
Abstract
Purpose. To determine the 5-year success rate of the “all-inside” technique of arthroscopic meniscus suture and collagen membrane wrapping along with bone marrow blood injection, to evaluate the progression of degenerative changes and the impact of simultaneous anteriro cruciate ligament (ACL) reconstruction. Methods. Fifty-four consecutive patients with complex meniscal tears were treated with the previously described technique. The subjective scores (International Knee Documentation Committee 2000, Lysholm, EQ-5D-5L) and Barret clinical criteria of meniscal healing were recorded. Magnetic resonance images (MRIs) were assessed at 2 and 5 years postoperatively, using the Whole-Organ Magnetic Resonance Imaging Score (WORMS) criteria. Kaplan-Meier survival analyses were performed in order to assess the survivorship after the index procedure. Thirty-nine patients were divided into 2 groups: group A—isolated meniscus repair and group B—meniscus repair with concurrent ACL reconstruction. Results. Fifty-four patients were treated and 44 were available for analysis. There was a statistically significant improvement in subjective scores and clinical assessment between the preoperative, 2-year follow-up, and 5-year follow-up time points. EQ-5D-5L utility value was 0.9 ± 1 at final follow-up. The WORMS osteoarthritis severity grade had increased from 6.9 ± 5.0 points at the 2-year follow-up to 11.1 ± 9.6 points at the 5-year follow-up (P < 0.001). There was a significant difference between the groups after 60 months. The overall survival rate at final follow-up was 88%. Conclusions. The treatment option evaluated in this study has shown very good mid-term clinical and MRI-based outcomes as well as a favorable survival rate. Simultaneous ACL reconstruction is likely a factor for osteoarthritis progression.
Introduction
The importance of the meniscus in the knee is now commonly understood, and all major orthopedic societies recommend preservation of the meniscus.1,2 While a simple suture of the meniscus tear is the most common surgical technique, it has limited indications, with the best results obtained by suturing a simple type of tear in the red-red or red-white zone. 3 In recent years, there has been a growing trend in the use of biological factors to enhance regeneration and tissue healing of meniscal lesions.4,5 One of these strategies includes the all-inside technique of Arthroscopic Matrix-based Meniscus Repair (AMMR) using a collagen membrane repair accompanied by bone marrow blood aspirate injection.6,7
AMMR is an evolution of Henning’s concept to create a biological compartment with an optimal environment for meniscal healing. 8 Originally, the meniscal lesion was sutured then wrapped with periosteum from the pes anserinus region. This was later replaced by periosteum with collagen type-I matrix produced from porcine peritoneum. 9 Initial results were satisfactory but it was technically difficult and outcomes were not reproducible, thus a new technique (AMMR) was developed. 6 The 2-year follow-up results demonstrated that the technique is safe and can offer an option to save the meniscus in patients otherwise scheduled for meniscectomy. 7 Although early results were promising, longer observation was needed in order to verify the clinical utility of this procedure.
In this study, clinical outcomes, radiologic results, and factors affecting success rate after AMMR were investigated. It was hypothesized that the long-term follow-up results of this new technique were more favorable for patients with isolated meniscal injury rather than for the patients undergoing AMMR with concomitant anterior cruciate ligament reconstruction (ACLR). In order to examine this, we conducted an analysis of the MRI and clinical outcomes as well as a survival analysis at 5 years postoperatively in a consecutive series of patient who had presented for surgical treatment of meniscal lesions.
Materials and Methods
This study was approved by the Institutional Review Board of the Medical University of Poznan, Poland and was performed according to the standards in the 1964 Declaration of Helsinki. All participants provided their written, informed consent to participate in this study.
Study Design
This case series was a retrospective analysis of prospectively collected data, thus a level IV study. Data were collected in the single institutional registry dedicated to the prospective tracking of patient outcomes after the AMMR technique had been performed.
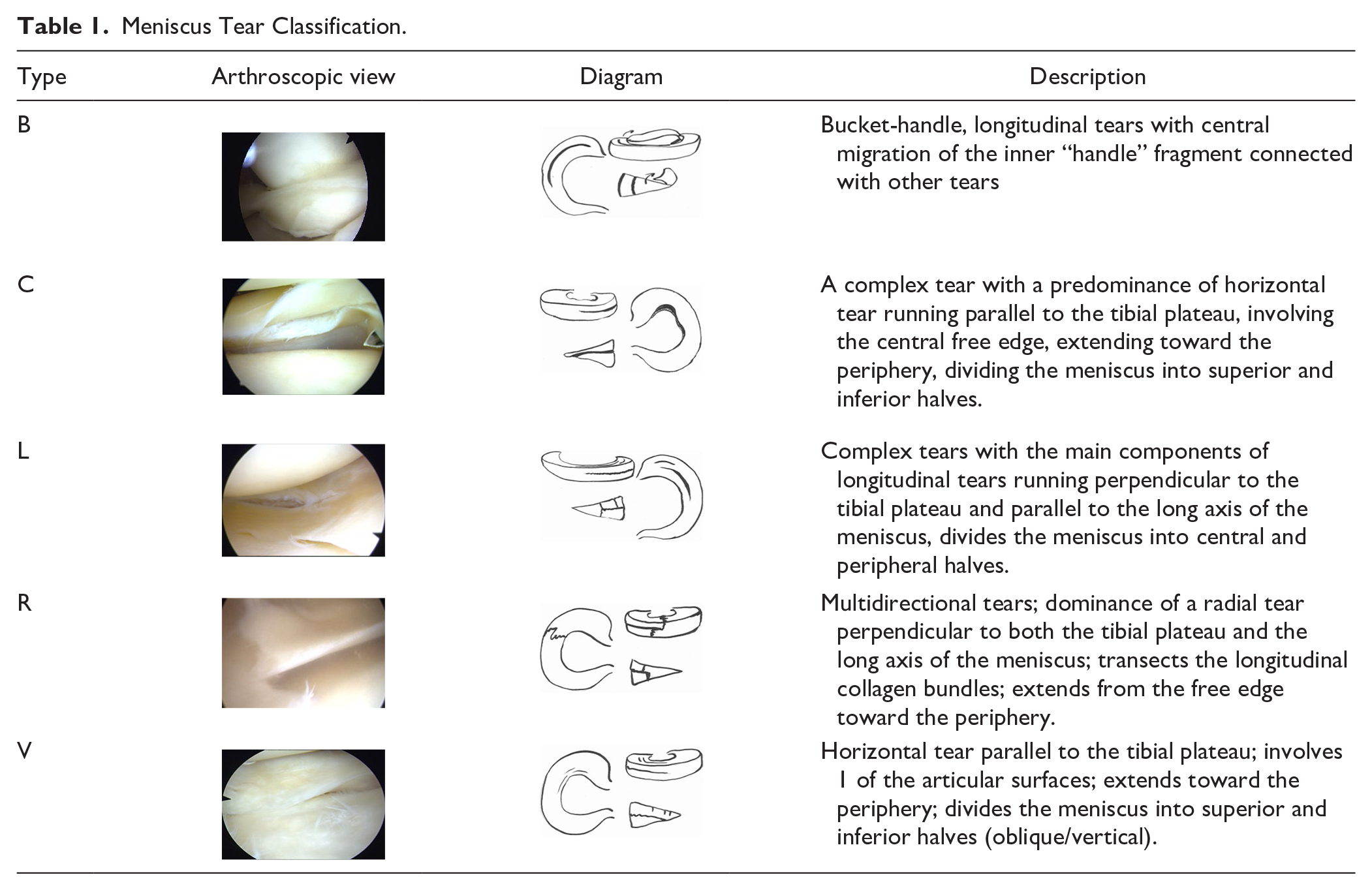
Inclusion criteria were (1) full-thickness, combined meniscal tear greater than 20 mm in length; (2) horizontal and radial tear; (3) tear location reaching more than 6 mm from the menisco-capsular junction, including the avascular zone; or (4) both degenerative and nondegenerative meniscus (i.e., horizontal and radial tears, involving the white-white and red-white zones, as well as extensive tears of the bucket-handle type). Patients were excluded if (1) full- thickness combined lesion was larger than 85% of the meniscus body or (2) a meniscal lesion with fibrillation extended to all areas and was not able to be stabilized via sutures.
