
Abstract
Objective
In end-stage knee osteoarthritis, total knee arthroplasty (TKA) may finally become inevitable. At a relatively young age, this comes with the risk of future revision surgery. Therefore, in these cases, joint preserving surgery such as knee joint distraction (KJD) is preferred. Here we present 5-year follow-up data of KJD.
Design
Patients (n = 20; age <60 years) with conservative therapy resistant tibiofemoral osteoarthritis considered for TKA were treated. Clinical evaluation was performed by questionnaires. Change in cartilage thickness was quantified on radiographs and magnetic resonance images (MRI). The 5-year changes after KJD were evaluated and compared with the natural progression of osteoarthritis using Osteoarthritis Initiative data.
Results
Five-years posttreatment, patients still reported clinical improvement from baseline: ΔWOMAC (Western Ontario and McMaster Universities Arthritis Index) +21.1 points (95% CI +8.9 to +33.3; P = 0.002), ΔVAS (visual analogue scale score) pain −27.6 mm (95%CI −13.3 to −42.0; P < 0.001), and minimum radiographic joint space width (JSW) of the most affected compartment (MAC) remained increased as well: Δ +0.43 mm (95% CI +0.02 to +0.84; P = 0.040). Improvement of mean JSW (x-ray) and mean cartilage thickness (MRI) of the MAC, were not statistically different from baseline anymore (Δ +0.26 mm; P = 0.370, and Δ +0.23 mm; P = 0.177). Multivariable linear regression analysis indicated that KJD treatment was associated with significantly less progression in mean and min JSW (x-ray) and mean cartilage thickness (MRI) compared with natural progression (all Ps <0.001).
Conclusions
KJD treatment results in prolonged clinical benefit, potentially explained by an initial boost of cartilaginous tissue repair that provides a long-term tissue structure benefit as compared to natural progression. Level of evidence, II.
Introduction
Tibiofemoral knee osteoarthritis is a progressive degenerative joint disease affecting all joint tissues, most prominently the articular cartilage. The disease is characterized by persistent pain, soft tissue impairment, subchondral bone changes, and cartilage tissue damage and loss (visualized on radiographs and/or MRI), all together reducing joint function. 1 The disease has a major impact on health care costs and quality of life, significantly affecting labor participation. Accurate data on incidence and prevalence of knee osteoarthritis in literature are lacking because of absence of a clear definition of the disease. Yet, knee osteoarthritis is considered the most common type of osteoarthritis and affects approximately 6% of the adult population worldwide, with increasing age reaching up to 40% for those older than 70 years. 2 Furthermore, more recent data show that 13.8% of the population >45 years is diagnosed with symptomatic knee osteoarthritis, and this number is predicted to increase to 15.7% in 2032. 3 The incidence is significantly increasing due to aging of the population, with a preferred active lifestyle at a relatively older age, as well as the significant increase in obesity at younger age, both being important predictors for disease development and progression. 4
If conservative treatment fails and pain or joint function becomes unbearable, several surgical options are indicated. In case of relatively young and physically active patients (<65 years), joint preserving surgery is preferred. 5 This is because a total knee arthroplasty (TKA) at this age, where patients still have an active lifestyle, is less successful than in the elderly, with high revision rates of up to 44% later in life.6,7
Recently, knee joint distraction (KJD) treatment has been proposed as an effective and joint saving treatment. It is an experimental surgical procedure in which the 2 bony ends of a joint are gradually separated to a certain extent for a certain period of time, by use of an external fixation frame.8,9 It was demonstrated that this treatment results in cartilaginous tissue repair by use of digitally analyzed standardized radiography, quantitative magnetic resonance imaging (MRI) analyses, and biochemical analysis of collagen type II up to 2 years after distraction.10-15 However, the durability of this clinical effect as well as of the cartilage tissue structure repair has not yet been evaluated.
In the present study, we have followed the first 20 KJD patients to evaluate the durability of the clinical benefit and the observed cartilaginous tissue repair, abutting the earlier reported 1- and 2-year follow-up.14,15 Additionally, a control group was selected, using data from the Osteoarthritis Initiative (OAI), to compare cartilaginous tissue repair over time after KJD with the natural progression rate of cartilage damage in case of no or conservative treatment.
Methods
Patients Selection
From 2006 to 2008, a total of 20 patients with primarily tibiofemoral knee osteoarthritis and with persistent pain refractory to conservative therapy (average age 48.5 years, range 32-57 years; 45% females; body mass index [BMI] 29.6 kg/m2, range, 25-36 kg/m2) were included at the Department of Orthopedics, University Medical Center Utrecht (UMCU). Patient characteristics have been described in detail previously. 15 These patients were referred and indicated by their orthopedic surgeon for TKA, based on clinical examination (visual analogue scale score (VAS) for pain of ≥60 mm) and radiographic examination (signs of primarily tibiofemoral cartilage tissue loss), and they had to be less than 60 years of age. Because of their relative young age, KJD was proposed as an experimental alternative for the indicated TKA. Patients were excluded in case of primary patellofemoral OA, if a history of inflammatory or septic arthritis existed, in case of severe varus/valgus malalignment (>10°), and in case of psychological inabilities to cope with an external fixation fame. The medical ethical committee of the UMCU approved the study (No. 04/086). All patients gave written informed consent.
Distraction Method
The distraction method was applied as previously described by Intema et al., 14 using a proof-of-concept distraction device consisting of 2 external bilaterally placed dynamic monotubes, fixed on 2 bone-pins at each end, bridging the knee joint (see Fig. 1 ). Distraction was applied in stages until 5 mm was reached, confirmed by radiography. KJD treatment lasted for 2 months (average 60 days, range 54-64 days) and was every 2 weeks shortly interrupted during which continuous passive motion (CPM) was performed (average 25° flexion, range 15° to 80°). After reinstalling the distraction tubes actual distraction was checked by radiography. Throughout the whole treatment patients were allowed and encouraged to load the distracted joint with full weight bearing capacity, supported with crutches if needed. Pin-tract infections were successfully treated with flucloxacillin for 5 to 7 days. After removal of the tubes and pins at daycare surgery, patients were discharged without imposed functional restrictions.
