
Abstract
Objective:
Studies have shown that meniscal repairs have better outcomes over both partial and total meniscectomies. Tissue engineering strategies to repair meniscus tears have been explored using cell sources that involve a donor as well as a period of in vitro cell expansion before use. This study explored cell sources that could be easily harvested and rapidly isolated by enzymatic digestion and cannulated delivery.
Methods:
Bovine menisci were used to create a bucket handle tear. Cell lines were established from meniscus, synovium, and adipose tissue and fluorescently labeled. At passages P2, P4, and P8, cells were added to the defect from the following experimental groups: cells alone, collagen gel, collagen scaffold, or hyaluronic acid. Menisci constructs were xenografted subcutaneously onto the dorsum of athymic rats and incubated for 3, 6, and 9 weeks, at which time they were retrieved and processed for histology.
Results:
Meniscal cells were able to repair defects faster and significantly better than adipose or synovium derived cells. Adipose cells were the least effective in comparison. Repair was significantly better at 9 weeks compared with 6 and 3 weeks. Macroscopic examination of menisci that received cell implants showed the thickest tissue in menisci that had collagen implants, and the thinnest fill occurred in menisci treated with cells alone. Histology confirmed no cells or integrative repair in the control specimens.
Conclusions:
Delivery of cells alone outperformed the additional use of biomaterials. Our results suggest a strategy that would use both meniscus and synovial cells for arthroscopic meniscal repair.
Introduction
The meniscus plays a vital role in knee joint mechanics, including force transmission, shock absorption, joint stability, lubrication, and proprioception. Meniscus injuries remain a difficult challenge in orthopedics, particularly with lesions located in the inner-most avascular regions, because research has repeatedly shown that avascular tears of the meniscus do not heal adequately.1-7 Capillaries from the lateral and medial geniculate arteries only penetrate peripherally to a depth of 10% to 30% of the width of the medial meniscus and only 10% to 25% of the width of the lateral meniscus. 8 Meniscal fibrochondrocytes also lack sufficient scaffolding in which to mount effective wound repair. 9
Orthopedic surgeons commonly perform meniscectomies when treating torn menisci by simply debriding torn meniscal tissue. However, studies have shown that meniscal repairs have better outcomes over meniscectomies and that resection of the meniscus can predispose the knee joint to degenerative changes.10,11 Successful surgical restoration of damaged menisci has always been a challenge to the orthopedic surgeon. Numerous strategies to repair and replace meniscus have achieved only limited success. 11 A number of different surgical procedures are available to achieve stabilization of the defect, such as staples and arrows. A number of techniques have also been described to repair menisci, such as inside-out, outside-in, or all-inside suturing techniques. 8 These procedures frequently do not produce an integrative, functional repair. 12 In the past, complete excision of the injured meniscus was used, but found to result in early onset of osteoarthritis.2,13 At present, the most common surgical approach is arthroscopic examination and adequate partial menisectomy of the injured portion of the meniscus.13-17 However, the patient is potentially subjected to a chronic course of degenerative changes secondary to altered biomechanics.
The utility of applying principles of tissue engineering to meniscus tears has been explored in several reports in the literature.11,18,19 These have generally been successful in bridging clinically relevant meniscus lesions with mechanically stable repairs. The cell source in most of these studies have involved both meniscal cells themselves as well as other potential allogeneic cell sources such as articular cartilage, auricular cartilage, and marrow stromal cells. All these cell sources involve a donor as well as a period of in vitro cell expansion before they can be introduced into meniscus defects.
Tissue engineering combines the technologies of cell culture and biodegradable scaffolds to deliver a cellular repair, and may hold one future answer to the problem of meniscus healing. The concept of using cell-based repair for torn menisci could improve the healing of lesions in the avascular zone and broadly expand the indication for repair rather than removal, obviating the need for meniscectomy. 18 The use of cells and cell constructs for promoting meniscus repair has been investigated with some success.11,19
The purpose of the present study was to explore cell sources that could, in principle, be easily harvested in a reasonably rapid time frame by enzymatic digestion and cannulated delivery. In this study, we chose synovial derived cells and adipose derived cells because of their ease of utility for the proposed application, and compared them to meniscus cells as a benchmark standard. We also looked at several methods to deliver the cells that could be adapted for use by arthroscopic methods including fibrillar scaffolds and hydrogels. Furthermore, we also studied the effect of cell doubling in vitro in order to determine if these cells could not only be applied to a perioperative time frame but could possibly be stable in vitro for a period of time, and thus have utility as an expanded population capable of multiple patient use.