Preoperative data included the time to surgery (defined as the time between either injury or patient decision to seek treatment to the date of surgery) and baseline patient-reported outcome scores. Intraoperative data included status of the articular surfaces in other compartments, meniscal status, and concomitant procedures. The length of the meniscal tear was measured during the arthroscopic procedure by using an arthroscopic ruler. Degenerative meniscus was in most cases defined as adipose degeneration or significant fibrillations not exceeding 85% body of the meniscus.
At each follow-up, outcomes were assessed by the polish version of International Knee Documentation Committee (IKDC) 10 Subjective and Clinical evaluation scores, Lysholm score, 10 and Barrett clinical criteria of meniscal healing. Based on original Barrett score, we used a converted method 7 to allow for statistical analysis. This calculation converts the 4 clinically meaningful signs (pain, effusion, clicking/locking, McMurray test) into a numerical notation. The final values (range 0-15) represent a discrete stage of the knee joint with respect to the initial Barrett’s evaluation.
The following notations were adopted for the description of the Barrett’s criteria:
Score
0. no symptoms in any of all 4 criteria
1. pain or joint-line tenderness
2. effusion
3. 1 + 2; pain or joint-line tenderness + effusion
4. clicking or locking
5. 1+4; pain or joint-line tenderness + clicking or locking
6. 2+4; effusion + clicking or locking
7. 1+2+4; pain or joint-line tenderness + effusion + clicking or locking
8. positive McMurray’s test,
9. 1+8; pain or joint-line tenderness + positive McMurray’s test,
10. 2+8; effusion + positive McMurray’s test,
11. 1+2+8; 1+8; pain or joint-line tenderness + effusion + positive McMurray’s test,
12. 4+8; clicking or locking + positive McMurray’s test,
13. 1+4+8; pain or joint-line tenderness + clicking or locking + positive McMurray’s test,
14. 2+4+8; effusion + clicking or locking + positive McMurray’s test,
15. 1+2+3+8; pain or joint-line tenderness + effusion + clicking or locking + positive McMurray’s test.
Patient satisfaction was assessed at 5-year follow-up by asking patients if they would undergo the surgery again? The quality of life (QoL) was assessed using EuroQoL (EQ-5D-5L) questionnaire.
In order to assess the influence of concomitant ACLR, we performed a subgroup analysis of patients treated with new technique for isolated meniscal injury (n = 19) and with simultaneous ACL reconstruction (n = 20). Cases with concomitant cartilage procedure or additional knee structure lesions were excluded.
Secondary outcomes included postoperative magnetic resonance imaging (MRI; 1.5-T) at 24 and 60 months.
Imaging sequences included axial T1-weighted spin-echo (SE: 700/11 [repetition time TR ms/echo time TE ms], 20 cm field of view (FOV), 5 mm/1 mm [slice thickness/interslice gap], 256 × 192 matrix, frequency encoding [FE] anterior posterior, 1 excitation), coronal T1-weighted SE (600/11, 16 cm FOV, 4 mm/0.5 mm, 256 × 192, FE superior-inferior, 2 excitations averaged), sagittal T1-weighted SE (600/11, 16 cm FOV, 4 mm/0.5 mm, 256 × 192, FE anterior-posterior, 2 excitations averaged), sagittal T2-weighted fast spin echo (FSE: 2500/90; echo train length [ETL] of 8; 14 cm FOV, 4 mm/0 mm, 256 × 192, FE superior-inferior, 2 excitations averaged) with fat suppression (frequency-selective pre-saturation), and sagittal fat-suppressed T1-weighted 3-dimensional (3D) spoiled gradient echo (FS-3DSPGR: 58/6, 40° flip angle, 14 cm FOV, 256 × 128 matrix, 60 contiguous 2-mm slices covering all articular cartilage plates in the knee, FE, superior-inferior, 1 excitation, frequency selective fat saturation, superior-inferior saturation bands to minimize pulsation artifacts).
All images were transferred to the Osirix v.5.8.5 DICOM viewer software (Pixmeo SARL, Bern, Switzerland). Images were evaluated with respect to Whole-Organ Magnetic Resonance Imaging Score (WORMS) for osteoarthritis (OA). MRI (n = 37) were assessed independently by 2 orthopedic surgeons. Readers used all images to evaluate each feature. Problematic cases were assessed by both readers at the same time in order to achieve consensus. WORMS >40 indicated presence of OA. 11 Additionally, the following pass-fail criteria were used:
If the patient underwent partial/complete meniscectomy or knee replacement after AMMR procedure, it was considered a failure.
An overall IKDC grade of A or B at final follow-up was a pass.
If the patient exhibited no pain at rest or with activity and a negative McMurray’s test, it was a pass.
Patients who did not meet these criteria were characterized as “poor” with regard to their latest clinical follow-up. Furthermore, a WORMS ≥40 was classified as a poor outcome.
Classification of Meniscus Lesions
Meniscal lesions were organized into 5 distinct types, as described in Table 1 .
Meniscus Tear Classification.
Surgical Technique
A diagnostic knee arthroscopy was made to rule out other pathology, such as lesions of ligaments and cartilage. All cartilage and ligaments lesions were repaired during surgery. The meniscus lesion was anatomically reduced and stabilized by the meniscal suture. The collagen matrix (usual size 30 × 20 mm), was fixed by Vicryl 1 (Ethicon, Johnson & Johnson S. A., Madrid, Spain) suture, passing through the surface of the matrix on either side. The matrix was than mounted on the applicator. Using direct arthroscopic vision, the collagen matrix is inserted inside of the knee joint and positioned around previously stabilized meniscus in such a manner that its smooth surface was directed to the articular surfaces and its porous part to the meniscal surface. Afterward, the matrix was fixed on the meniscus, with arthroscopic simple knotted sutures sliding on the femoral surface of the meniscus, starting from the meniscal posterior horn. As a result, the meniscus was wrapped in the collagen matrix on both sides and was fixed onto the meniscus in a stable way.