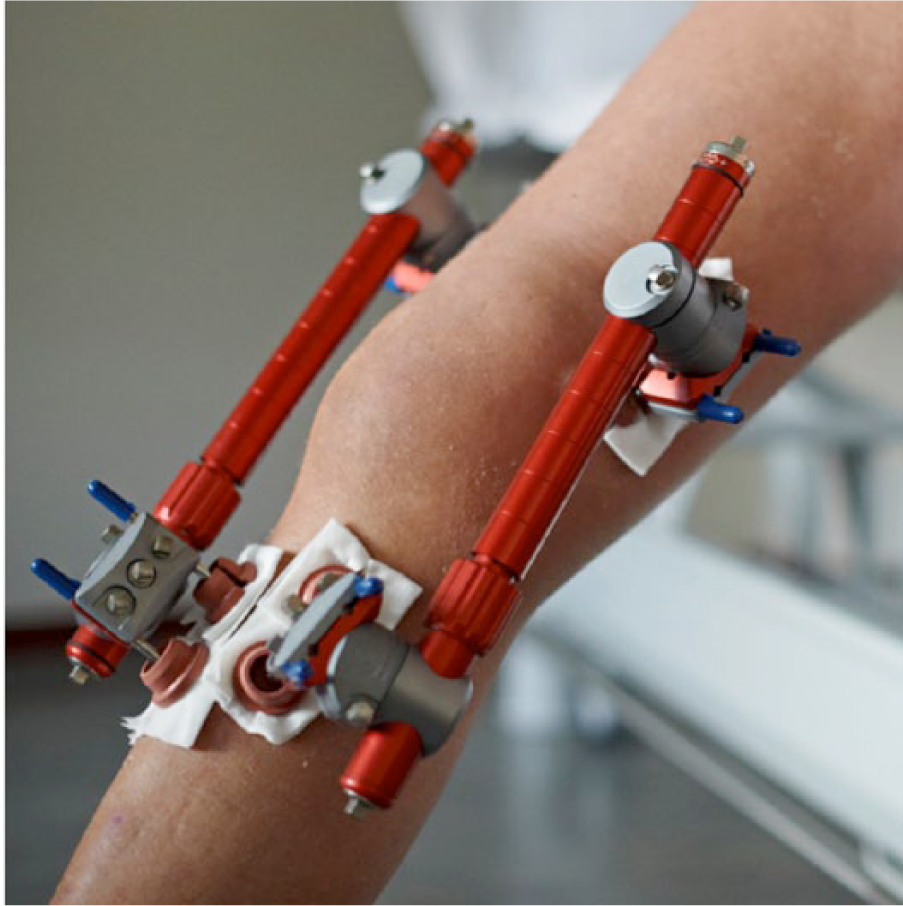
The bilateral external fixation frame used for knee joint distraction treatment.
Follow-up
Patient-reported outcome measurements (PROMs) were collected twice at baseline and at 3, 6, 12, 18, and 24 months’ follow-up as reported14,15 and subsequently every year. Structural outcome parameters were assessed at baseline and 1, 2, and 5 years’ follow-up. No data were gathered over time on posttreatment medication or physiotherapy as this was on personal demand.
Clinical Outcome, PROMs
The Western Ontario and McMaster Universities Arthritis Index (WOMAC) questionnaire (version 3.0, normalized to a 100-point scale for total and subscales; “100” being the best score) including 3 domains (pain, function, and stiffness) was used as primary outcome parameter. 16 The secondary clinical outcome parameter was the VAS pain score (0-100 mm; “0” meaning no pain).
Structural Outcome
Radiographic Analysis
Standing, weight bearing, semiflexed, posterior-anterior radiographs were taken, with a magnification/density reference in view, according to the KIDA (Knee Images Digital Analyses) protocol. 17 Images were digitally mathematically analyzed independent of subjective clinical reader interpretation, by an experienced observer. Minimum and mean joint space width (JSW) of the most affected compartment (MAC; medial n = 18, lateral n = 2) are presented. Reproducibility of this technique has been reported. 17
Quantitative MRI Analysis
MRI analyses were performed as described earlier 15 with the use of custom software (Chondrometrics GmbH, Ainring, Germany). In short, coronal MRIs of the tibiofemoral cartilage plates were acquired using a 1.5 T Philips Achieva, with a SENSE T/R knee coil and a 3-dimensional spoiled gradient recalled (SPGR) imaging sequence with fat suppression (repetition time 20 ms; echo time 9 ms; flip angle 15°; slice thickness 1.5 mm; in-plane resolution 0.3125 × 0.3125mm. 18 Similar as for the 1-year follow-up analyses, 14 5-year follow-up images were segmented with reference to the baseline images, which were segmented again to minimize intra- and inter-observer variability, and to ensure blinding of the reader and quality control reader to the temporal sequence of the images.
