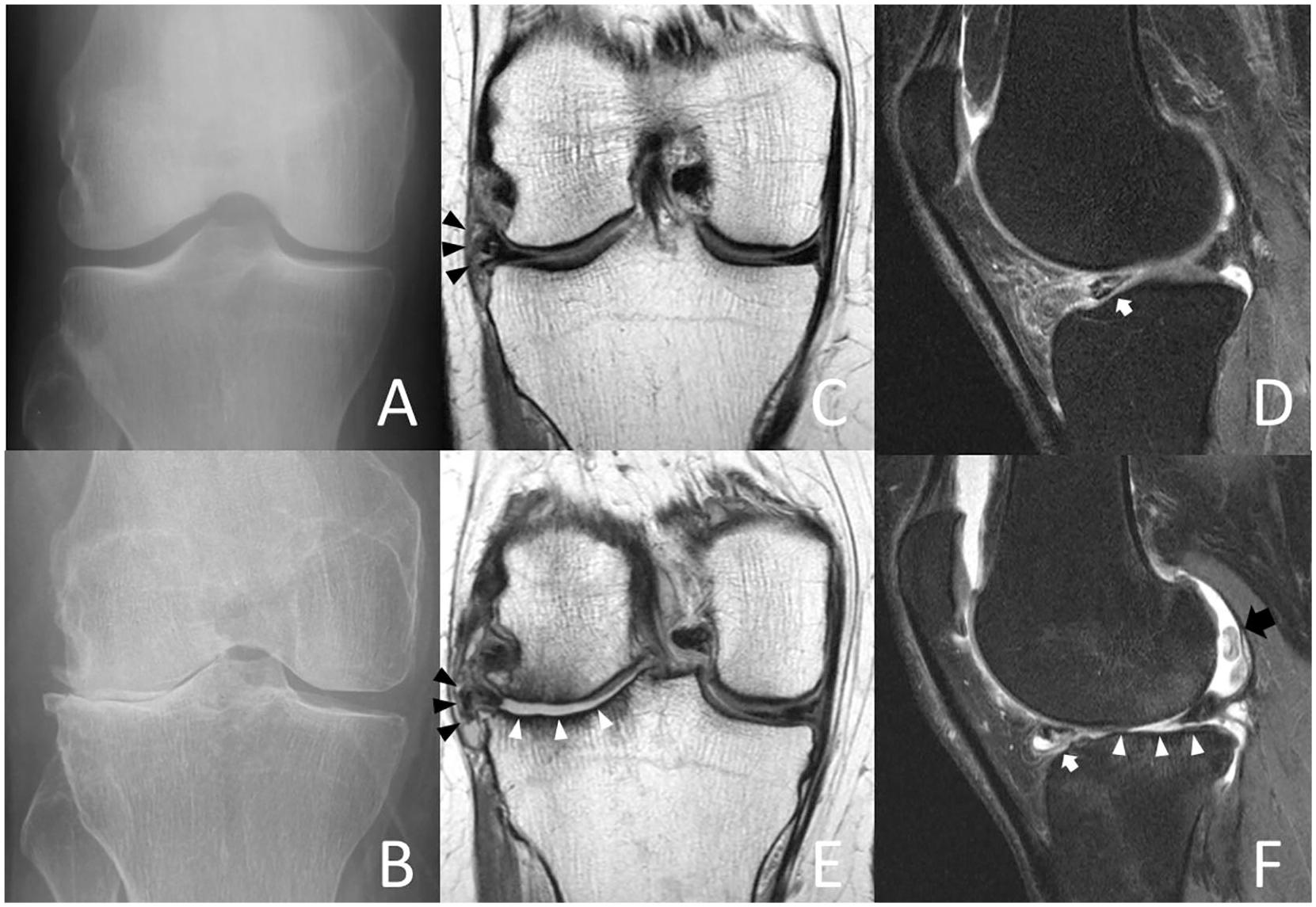
Index visit (
Regarding types of meniscal damage associated with AKOA development, knees with meniscal root tears (adjusted OR 4.64; 95% CI 1.61-13.34; P = 0.004) and medial or lateral meniscal extrusion (adjusted OR 6.30; 95% CI 2.57-15.49; P < 0.001) at the index visit were at higher odds for AKOA development ( Fig. 3 ).
Index visit (
Knees with higher WORMS medial tibia (MT) cartilage lesion scores were at significantly higher odds for developing AKOA. Furthermore, knees with higher medial and lateral tibia BMEP scores at the index visit were at higher odds for AKOA development. One insufficiency fracture was identified in the AKOA and the control group, respectively.