GALL-BM11/10 equipment (Gallini Medical Devices, s.p.a. Italy) was used to collect blood from the bone marrow of the proximal, tibial epiphysis. After passing through the cortical layer of the tibial bone with the use of a hammer, the internal mandrin of the cannula was removed, and a 50-mL syringe was attached to the needle. Then, approximately 5 mL of liquid bone marrow was aspirated. The entire aspirated liquid bone marrow was injected with a long needle between the matrix and the meniscus, using direct arthroscopic visualization with a technique of “dry arthroscopy.”
The surgery was completed by closing the wounds without drainage of the knee. No knee-stabilizing orthosis was used.
An extensive description of the surgical technique has been published previously. 6
Postoperative Physiotherapy Protocol
Patients began postoperative treatment from toe-touch crutch walking and range of motion exercises on the first postoperative day, for a period of 4 weeks. After 4 weeks, the patients were allowed to walk with partial weightbearing over the next 2 to 4 weeks. The patients were encouraged to return to their daily activity by 12 weeks. Sports activity was possible after 6 months postsurgery.
Statistical Methods
Numerical variables were summarized using standard descriptive statistics. Mean and standard deviation were graphed as bars and whiskers, respectively. Qualitative variables were summarized by number and frequency. The Mann-Whitney U test, Kruskal-Wallis test, and Fisher exact tests were used for nonparametric data analysis, with the Wilcoxon test used for dependent group comparison.
A logistic model was created to predict the occurrence of a good result 5 years after surgery. The criteria for individual scales were at least 84 points on the Lysholm scale, at least 76 points for IKDC Subjective, and A or B for IKDC Clinical. Classification based on WORMS was not considered due to only 1 observation indicating early OA. The following factors were introduced as independent variables: gender, age, body mass index (BMI), tear classification, group (AMMR + ACL / AMMR isolated) and preoperative values for Lysholm, IKDC Subjective, IKDC Clinical, and Barrett. The models were brought to the optimal form using the backward stepwise method.
Outcomes were analyzed by linear mixed-effect models, using time, group and their interaction as fixed effects and intercept for subjects as random effects. In addition to the models’ coefficients, intergroup comparisons were performed on basis of lsmeans. Additionally, a Kaplan-Meier test was used to analyze the survival. Significance for all statistical tests was set at 0.05. All computations were performed in R (version 3.5) with packages: lme4 i lmerTest (mixed models), lsmeans (lsmeans), survival (survival analysis), ggplot (plots).12-18
Results
Fifty-four consecutive patients, treated from 2010 to 2011, were included. The mean follow-up was 5.92 years (range 3.56-8.34 years). The patients’ inclusion in the study and the numbers analyzed are presented in Figure 1 .
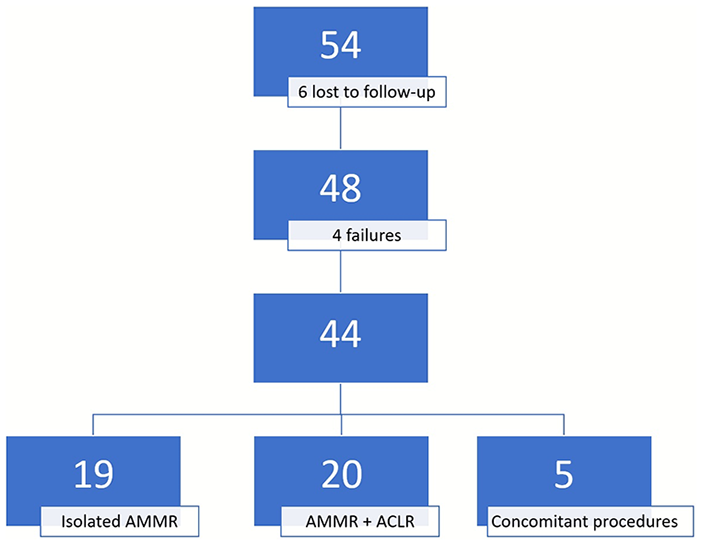
The patient inclusion in the study.
The demographics data for the study participants are summarized in Table 2 , with no significant differences noted between the subgroups. The data of 5 patients who underwent surgery for meniscal lesions concomitant with other procedures, including those for ACL, cartilage lesion, and medial patellofemoral ligament, are presented separately in Table 3 .
Patient Demographics. a .
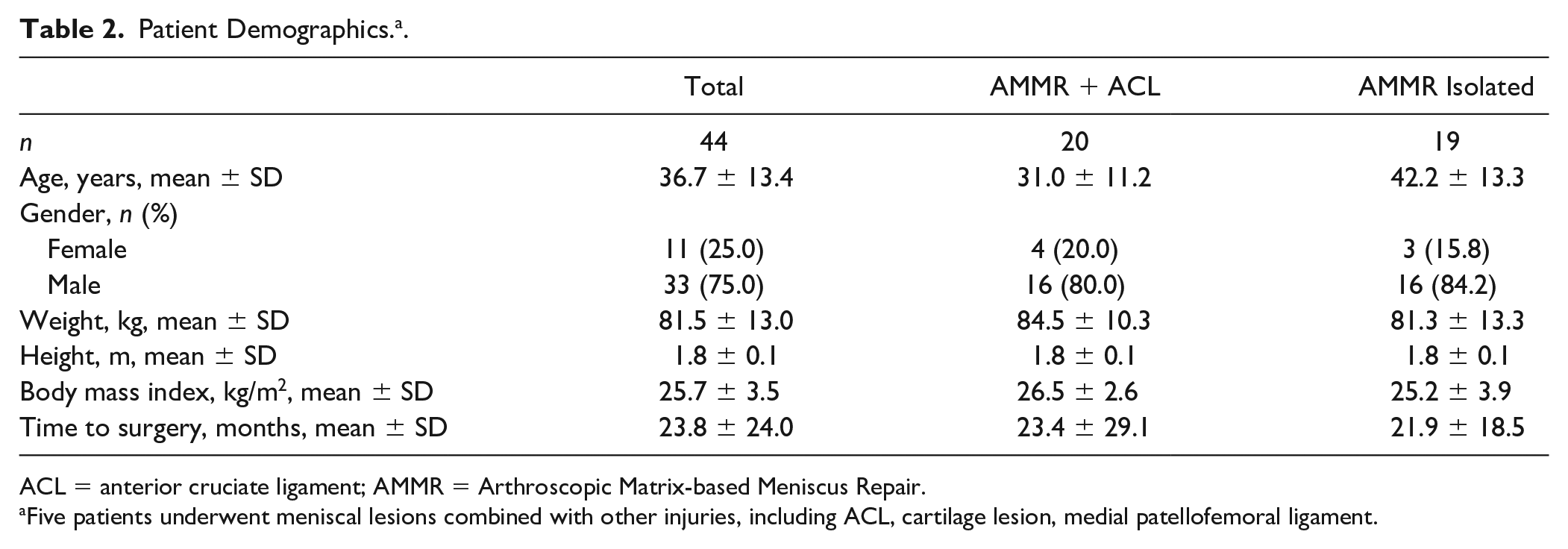
ACL = anterior cruciate ligament; AMMR = Arthroscopic Matrix-based Meniscus Repair.
Five patients underwent meniscal lesions combined with other injuries, including ACL, cartilage lesion, medial patellofemoral ligament.
The Demographic Data and Results of the 5 Patients in the Concomitant Group.