The primary outcome parameter was the mean cartilage thickness over the total subchondral bone area (ThCtAB) and the percentage of denuded subchondral bone area (dABp), that is, without cartilage coverage. 19 All parameters were calculated for the MAC. The reproducibility of this type of analyses has been published before in detail.20-22
Control Group From the Osteoarthritis Initiative
The control group was composed from the Osteoarthritis Initiative (OAI) database. The OAI is an ongoing multicenter study (http://www.oai.ucsf.edu) targeted at identifying sensitive biomarkers of onset and progression of knee osteoarthritis. 23
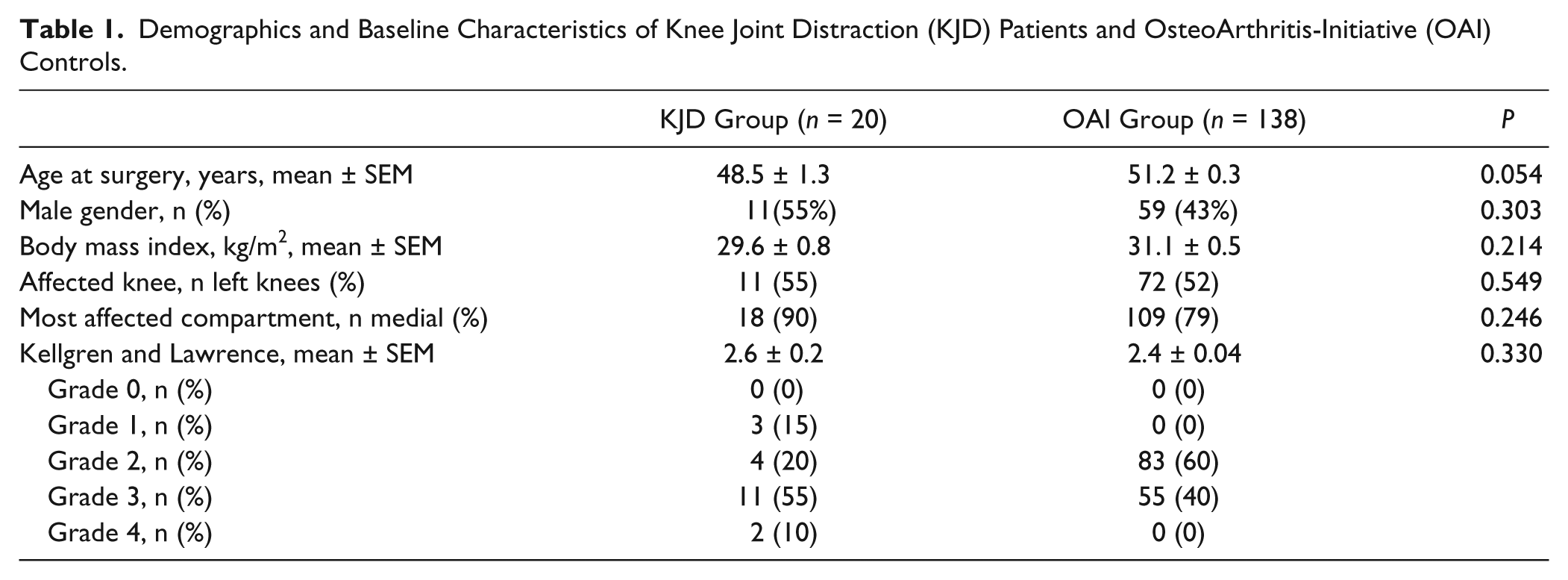
Data were selected from the progression subcohort (n = 1390), in order to select a group comparable at baseline with our KJD patients. In this subcohort, the patients had at least 1 knee with definite osteophytes (Kellgren and Lawrence grade [KLG] ≥ 2) and frequent knee symptoms at baseline. All patients ≤60 years of age, without TKA during follow-up and with available radiographic JSW measurements at 4 years’ follow-up, and/or quantitative MRI measurements (ThCtAB and dABp) available at 2 years’ follow-up (longest follow-up for both parameters available) were selected. This resulted in 138 patients for the OAI control group (baseline characteristics; Table 1 ).
Demographics and Baseline Characteristics of Knee Joint Distraction (KJD) Patients and OsteoArthritis-Initiative (OAI) Controls.
Since in the OAI radiographic measurements were only available up to 4 years and quantitative MRI measurements up to 2 years, the value of outcomes and change scores (for radiographic mean and minimum JSW and the quantitative MRI measurements (ThCtAB and dABp) of the MAC) at 5-year follow-up was calculated assuming a linear progression over time.24,25
Statistical Analysis