T2 Relaxation Time Measurements
The results for T2 relaxation time measurements assessed at the index visit for both groups are shown in Table 4 . Differences for cartilage T2 values were nonsignificant for all cartilage compartments and global knee T2 values (P > 0.191).
Cartilage T2. a
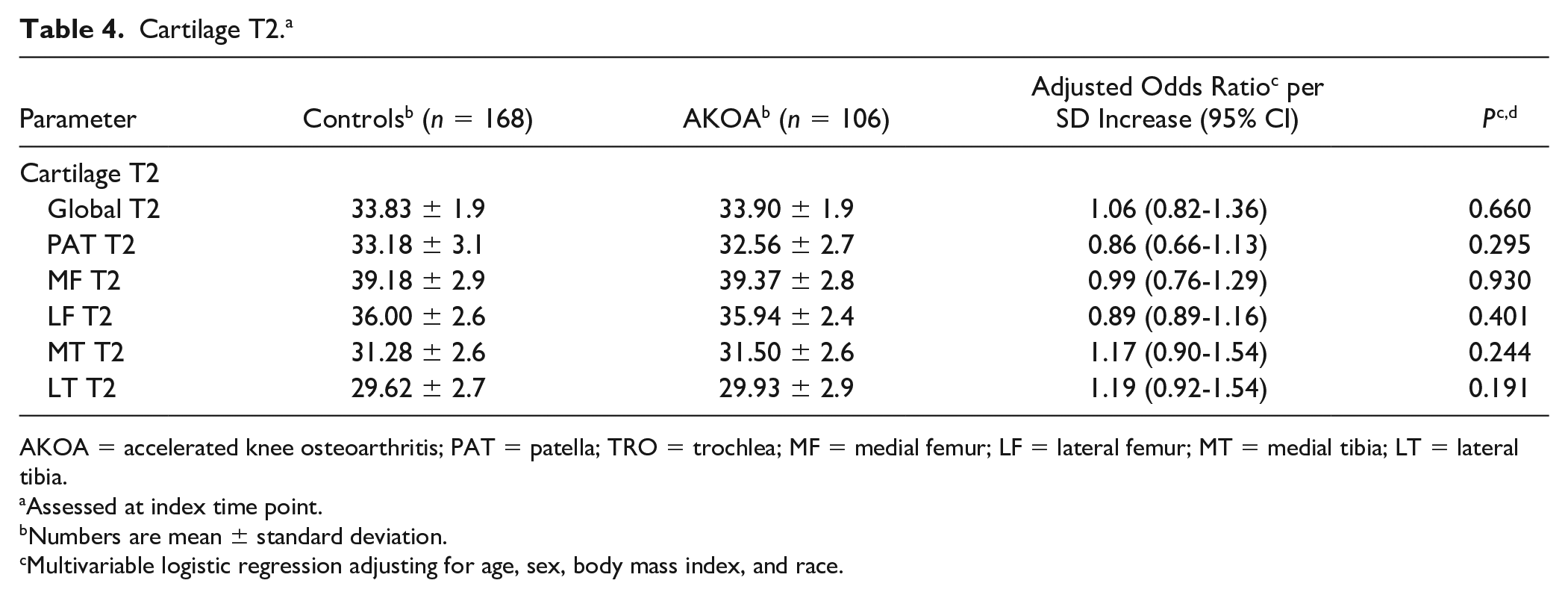
AKOA = accelerated knee osteoarthritis; PAT = patella; TRO = trochlea; MF = medial femur; LF = lateral femur; MT = medial tibia; LT = lateral tibia.
Assessed at index time point.
Numbers are mean ± standard deviation.
Multivariable logistic regression adjusting for age, sex, body mass index, and race.
Discussion
In this study, we found meniscal damage, especially meniscal root tears and extrusion to be highly significant risk factors for AKOA development. Moreover, medial tibia cartilage damage and tibial BMEP were also significantly associated with AKOA development, while altered biochemical cartilage composition was not a significant risk factor.