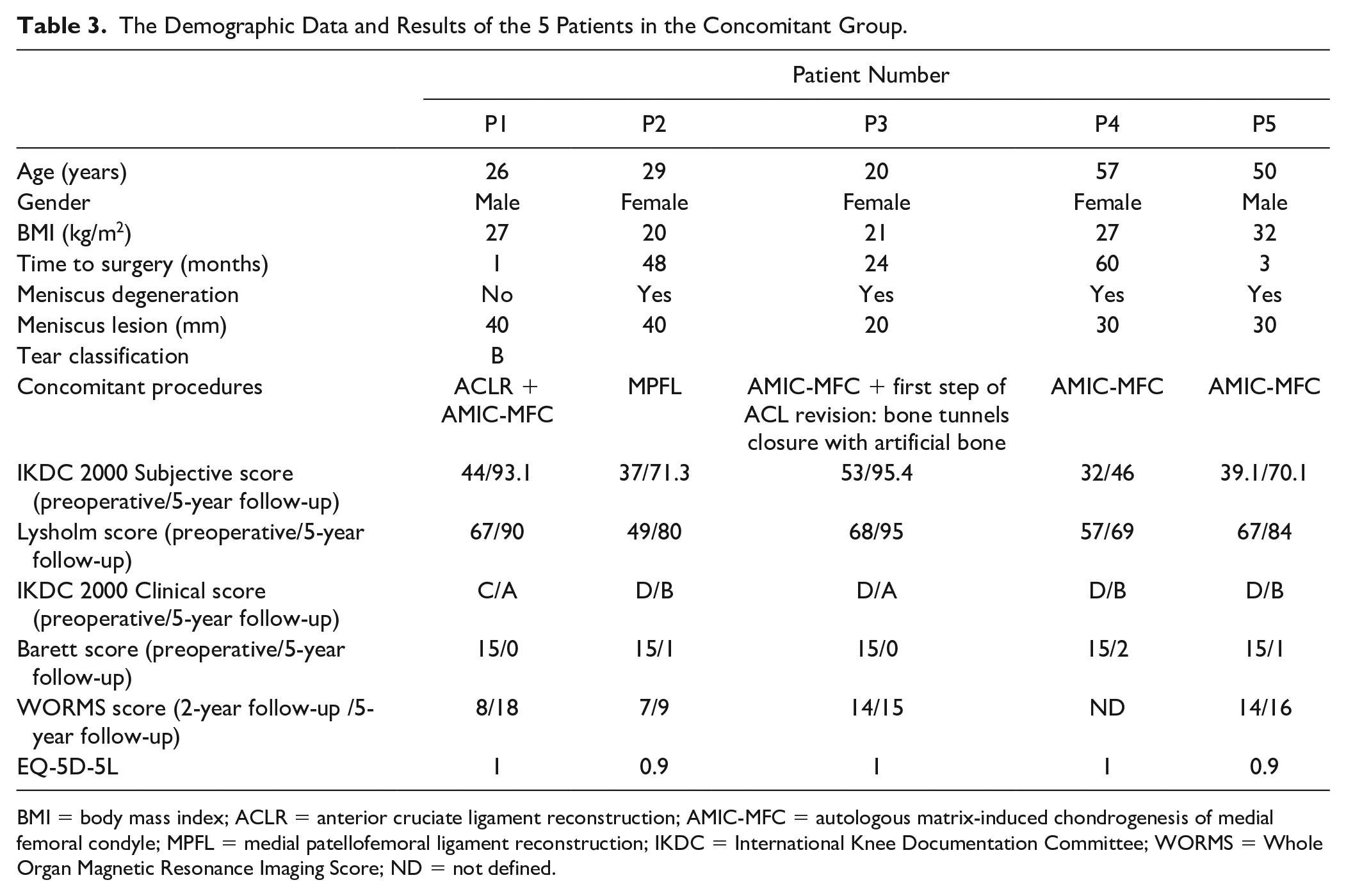
BMI = body mass index; ACLR = anterior cruciate ligament reconstruction; AMIC-MFC = autologous matrix-induced chondrogenesis of medial femoral condyle; MPFL = medial patellofemoral ligament reconstruction; IKDC = International Knee Documentation Committee; WORMS = Whole Organ Magnetic Resonance Imaging Score; ND = not defined.
The extent and type of meniscal lesion among the patients in each group is provided in Table 4 . No relationships were noted between the type of meniscal lesion and the complexity of the knee injury (ACL + meniscal tear vs. isolated meniscal tears). Meniscal degeneration was more frequent in the group of patients diagnosed with an isolated meniscal tear (Fisher exact test, P = 0.01).
Lesion Characteristics.
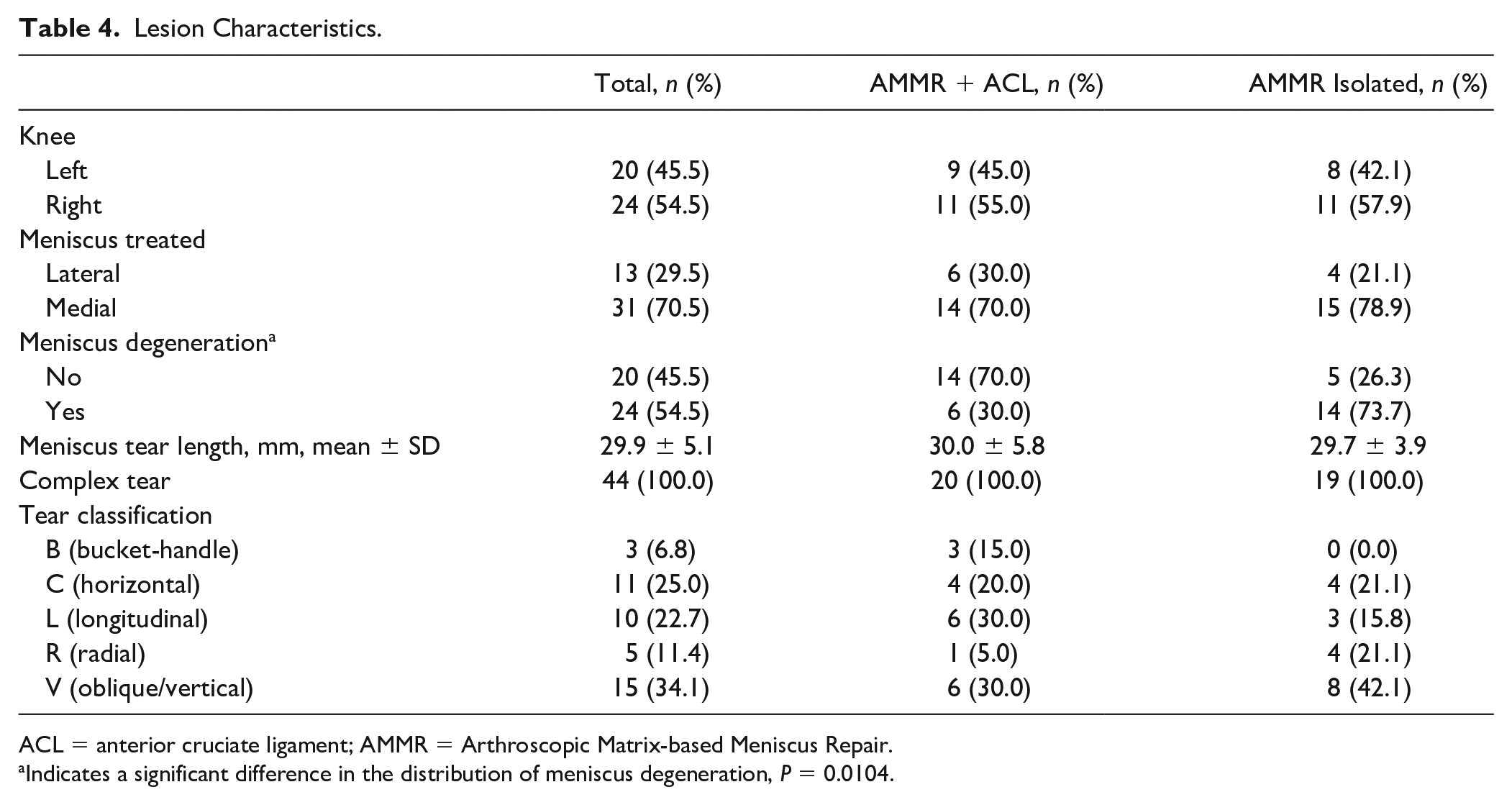
ACL = anterior cruciate ligament; AMMR = Arthroscopic Matrix-based Meniscus Repair.