For all parameters mean values ± standard error of the mean (SEM) are given, at each time point. In case of double baseline measurements, these were averaged. Statistics for comparison of posttreatment follow-up outcomes with baseline values was performed by 2-sided paired t tests. For comparison of changes in structural outcome parameters over 5 years between patients after KJD and controls multivariable regression analysis was used, with adjustment for the respective baseline values for the outcome and confounders. A stepwise selection procedure was used starting with all baseline variables ( Table 1 ) and removing them one-by-one based on change (≤5%) of the regression coefficient of the variable “group” (KJD group or OAI group). Mean changes are presented with a 95% confidence interval (95%CI). P ≤ 0.05 was considered statistically significant. For all statistical tests, IBM SPSS Statistics version 20.0.0 was used.
Results
Patients
In total, 2 patients withdrew consent for further follow-up, one after 2 years and one just before 5 years’ follow-up. Three other patients underwent TKA because of unsatisfactory/declining clinical benefit, at 3.8, 4.4, and 4.8 years (mean 4.3 ± 0.5) after KJD treatment. For all missing data, the last observation was carried forward for evaluation.
Clinical Benefit
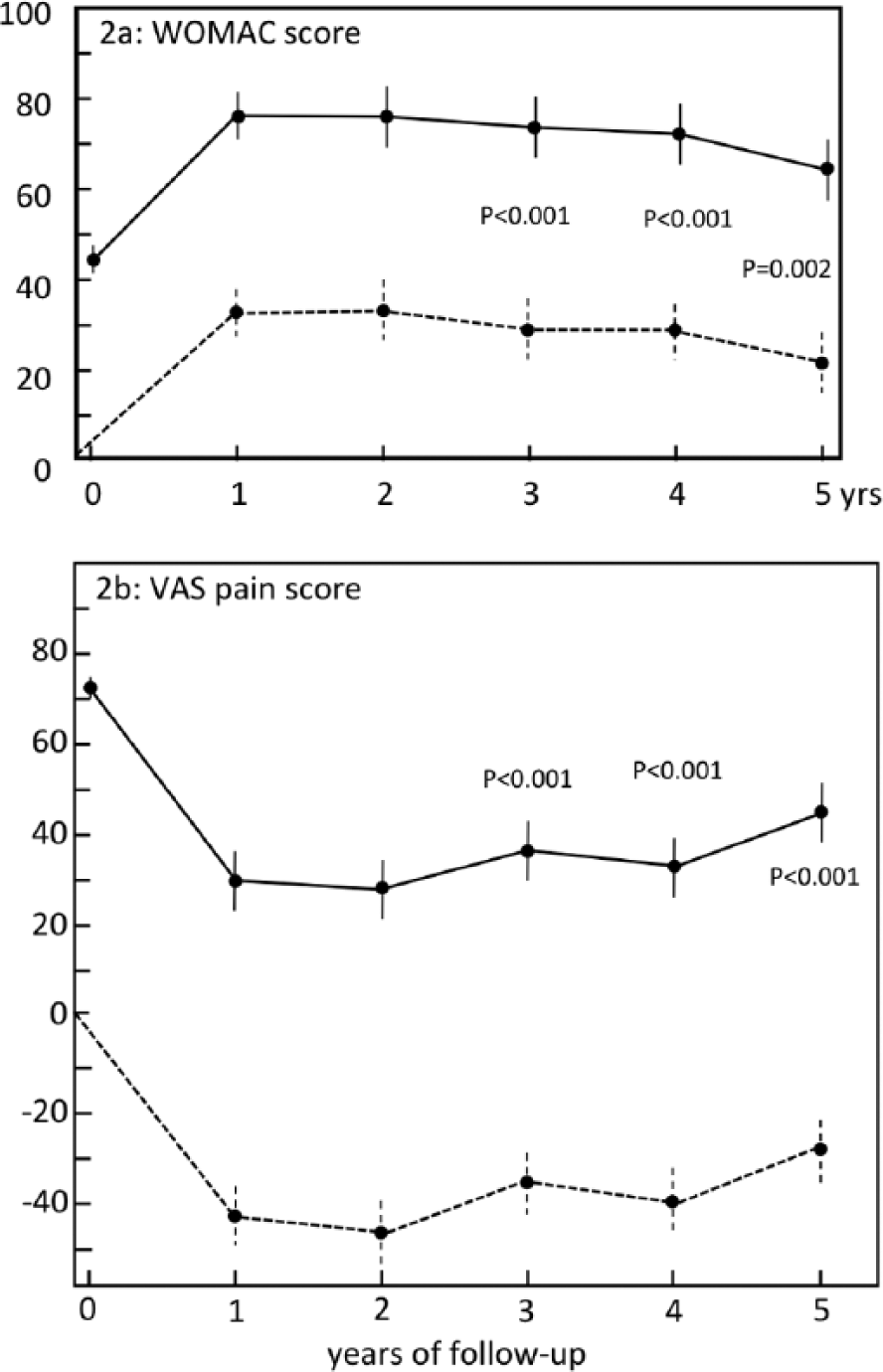
As for the published 1- and 2-year follow-up (Intema et al. 14 and Wiegant et al. 15 ), at 3 to 5 years’ follow-up, the WOMAC scores were statistically significant improved as compared to pretreatment values ( Table 2 ; Fig. 2a ), although over time the clinical benefit tended to decrease (not statistically significant). WOMAC total scores were at baseline: 43.9 ± 3.3 vs. 72.9 ±5.6 (P < 0.001) at 3 years’ follow-up; vs. 73.0 ± 5.4 (P < 0.001) at 4 years’ follow-up; vs. 65.1 ± 5.6 (P = 0.002) at 5 years’ follow-up. The changes compared with baseline for each patient, presented as mean with 95% CI for the whole group are presented in Figure 2a and Table 3 .
Overview of All Clinical and Structural Parameters at Baseline and at 1, 2, and 5 Years’ Follow-up for the Knee Joint Distraction (KJD) Group. a
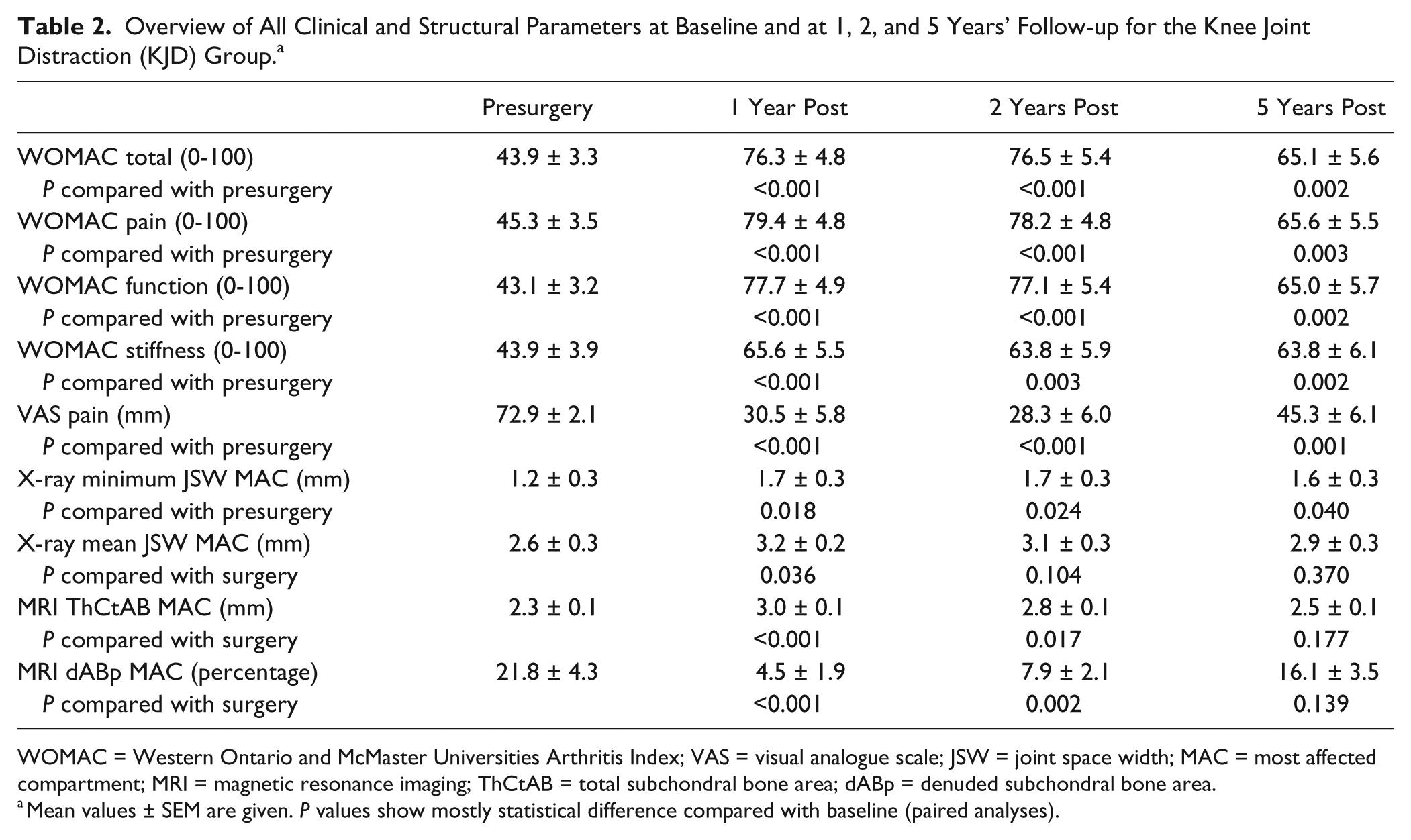
WOMAC = Western Ontario and McMaster Universities Arthritis Index; VAS = visual analogue scale; JSW = joint space width; MAC = most affected compartment; MRI = magnetic resonance imaging; ThCtAB = total subchondral bone area; dABp = denuded subchondral bone area.