Among demographic and clinical correlates, subjects later developing AKOA were older compared to subjects with a more gradual OA onset. Higher BMI was not associated with AKOA in univariate or multivariate analyses. While elevated BMI is a well-established risk factor for incident knee OA,10,34 it may be less useful to distinguish subjects at risk of AKOA from subjects with a more gradual OA onset. Baseline WOMAC knee stiffness scores and KOOS pain scores for bending the knee fully were significantly higher in AKOA subjects. Since loss of knee flexion is frequently observed in subjects with meniscal root tears or other meniscal abnormalities, 35 these symptoms could be useful to identify subjects that would benefit from an MRI to identify morphological pathologies associated with rapid cartilage loss. These subjects could then receive treatment for these pathologies to prevent AKOA such as meniscal repair surgery. 36 Recent studies demonstrated promising results using surgical techniques such as arthroscopic pullout suture for meniscal root tears37-39 or arthroscopic direct extrusion reduction to treat meniscal extrusion.40,41 Studies comparing different approaches to treat posterior medial meniscal root tears found that anatomic transtibial pull-out root repair (with and without centralization suture into the posterior medial tibial plateau) best restored contact mechanics in the knee, compared with nonanatomic repair states, 42 while partial meniscectomy surgery or nonoperative management was associated with poor clinical outcomes and high arthroplasty rates.43,44
Previous studies demonstrated that meniscal damage could be an important morphological risk factor for AKOA development: Roemer et al. 13 identified meniscal extrusion and presence of meniscal abnormalities as risk factors for slow and fast tibiofemoral cartilage loss over 30 months comparing both types of cartilage loss to a reference group of knees without cartilage loss. Davis et al. 12 studied the agreement between self-reported knee injury and distinct structural changes in subjects developing AKOA or a more standard rate of OA development. Distinct structural changes most commonly described in AKOA subjects, were medial meniscal lesions such as root or radial tears. 12 We identified several measures of meniscal damage as risk factors for AKOA, including higher scores of the medial and lateral body, and lateral posterior horn. Specifically, root tears and meniscal extrusion were strongly associated with AKOA development. Root tears are assumed to profoundly impact knee health, creating biomechanical changes similar to that of a total meniscectomy.15,45-48 Meniscal extrusion has also previously been identified as a risk factor for cartilage loss and is frequently associated with root tears.13,15,45
Regarding other morphological features, medial tibia cartilage damage was the only cartilage feature significantly associated with AKOA while other cartilage features were nonsignificant. Initial tibial cartilage volume was previously identified as an important factor influencing the overall amount of cartilage loss, 49 though medial and lateral compartment were not analyzed separately. Interestingly, high tibial BMEP scores at baseline were also associated with AKOA development in our study. Since compartments with higher baseline BMEP scores are at risk of greater cartilage loss, 50 higher baseline BMEP scores of the tibia may be related to increased tibial cartilage loss. These findings suggest that tibial cartilage damage, more specifically damage of the medial tibia cartilage could be an important factor initiating, or occurring early in, the development of AKOA. While cartilage composition is a known risk factor for incident knee OA,19-21 biochemical cartilage alteration was not a factor that distinguished between AKOA and a normal rate of OA development. Overall mean T2 values of all compartments exhibited no clear differences between groups, suggesting a limited impact of cartilage composition on AKOA development.
Some limitations are pertinent to this study. Since the patellofemoral joint was not assessed in the KL-based definition used for subject selection, some study knees likely had significant patellofemoral OA at the index visit. However, WORMS patella cartilage and patella BMEP scores were not associated with AKOA. In order to avoid misclassifying AKOA knees as normal OA, those who did not have follow-up radiograph readings 4 years after the index time point were excluded. As a result, a small number of knees were excluded that developed AKOA at an earlier time point but lacked 4-year follow-up readings (5 due to a subsequent knee replacement, 5 due to missing radiographs), and this may have influenced our results.
In conclusion, we identified meniscal damage, especially meniscal extrusion and meniscal root tears as risk factors for AKOA development. Given the rapid pace of cartilage loss in subjects with AKOA and subsequent short opportunity to intervene, our findings contribute to identifying subjects at risk of AKOA at an early stage when preventative measures targeting modifiable risk factors such as meniscal repair surgery could still be effective.
Footnotes
Acknowledgments and Funding
We would like to thank the participants and staff of the Coordinating Center of the OAI for their invaluable assistance with patient selection, statistical analysis, and technical support. The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the OAI, a public-private partnership comprising 5 NIH contracts (National Institute of Arthritis and Musculoskeletal and Skin Diseases contracts N01-AR-2-2258, N01-AR-2-2259, N01-AR-2-2260, N01-AR-2-2261, and N01-AR-2-2262), with research conducted by the OAI Study Investigators. The study was also funded in part by the Intramural Research Program of the National Institute on Aging, NIH. Private funding partners include Merck Research, Novartis Pharmaceuticals, GlaxoSmithKline, and Pfizer; the private sector funding for the OAI is managed by the Foundation for the National Institutes of Health. The analyses in this study were funded through the NIH/NIAMS (National Institute of Arthritis and Musculoskeletal and Skin Diseases grant R01AR064771).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was compliant with the Health Insurance Portability and Accountability Act and was approved by the local institutional review boards of all participating centers.
Informed Consent
Informed consent was obtained from all participants.
Trial Registration
Not applicable.