Indicates a significant difference in the distribution of meniscus degeneration, P = 0.0104.
Subjective Scores
The scores for both IKDC and Lysholm increased in both subgroups over time relative to the preoperative measurement. While there was a significant difference between pre- and postoperative scores (P < 0.000), there was no difference between scores at 24 and 60 months (IKDC Subjective, P = 0.395; Lysholm, P = 0.910) (
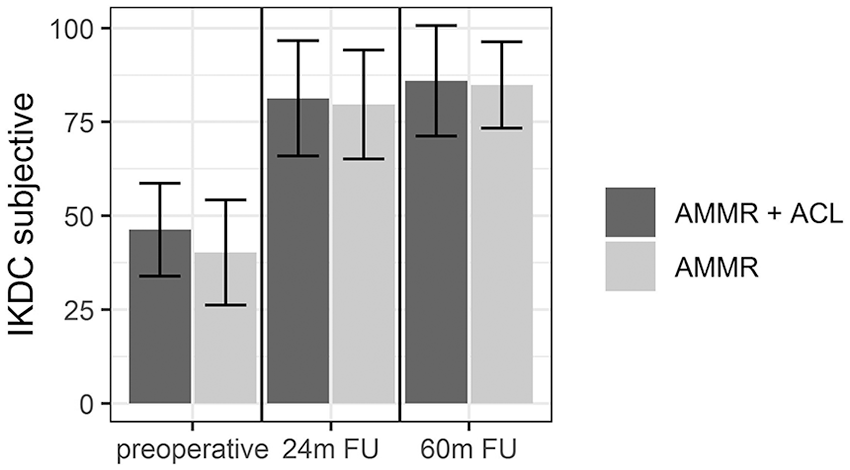
Improvement in International Knee Documentation Committee (IKDC) Subjective scores from the preoperative level to 24 and 60 months of follow-up in both groups.
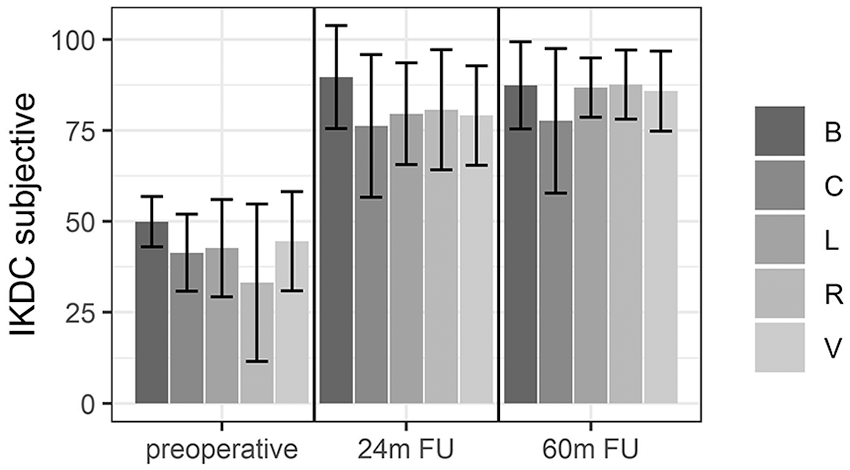
The change in the International Knee Documentation Committee (IKDC) Subjective score, separated by the type of meniscal lesion.
For the entire cohort, the Lysholm scores improved from a mean of 66.3 ± 16.4 at baseline evaluation to 88.6 ± 11.63 at 24 months and to 90.2 ± 8.7 at 60 months (P < 0.001). Similar to the IKDC, there was no difference in Lysholm scores between the 2 subgroups (
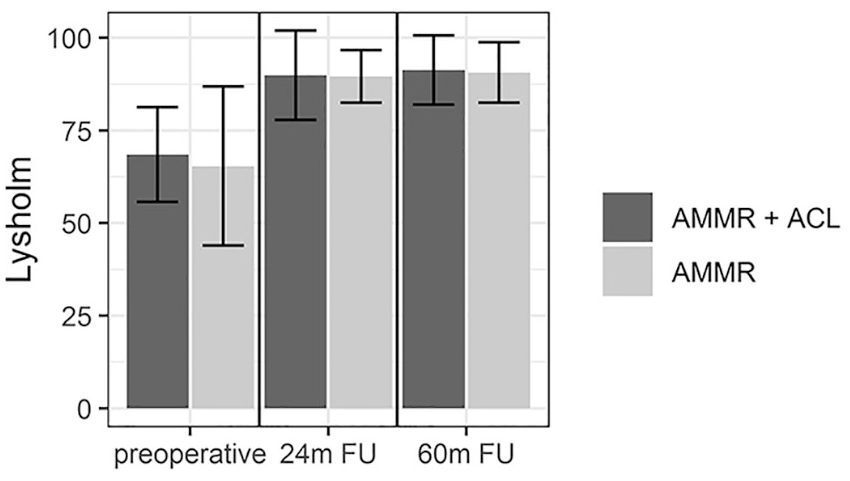
The change in the Lysholm score from the preoperative level to 24 and 60 months of follow-up. This is subdivided by the occurrence of a concomitant anterior cruciate ligament reconstruction (ACLR).
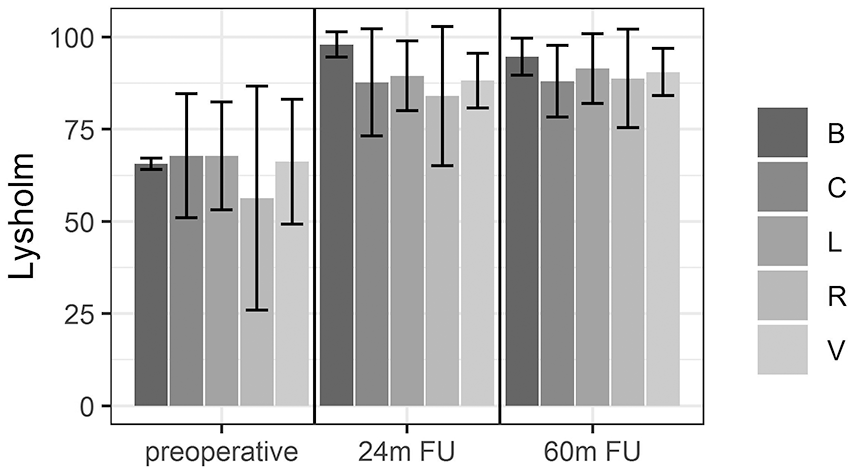
The change in the Lysholm score, separated by the type of meniscal lesion.