Mean values ± SEM are given. P values show mostly statistical difference compared with baseline (paired analyses).
Clinical outcome parameters. WOMAC (Western Ontario and McMaster Universities Arthritis Index) total (
Overview of All Changes at 5 Years Compared With Baseline for All Clinical Parameters for the Knee Joint Distraction (KJD) Group. a
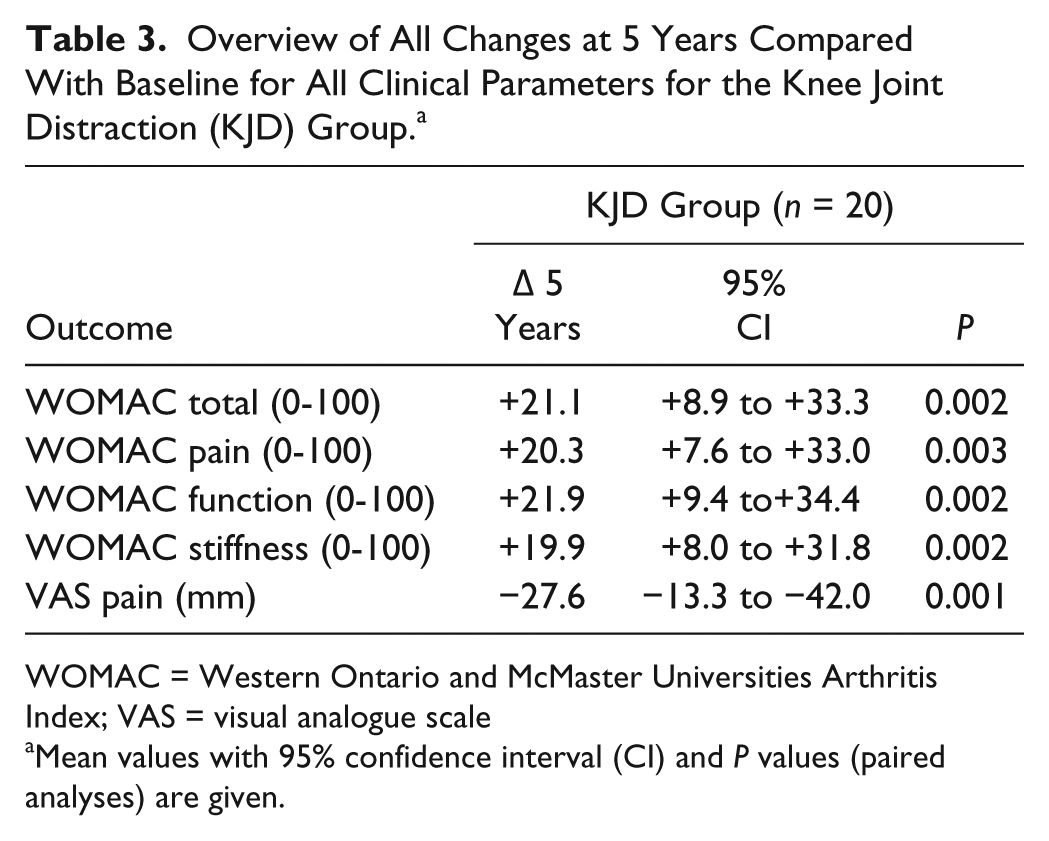
WOMAC = Western Ontario and McMaster Universities Arthritis Index; VAS = visual analogue scale
Mean values with 95% confidence interval (CI) and P values (paired analyses) are given.
Values for the 3 WOMAC subscores were statistically significant improved over 3 to 5 years’ follow-up as well ( Table 2 ); baseline versus 5 years’ follow-up for pain (45.3 ± 3.5 vs. 65.6 ± 5.5, P = 0.003), for stiffness (43.9 ± 3.9 vs. 63.8 ± 6.1, P = 0.002), and for function (43.1 ± 3.2 vs. 65.0 ± 5.7, P = 0.002). The changes compared with baseline for each patient, presented as mean with 95% CI for the whole group are presented in Table 3 .
As for WOMAC scores, the VAS pain score was statistically significantly improved at 3, 4, and 5 years’ follow-up as compared with pretreatment values: 72.9 ± 2.1 versus 37.0 ± 6.1 (P < 0.001) at 3 years’ follow-up; versus 33.3 ± 5.8 (P < 0.001) at 4 years’ follow-up; and versus 45.3 ± 6.1 (P < 0.001) at 5 years’ follow-up ( Fig. 2b ; Tables 2 and 3 for absolute values and changes from baseline, respectively).
Structural Outcome
KJD Group
Minimum JSW of the MAC at 5 years posttreatment was still increased as compared with pretreatment values (baseline, 1.2 ± 0.3 mm vs. 5 years, 1.6 ± 0.3mm; Δ +0.43mm, 95% CI, +0.02 to +0.84mm; P = 0.040) ( Fig. 3a ; Tables 2 and 4 ). Mean JSW of the MAC was not statistically significant different from pretreatment values anymore (baseline, 2.6 ± 0.3 mm vs. 5 years, 2.9 ± 0.3mm; Δ +0.26 mm, 95% CI = −0.33 to +0.85 mm; P = 0.370) ( Fig. 3b , Tables 2 and 4 ).