Methods
Cell Isolation and Culture
Meniscus Cell Isolation and Culture
Meniscal fibrochondrocyte cell lines were established from adult bovine knee joints following the dissection and harvest of menisci. Meniscal tissue was minced into pieces approximately 1 to 2 mm3 under sterile conditions. The tissue was then washed twice with culture medium and then weighed. The tissue was then digested overnight in a 0.2% collagenase solution under constant stirring at 37°C. The cell suspension was subsequently filtered through a 100-µm cell strainer to separate any undigested material, and then centrifuged for 10 minutes at 1,300 rpm. The pellet was resuspended in culture medium and counted. Cells were then plated in culture with complete medium (DMEM with 10% fetal bovine serum) at a density of 10,000 cells/cm2. Culture was continued at 37°C, 5% CO2, and 95% humidity until use.
Adipose and Synovial Derived Cell Isolation and Culture
Synovial and adipose tissue were harvested from bovine knee joints by careful dissection and biopsy of the identified tissue types. The tissue was weighed and preheated medium at 37°C. DMEM (Walkersville MD) was added to the Petri dishes to avoid dehydration. The tissues were then washed several times and then minced with a sterile pair of tweezers and a sterile scalpel. The minced tissue was transferred to a sterile tube containing 10 mL DMEM with antibiotic (DMEM-AB). A 0.4% collagenase solution in DMEM-AB was prepared with 15 mL digestion medium per gram of biopsy material. After passing through a sterile filter, the collagenase solution was added to the minced tissue. Four-millimeter sterile borosilicate beads were then added to the minced tissue (3 mL glass beads/tube). The tube was then placed in a vertical rotor and allowed to digest for 4 hours at 37°C. The vertical rotor was employed to increase the shear stress within the tube. After digestion, the cell suspension was sieved through a 100-µm cell strainer and subsequently through a 70-µm cell strainer. Undigested pieces of tissue were discarded. The cell suspension was centrifuged at 1,500 rpm for 10 minutes, counted, and plated in culture at a density of 10,000 cells/cm2. Culture was continued at 37°C, 5% CO2, and 95% humidity until use.
Scaffolds Utilized
In addition to using cells alone, the following biomaterial scaffolds were employed as cell delivery vehicles:
Collagen gel: High-density collagen gel (Nutragen 6 mg/mL; Advanced Biomatrix, San Diego, CA) was prepared according to the manufacturer’s specifications. Briefly, acid collagen solution was neutralized with 0.1 M NaOH and kept on ice until cell mixing (100,000 cells/10 µL). The cell-collagen gel mixture was then pipetted directly into the meniscus defect and allowed to polymerize for 10 minutes at 37°C.
Collagen scaffold: Type I fibrous collagen scaffold (Kensey-Nash, Exton, PA), 2-mm thick type I collagen scaffolds were seeded with cells (106 cells/0.5 cm2) just prior to surgical implantation. The collagen scaffold was then cut to fit the meniscal defect and inserted into the defect site.
Hyaluronic acid (HA): High-molecular weight HA of approximately 4 kDa molecular weight (A gift from Dr. Phillip Band, New York University) was used as a carrier to deliver cells. Cells were mixed with HA at 100,000 cells/10 µL prior to implantation and injected into the meniscus defect site.
Cell Labeling
Cells were pulsed for long-term staining during the log phase of in vitro growth with CellTracker Green (Lonza, Walkersville, MD) for subsequent localization studies. Following cell attachment before each scheduled passage, cells were rinsed of medium and replaced with prewarmed media containing the cell tracker probe (10 µM) for 45 minutes. The probe solution was replaced with prewarmed media for another 30 minutes before further manipulation. After fixation of tissue samples and processing for histology (described below), slides were viewed on an Olympus OM-2 microscope with epiflourescent capability.