Clinical Assessment Scores
Using the IKDC Clinical grading system, over 80% of patients were categorized in group A at 24 and at 60 months postoperatively. At 24 months postoperatively, there were 13 and 31 patients reclassified from category C and D, respectively. At 5 years’ follow-up, there were no patients in category C or D and only 7 (18.9%) patients classified in category B ( Table 5 ). However, there was a notable loss to follow-up at the 60-month time point.
The Distribution of the International Knee Documentation Committee (IKDC) Clinical Scores When Graded Categorically.

Analysis of the Barrett criteria indicated a statistically significant difference (P < 0.000) between the groups during preoperative measurement versus follow-up (
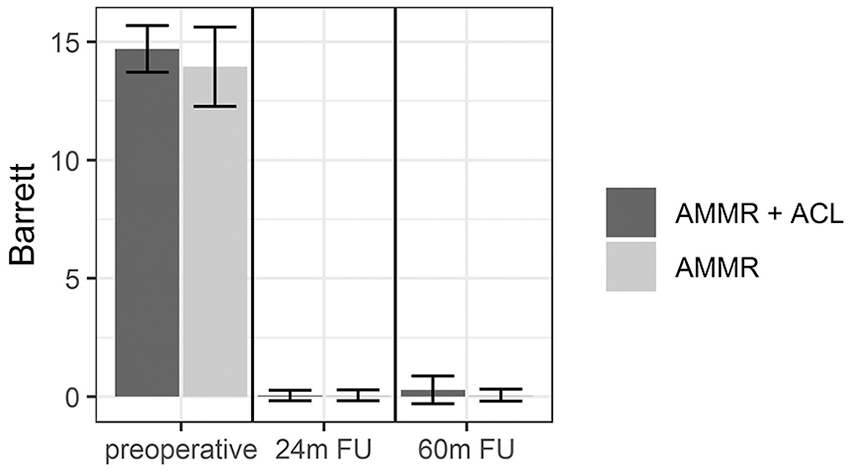
Barrett clinical score: improvement from the preoperative level to 24 and 60 months of follow-up.
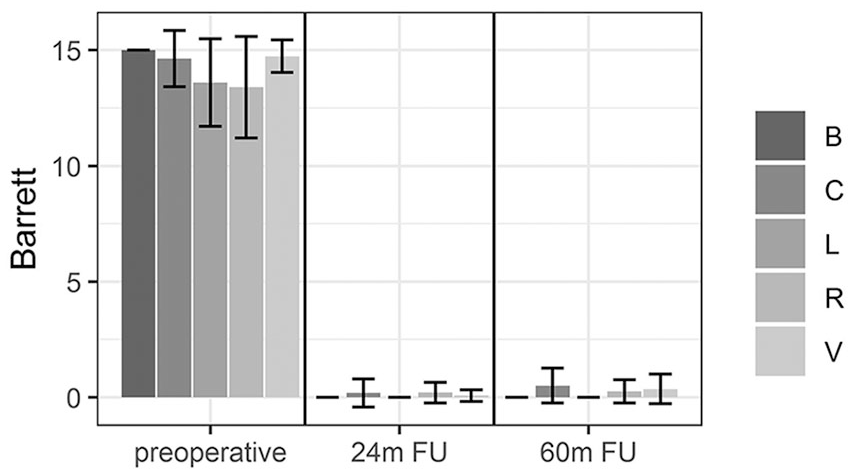
Barrett clinical score: improvement from the preoperative level to 24 and 60 months of follow-up in all meniscus tear types.
WORMS Score
Of the 44 patients for whom we had clinical data, 7 did not consent to a follow-up MRI. Overall results of postoperative MRI analysis indicated a statistically significant increase (P < 0.001) as shown in Table 6 .
Overall Scores for Whole-Organ Magnetic Resonance Imaging Score (WORMS), Where a higher Score Indicates a Worse Outcome.
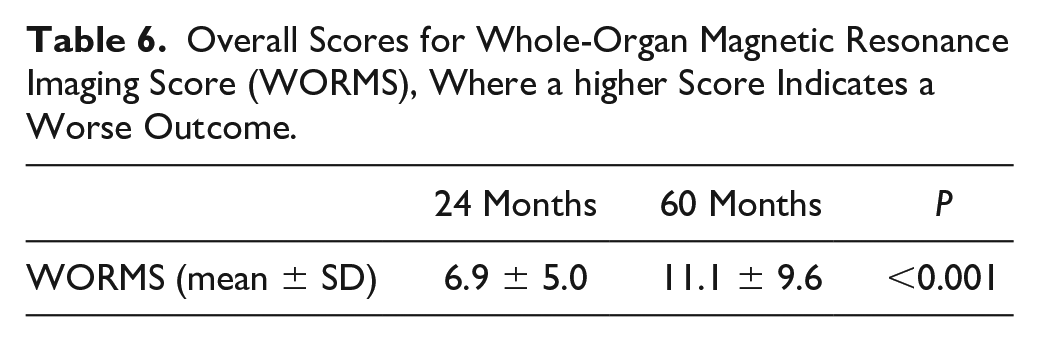
The score difference between 2- and 5-year follow-up indicates a statistically significant worsening; however, this fact is better explained when a subgroup analysis is performed. When compared between groups, WORMS increased significantly between 24 and 60 months only in the AMMR + ACL group. The difference between the groups also increased, being significant at 60 months (
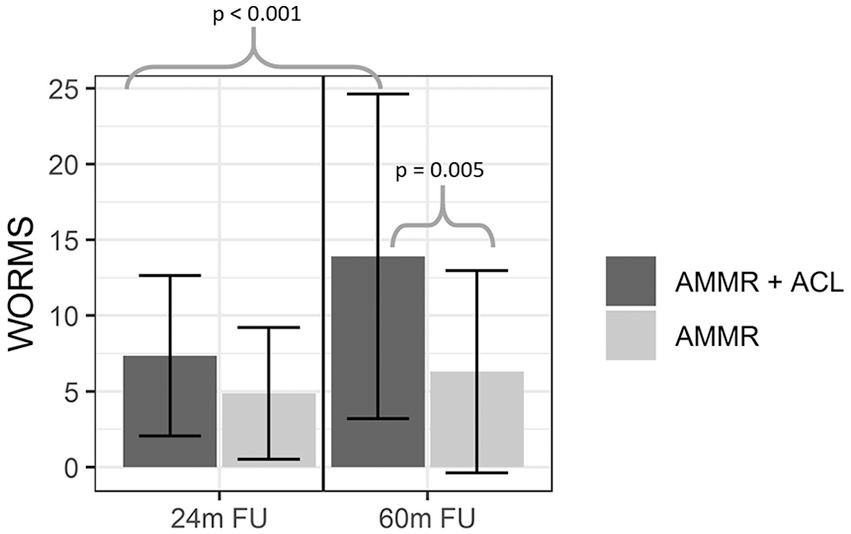
The intergroup comparisons for Whole-Organ Magnetic Resonance Imaging Score (WORMS) analysis.