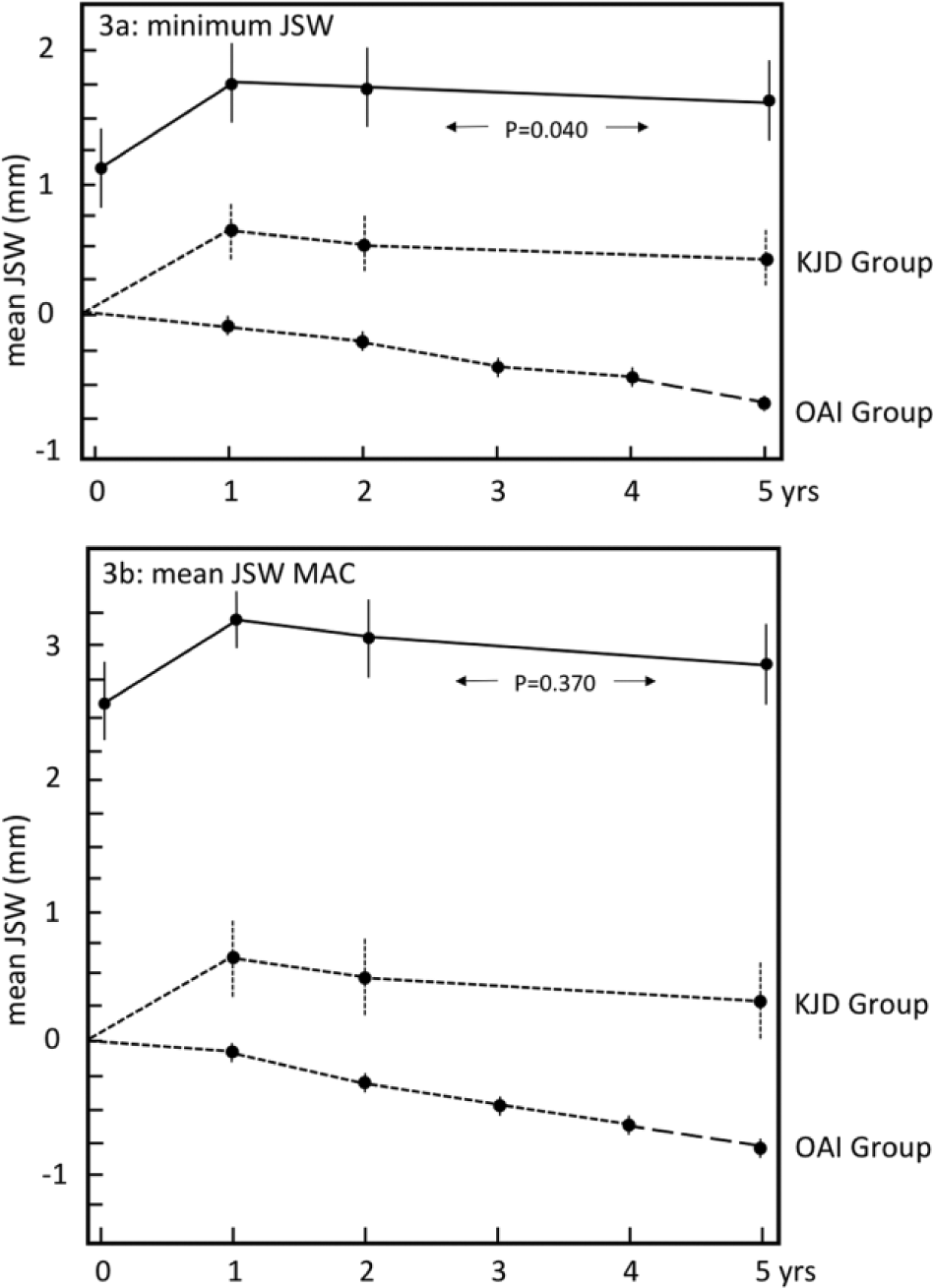
Radiographic structural outcome parameters. Minimum (
Overview of All Changes at 5 Years Compared With Baseline for All Structural Parameters for the KJD Group and the OAI Group. a
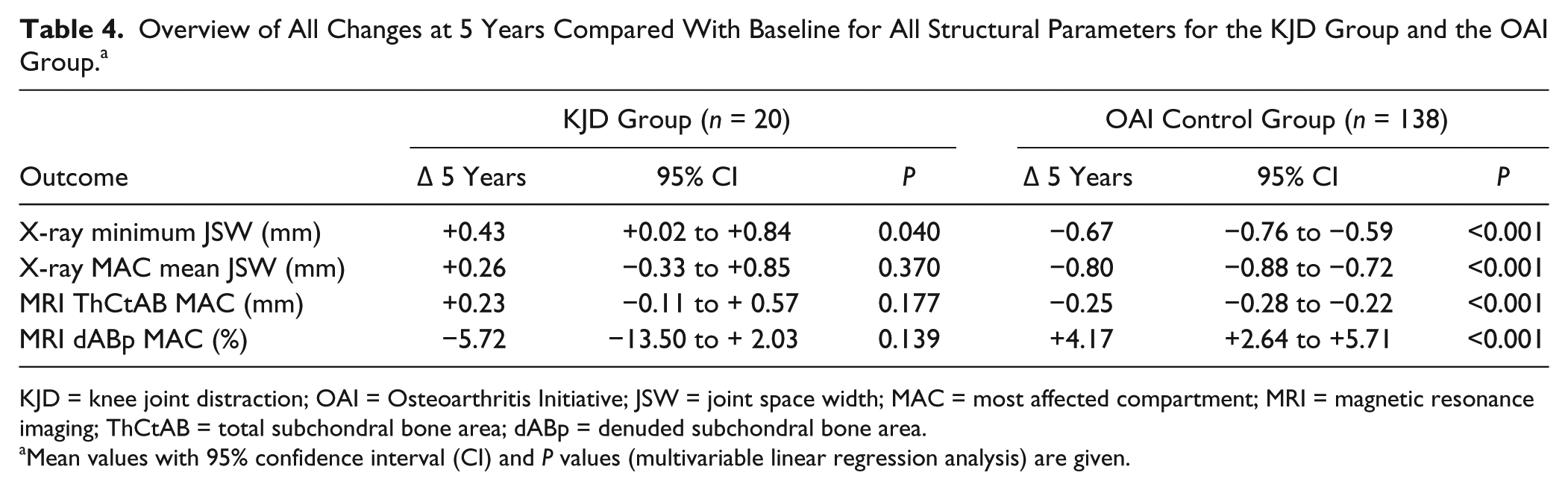
KJD = knee joint distraction; OAI = Osteoarthritis Initiative; JSW = joint space width; MAC = most affected compartment; MRI = magnetic resonance imaging; ThCtAB = total subchondral bone area; dABp = denuded subchondral bone area.