Preparation of Meniscus Xenografts
Menisci were harvested from bovine knee joints and cut into 1.5-cm radical segments. A bucket handle tear was created using a scalpel and either left empty, filled with a cell graft as described above, or filled with a cell biomaterial construct and closed with a nylon 6-0 suture. Menisci were wrapped in a nytex screen to exclude host cells, and then 4 menisci constructs were xenografted subcutaneously onto the dorsum of each athymic rat (350-400 g) and incubated in vivo for 3, 6, and 9 weeks, at which time they were retrieved and processed for histology.
Experimental Design
Cells prepared from the 3 different tissue compartments—meniscus, synovium, and adipose tissue—and cultured as described above. At specific cell passage numbers of P2, P4, and P8, the cells were trypsinized, washed, pelleted, and allocated to one of the following experimental groups: (a) cells alone, pipetted directly into the previously created meniscus defects (typical volume was 20-40 µL containing 2-3 million cells); (b) collagen gel; (c) collagen scaffold; or (d) hyaluronic acid. Meniscus defects that were left untreated served as the control group. The various meniscus xenograft groups were implanted as described above for 3, 6, and 9 weeks.
Histological Preparation and Analysis
Rats were sacrificed at 3, 6, and 9 weeks postimplantation. Samples were harvested and examined macroscopically for evidence of healing and then fixed in 10% buffered formalin. Samples were then dehydrated and embedded in paraffin. Five-micrometer-thick sections were either stained with hematoxylin and eosin or Mallory’s trichrome stain. Unstained sections were examined with a fluorescent microscopy to localize cells within the defect. To evaluate the degree of repair in each of the groups, we used a scoring system similar to those used in scoring tendon repair. The scale ranged from 0 to 4 with the following characteristics:
0: No healing observed, empty void space with defect clearly present
1: Minimal healing present with some integrative repair observed on one or both sides of the defect
2: Moderate healing observed with 25% to 50% integration of the surrounding tissue present
3: Abundant healing present 50% to 75% integration present
4: Healing nearly complete with full (>75%) integration observed
Each specimen was independently evaluated by 2 blinded observers and a minimum of 20 fields and 10 sections were scored.
Results
Cell Culture
All the cell types used were easily cultured and displayed a typical fibroblastoid appearance in monolayer culture. The rate of the cell growth was similar for adipose and synovial cells, whereas meniscus cells were slower by 1 to 2 days before needing to be passaged.
Control Meniscus
Following tissue retrieval, the bovine meniscus implants were grossly examined and then bisected through the central region of the created tear. These specimens were primarily characterized as containing a conspicuous gap in the central region of the defect with no healing observed. The gap was easily distracted by minimal force with surgical forceps. In 4 meniscal implants some minimal reduction in gapping could be found in the peripheral margins of the defect only, but never in the central region. Histological evaluation by a blinded observer confirmed no cells or integrative repair taking place in any of the control specimens (Fig. 1A-C). There was also a lack of host cell migration from the meniscus outward in an attempt to heal the defect. There was also no infiltration of host cells present from the nude rat host. None of the scaffolds or other delivery systems investigated resulted in any repair over just suture alone. Collagen scaffold material was observed in the gap in those specimens treated with scaffold alone, but lacking any cellular infiltration from the host meniscal cells.