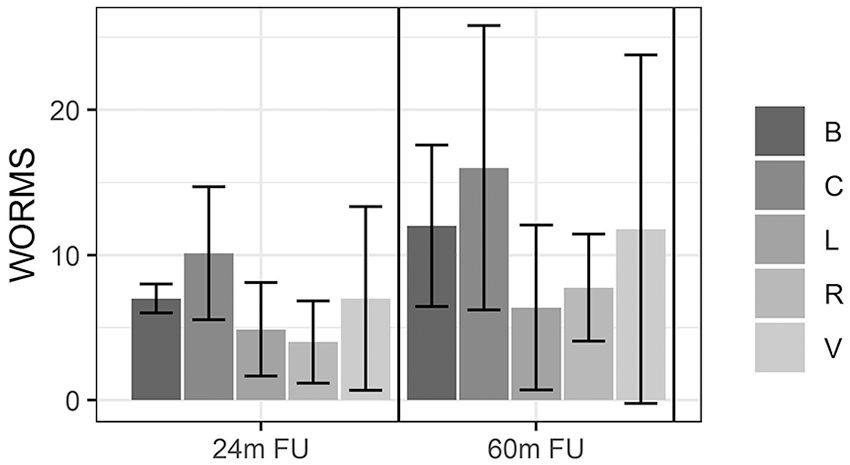
The comparisons for Whole-Organ Magnetic Resonance Imaging Score (WORMS) according to the meniscal tear type.
Predictive Factors Analysis
Unfortunately, the subjective model for IKDC was completely reduced, that is, only the free expression remained. In turn, for IKDC Clinical only the preoperative Barrett value remained in the model, but the coefficient for this variable was not statistically significant. In the model for Lysholm, the variables that remained were BMI, tear classification, and preoperative IKDC Clinical and Barrett values. Of these variables, only the BMI coefficient turned out to be statistically significant. Its value indicates that along with the increase in BMI, the chance for a good Lysholm result after 5 years increased (P = 0.023). No significant correlations were found between the type of meniscus tear and metric variables.
Patient Satisfaction and QoL
In terms of patient satisfaction, 43 patients (97.7%) responded that they would have the surgery again. The 1 unsatisfied patient said that the surgery did not meet his expectations. The patient was 49 years old and physically active, with concomitant grade III cartilage lesions. His EQ-5D-5L after 5 years follow-up was 0.828, IKDC subjective score was 64.4 (preoperative score: 41) and Lysholm score was 85 (preoperative score 80). He presented with a notable progression of degenerative changes, with WORMS of 16 at 2 years and 28 at 5-year follow-up.
We assessed QoL using the EQ-5D-5L questionnaire, and these were converted to utility values ranging from 0 (the worst possible health state) to 1 (full health). Of the 43 patients who responded, the mean score was 0.9 ± 0.1, with a range from 0.7 to 1, indicating that, in general, the patients exhibited a good QoL.
Survival Analysis
Six patients were lost to follow-up while 4 underwent arthroscopic debridement for persistent knee pain and swelling following their AMMR. These patients therefore were considered as failures (nonsurvival) based on the established pass-fail criteria. Figure 10 illustrates the Kaplan-Meier survival analysis for the patients in this study. This analysis demonstrated a survival of 88% at 5 years.
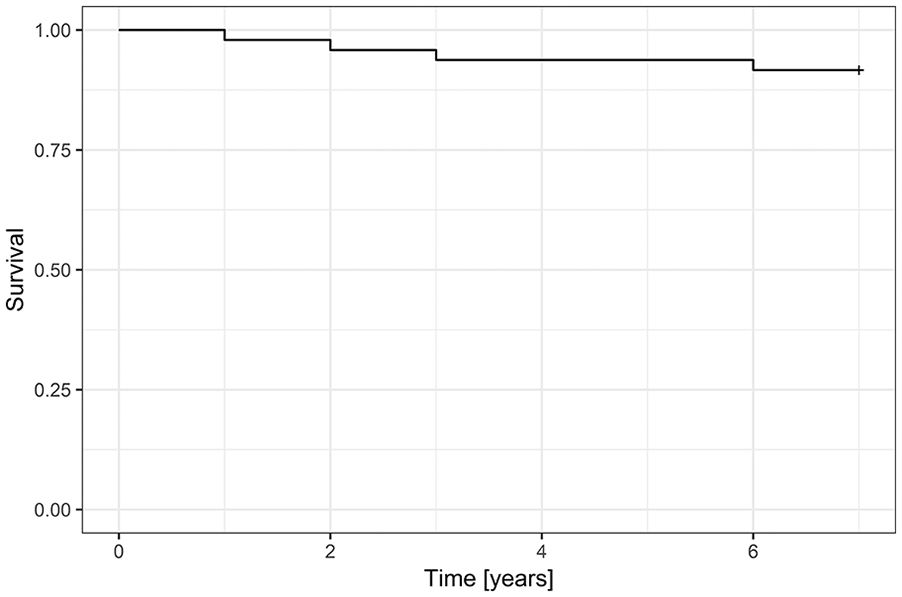
Overall survivorship as determined by clinical failure, which was defined as a secondary surgery or a Whole-Organ Magnetic Resonance Imaging Score (WORMS) score of > 40 points.
Discussion
Our study provided evidence of successful clinical outcomes after AMMR surgical treatment, with low failure rates. In addition, we have found some evidence indicating that the all-inside arthroscopic suturing of a meniscus lesion and then wrapping with a collagen membrane accompanied by bone marrow blood injection can inhibit the progression of degenerative changes in patients with isolated meniscal tears.
Reported failure rates in the general population are variable and have ranged from 5.3% 19 to 36%, 20 while a systematic review reported that meniscal repair in red-red and red-white zones exhibited a pooled failure rate of 23%. 21 We treated complex meniscus tears in the red-white and white-white zones. Usually, most, if not all, of these patients will be scheduled for meniscectomy. The failure rate of 12%, as presented in the current study, seems an acceptable clinical outcome and compares favorably to a pooled rate of failure 20.2% to 24.3%, depending on the ACL status, that was reported among studies with greater than 5-year follow-up. 21
Patient age is a controversial issue regarding its role in healing of a meniscal tear. Gobbi et al. 22 reported a higher rate of subsequent meniscectomy in patients younger than 30 years. This contrasted to reports of comparable rates of healing for younger and older patients, even for tears in the avascular middle zone of the meniscus, where healing has previously been thought to be less likely.23,24 It was also suggested that older patients tend to be less active and return to physically demanding activities at a lower and slower rate than their younger counterparts. 25 However, another publication noted that meniscal repair failure rates and patient-reported outcomes do not differ substantially between older or younger patients of similar activity level. 26 In our study, patient age influenced neither clinical nor MRI results after AMMR surgery.