Mean values with 95% confidence interval (CI) and P values (multivariable linear regression analysis) are given.
The quantitative MRI analysis showed at 5 years’ follow-up that the mean cartilage thickness of the MAC on MRI was not statistically significant different from pretreatment values anymore (ThCtAB: baseline, 2.3 ± 0.1 mm vs. 5 years, 2.5 ± 0.1 mm; Δ +0.23 mm, 95% CI, −0.11 to +0.57 mm; P = 0.177), due to a gradual decrease of the initial increase at 1 and 2 years (Intema et al. 14 and Wiegant et al. 15 ) ( Fig. 4a ; Tables 2 and 4 ). The same was observed for the average percentage denuded bone area of the MAC on the MRI (dABp: baseline, 21.8% ± 4.3% vs. 5 years, 16.1% ± 3.5%; Δ −5.72%, 95% CI, −13.50% to +2.03%; P = 0.139) ( Fig. 4b , Tables 2 and 4 ).
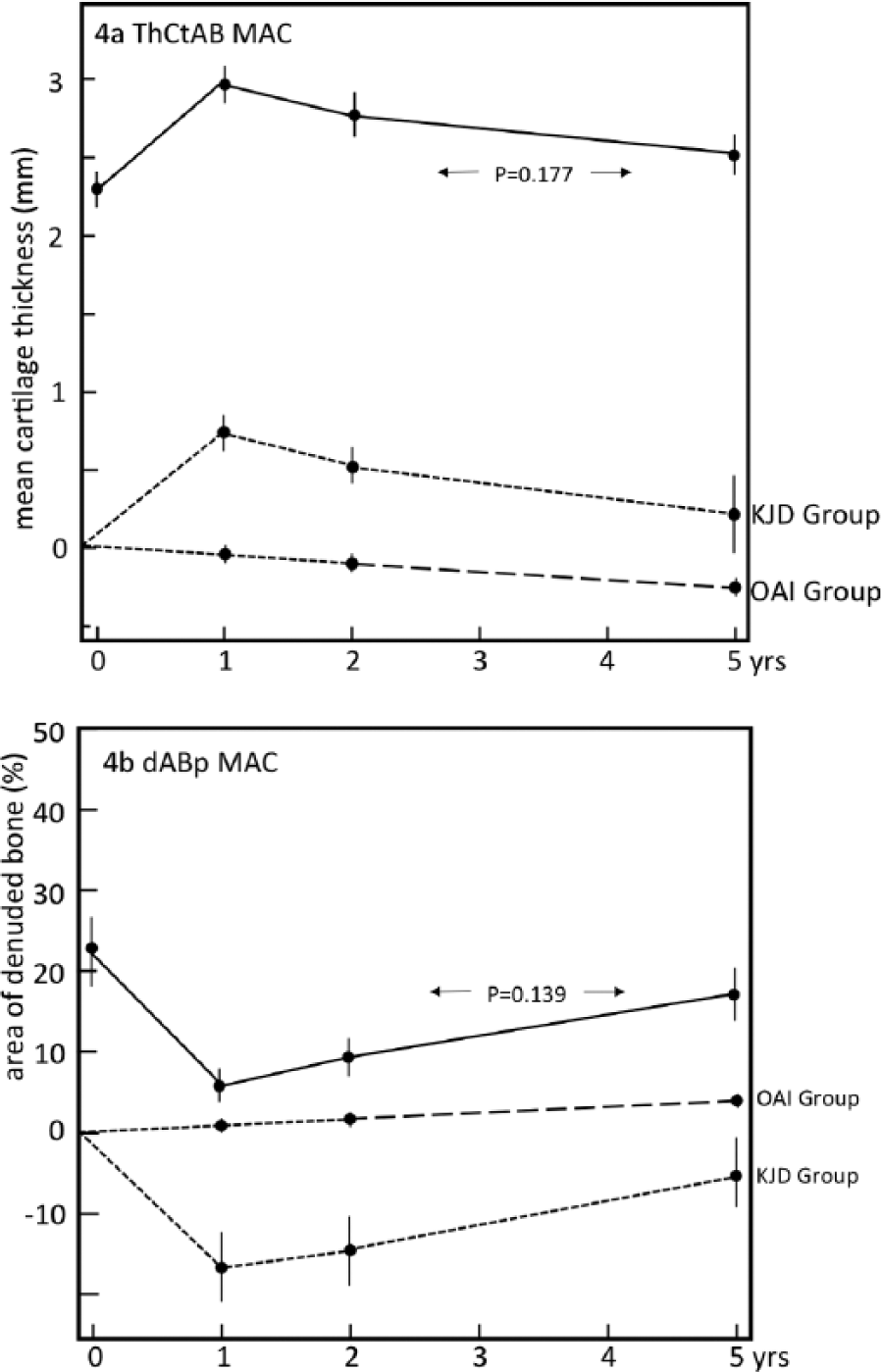
Magnetic resonance imaging (MRI) structural outcome parameters. Mean cartilage thickness (
Adverse Events
During distraction treatment, 17 out of the 20 patients had had single or multiple pin tract infections, and could be treated adequately with antibiotics Two patients suffered from pulmonary embolism, treated according to guidelines with oral anticoagulants for 6 months. At 6-month follow-up, knee flexion was still decreased by 9° (±4.5°). After this initial fall in joint flexion, levels returned to baseline levels after 1 year (121° ± 4.0° at baseline, and 123° ± 3.7° at 1 year). These levels of joint flexion were maintained at the 2-year follow-up (123° ± 3.3°).
Comparison With OAI Group
The KJD group and OAI control group were not statistically significantly different regarding demographic baseline values and severity of osteoarthritis ( Table 1 ).