It is well known that the prognosis of meniscal repairs depends on the type of meniscal tear and the presence or absence of an articular cartilage lesion. 25 However, in our series, we found no significant difference in healing rates or functional scores between various types of complex meniscal lesions. We were also unable to correlate the failure rate with clinical findings related to the meniscal injury. Based on our results, we suggest that meniscal repair in complex meniscal tear can provide good to excellent mid-term results and that tear type, size, and location should not be a relative contraindication for attempted meniscal repair by AMMR procedure.
In our study, MRI was used to detect discrete OA changes from the initial 2-year follow up to the final follow-up, because a small increase in OA severity would not be expected to be detected on a radiograph. This is consistent with previous work which has reported that caution should be used when using ordinal radiographic scales to monitor changes in knee OA severity over time. In patients who exhibit a standardized total WORMS less than 40, there is a 75% chance of a Kellgren-Lawrence grade of 0 to 1, that is, no OA. 10 In the population of our study, WORMS increased significantly between 24 and 60 months by approximately 4 points (from 6.9 to 11.1). Only 1 case reached score >40 and this was classified as early OA changes. We have also noted statistically significant differences between isolated AMMR group and AMMR with simultaneous ACLR, and this would not likely be seen on radiographs.
Meniscal repair in conjunction with ACLR has been reported to create a favorable environment for meniscal healing because of an increase in bone marrow–derived intra-articular stem cells and knee joint stability.27,28,29 Tachibana et al. 30 reported a healing rate of 74% with favorable clinical outcome, on second-look arthroscopic surgery, for meniscal repair performed concurrently with ACLR, with a 15% rate of incomplete healing and an 11% rate of nonhealing. Superior outcome after simultaneous ACL and meniscal repair versus simultaneous ACL and meniscectomy has also been reported. 31 The authors concluded that the meniscus resection in addition to ACLR resulted in worse clinical outcomes than isolated ACLR in contrast to the results seen within the meniscus repair group. 31 This would suggest that, when possible, in patients with ACL injury and meniscus tear, the meniscus repair instead meniscectomy should be performed to achieve better clinical outcome.
In our study, there was no significant difference in clinical outcome between meniscal repairs performed in isolation or concurrently with ACLR, although the low number of failures (n = 4) precluded an appropriate statistical analysis. However, in our case series, the worst WORMS assessment results were observed in patients with concomitant ACLR what would suggest faster progression of OA in this group.
Our results suggest that simultaneous ACL injury and subsequent reconstruction may be a progression factor for the OA, in spite of a meniscal repair, which is consistent with previous publications.32-34 Those authors reported that ACLR does not protect against knee structural degeneration and at 10 years post-ACLR, around 30% of patients exhibit tibiofemoral OA. Moreover, concomitant meniscal injury elevates the prevalence of tibiofemoral OA by a factor of 2 to 4 as compared to knees with isolated ACL injury.34-36 At 10-year follow-up, radiological signs of OA were present in 53.5% of the patients. The rate of OA after meniscectomy and ACLR was 64.5% in comparison with 20% in the group with isolated ACLR. 37
A long-term study, with 20 years of follow-up, had evaluated 102 knees with an intact ACL, and 93 with an unrepaired rupture. More patients with a ruptured ACL had downgraded their sport activity by 5 years after meniscectomy. The incidence of radiographic OA was 65% in patients with a ruptured ligament, and 86% in those followed-up for over 30 years. In the ligament-deficient group, 10% had undergone further surgeries due to OA, and another 28% underwent other surgeries (mainly further meniscectomies). The authors concluded that the long-term outcome after rim-preserving meniscectomy depends mainly on the state of the ACL. 38
Results observed in the ACLR group support the conclusions of recently published reviews, explaining the risk factors of OA development in patients with ACL injuries. ACL injury alone leads to increased inflammatory markers in the knee which can influence the development of knee osteoarthritis, which cannot be reversed by ACL reconstruction. Additionally, arthrokinematics, gait and other alterations in ACL-injured patients may predispose these individuals to secondary chondral and meniscal injuries. 39 Furthermore, patients presenting with ACL injuries may experience more critical injury sequelae and frequently undergo concomitant procedures. In future studies, we suggest analyzing the data from patients presenting with isolated meniscus lesions separately from those suffering from combined ACL and meniscal injuries.
To our knowledge, this is the first study that has assessed patient satisfaction and quality of life in the medium term after AMMR for complex meniscal tears. These data might be of importance for future analyses of cost and clinical effectiveness. The QoL reported by the participants in this study, 5 to 8 years after the procedure, was very good.
The limitations of our study need to be acknowledged. These include a relatively small number of patients. The retrospective analyses of prospectively collected data design of our study is an inherent weakness. There were no preoperative MRI available for this patient population, and changes in outcome scores were able to be assessed only at 2-year and 5- to 8-year follow-up visits. We were not able to assess meniscus healing status. Our study cohort included only patients treated in single clinic by single surgeon. While all patients underwent the same meniscal repair procedure there were different concomitant procedures including ACLR and AMIC cartilage regeneration in various configurations and combinations, which were decided on a case-by-case basis. Additionally, there was some loss to follow-up, and patients lost to follow-up can bias estimates of failure rates or patient-reported outcome scores.
Despite these limitations, our study focused specifically on clinical and MRI-based outcomes of a treatment (AMMR) that can provide a viable alternative to meniscectomy. It was possible to assess the effect of simultaneous ACLR on outcomes, both clinical and MRI, and the data showed an 88% success rate at 5 to 8 years’ follow-up. In addition, patient satisfaction with their knee function and QoL demonstrated very high patient satisfaction measured 5 or more years postoperatively. Given all our results, we suggest that meniscal repair in this population can render good to excellent medium-term results and that tear size and location should not be a relative contraindication to attempted repair. In addition, tear complexity did not affect clinical outcome.
Conclusion
As an alternative to meniscectomy, AMMR enabled meniscus preservation and demonstrated very good mid-term clinical, patient-reported and MRI-based outcomes, as well as a favorable survival rate after the all-inside technique of arthroscopic suture of meniscus and wrapping with a collagen membrane with bone marrow blood injection. Although patients with simultaneous ACLR and meniscal lesions showed an improvement in all scoring systems, they are likely to be predisposed to OA progression.
Footnotes
Authors’ Note
The work reported was done in Rehasport Clinic, Poznań, Poland.
Acknowledgments and Funding
The authors thank Miss Barbara Gorzawska, Joanna Smieja, and the Biostat Company Team for their untiring help in statistical data analysis. The application of Chondro-Gide matrix described in this paper was not CE marked or FDA cleared at the time of the surgery. The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Geistlich Pharma AG: (1) The authors received collagen matrix from Geistlich Pharma AG free of charge and (2) Geistlich Pharma AG provided financial support for data collection and study monitoring performed by a third party.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: T.P. occasionally receives payment as trainer of arthroscopy from Smith & Nephew and Arthrex and payment for lectures from Geistlich.
Ethical Approval
This study was approved by the Institutional Review Board of the Medical University of Poznan, Poland and was performed according to the standards in the 1964 Declaration of Helsinki.
Informed Consent
All participants provided their written, informed consent to participate in this study.
Trial Registration
Not applicable.