In the OAI group, the mean JSW of the MAC decreased from 4.93 ± 0.12 mm at baseline to an extrapolated value of 4.13 ± 0.14 mm at 5 years (Δ −0.80 mm, 95% CI, −0.88 to −0.72 mm) ( Fig. 3b ; Table 4 ). The minimum JSW of the MAC showed similar results, with a decrease from 4.20 ± 0.14 mm at baseline to a extrapolated value of 3.52 ± 0.14 mm at 5 years (Δ −0.67 mm, 95% CI, −0.76 to −0.59 mm) ( Fig. 3a ; Table 4 ). The mean cartilage thickness (ThCtAB) of the MAC decreased from 3.47 ± 0.06 mm at baseline to an extrapolated value of 3.22 ± 0.06 mm at 5 years (Δ −0.25 mm, 95%CI, −0.28 to −0.22 mm) in the OAI group ( Fig. 4a ; Table 4 ). The same was observed for the extrapolated average percentage denuded bone area of the MAC on the MRI images (dABp: baseline, 4.0% ± 0.8% vs. an extrapolated value at 5 years: 8.1% ± 1.5%; Δ 4.17%, 95% CI, +2.64% to +5.71%) ( Fig. 4b , Table 4 ).
Multivariable linear regression analysis indicated that KJD treatment was associated with significantly less progression in mean JSW, min JSW, mean cartilage thickness, and average percentage denuded bone area (adjusted for the respective baseline values and confounders age, and KL grade) when compared with the “natural progression” in the OAI group over 5 years. The “regression coefficient” (β) for KJD was negative for dABp (−17.49), indicating that patients in the KJD group would on average have a 17.49% (95% CI, −21.96 to −13.03, P < 0.001) lower progression of percentage denuded bone area when compared with patients in the OAI group. For mean JSW, the β for KJD was positive (0.76), indicating that patients in the KJD group have on average a 0.76 mm (95%CI, 0.50 to 1.02, P < 0.001) lower progression of the mean JSW when compared with patients in the OAI group. The β for KJD in the analysis of minimum JSW was 0.83 (95%CI, 0.59 to 1.08, P < 0.001) and for mean cartilage thickness (ThCtAB), it was 0.35 (95%CI, 0.24 to 0.46, P < 0.001).
Discussion
Five years after KJD, >80% of patients were still satisfied. There appeared to be a sustained clinical benefit and most patients lack the need for additional surgical intervention. Three out of 18 patients underwent TKA within the 5 years of follow-up (on average >4 years after KJD). Moreover, in 2 of the 3 secondary TKAs (all performed without any complications and with good results), WOMAC and pain scores were, despite of being decreased over the last year of follow-up, still significantly improved compared to pretreatment values (individual data not shown). Apparently a relative worsening of physical condition and pain, despite still improved compared with pretreatment conditions, is sufficient to prefer a subsequent alternative treatment.
The question is whether failure over time to KJD can be predicted by, for example, patient’s demographics or clinical condition? Unfortunately, no predictors could be identified in this still limited numbers of patients treated. Recently, 42 patients have been treated with KJD in 2 randomized controlled trials comparing KJD with high tibial osteotomy and with TKA. 26 Based on such numbers a prediction of failure to KJD might be found in the future. However, in over a 110 patients treated with joint distraction in case of ankle osteoarthritis only female gender appeared predictive of failure. 27 Finding reliable predictors would narrow criteria for treatment and facilitate implementation, because failure on such a demanding treatment should be avoided.
Another issue is whether KJD, in case clinical benefit is declining over the years, can be repeated or followed by other joint preserving surgical treatments such as osteotomy? This might be relevant in case patients are still younger than 65 years and joint preserving treatment is still favorable. A second joint distraction procedure has been performed sporadically in cases of ankle OA, 28 several years after the first treatment, with good clinical results. Whether this is also possible for knee osteoarthritis needs future study. This approach seems worthwhile to explore based on the initial 1 to 2 years’ cartilaginous repair followed by progression of damage with a rate very similar to natural progression.
Although patients have a stiff knee joint for 8 weeks, which limits their activities in daily life, almost all patients consider the treatment “worth the investment.” Also the frequently occurring pin-tract infections (reported on previously14,15 needing antibiotic treatment) were not considered of such a burden that patients would have refused KJD treatment. At present even subsequent treatment of the other osteoarthritic knee is performed on patient’s request. Clearly, factual information to patients about durability, burden, and risks is a prerequisite before general implementation can be started. Also proper pin tract care protocols and anti-coagulation to prevent embolism, as well as care to regain full joint motion after treatment are of utmost importance.
Originally, in the present study no control group was included. In fact, this is difficult, as patients need treatment in one or the other way in this debilitating stage of the disease. Therefore, in this study natural progression of osteoarthritis was determined in a control group with comparable patient characteristics (demographic and severity of osteoarthritis) at baseline. Although both groups were comparable at baseline there were also some limitations with this approach. The OAI control group only had radiographic measurements available up to 4 years and quantitative MRI measurements up to 2 years. Therefore, the 5-year follow-up date of the MAC for the OAI patients were calculated considering the natural progression rate to be linear over time, which is a reasonable assumption according to recent literature.24,25 Patients in the OAI group were slightly older (on average 2.3 years). It may be debated if in younger patients the progression rate will be higher considering the higher activity level of such younger patients. In that case, we may have overestimated the natural progression in the OAI group. On the other hand, patients that underwent TKA in the OAI group were excluded (worst cases) probably leading to an underestimation of actual progression in this group. Irrespectively, this population is the only one with comparable baseline characteristics and with longitudinal MRI and X-ray data available and as such might be considered the best available control.
Interestingly, after the first initial substantial increase in JSW on radiographs, and substantial increase in cartilage thickness on MRI upon KJD, the subsequent gradual decrease in these parameters over time seem to parallel with the rate of progression in the OAI group. Apparently, the cartilaginous tissue repair takes place in the first (2) year(s) and subsequently natural progression proceeds again. Irrespectively, the head start in the first year is maintained (statistically significant) over the subsequent 5 years.
In summary, KJD results in prolonged clinical benefit, potentially explained by an initial boost of cartilaginous tissue repair that provides long-term tissue structure benefit as compared with natural progression in the OAI group. KJD therefore represents a promising therapeutic option for young patients with severe knee osteoarthritis.
Footnotes
Acknowledgments and Funding
This study was funded by the Dutch Arthritis Association.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: FE is co-owner and CEO of Chrondrometics GmbH. All other authors declare that there is no conflict of interest.
Ethical Approval
The medical ethics committee of the University Medical Center Utrecht approved the study (No. 04/086).
Informed Consent
All patients gave written informed consent.
Trial Registration
Not applicable.