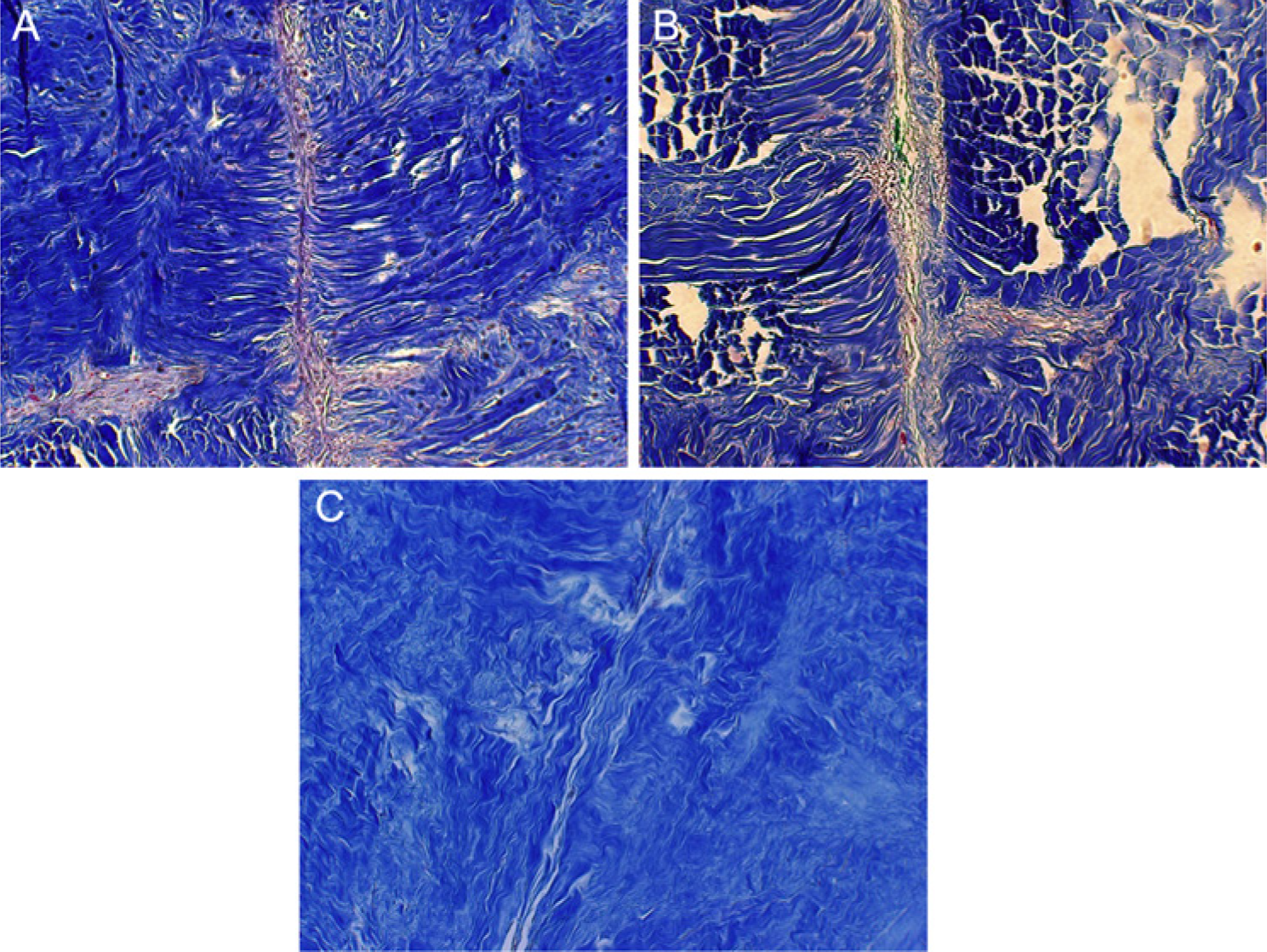
Photomicrograph of control meniscus demonstrating conspicuous persistence of defect, unhealed at 3, 6, and 9 weeks post implantation (
Experimentally Treated Meniscus
Macroscopic examination of harvested menisci that received cell implants regardless of scaffold type all demonstrated closure of the lesion with varying degrees of new filling. The thickness of the tissue filling the lesion gap was dependent on the type of scaffold implanted. The thickest tissue fill was observed in menisci that had received collagen implants. The thinnest tissue fill occurred in menisci treated with cells alone ( Fig. 2 ). Gross mechanical assessment of the strength of the repair site demonstrated adhesion that was not separated under moderate distraction by forceps. The strength of the bond also continued to improve with time in vivo. All menisci were prepared for histological examination and scored for their ability to bridge the gap defect with new tissue and synthesize collagen into the extracellular space. There was general trend of better healing with time; thus, repair was significantly better at 9 weeks compared with repair at 3 and 6 weeks.
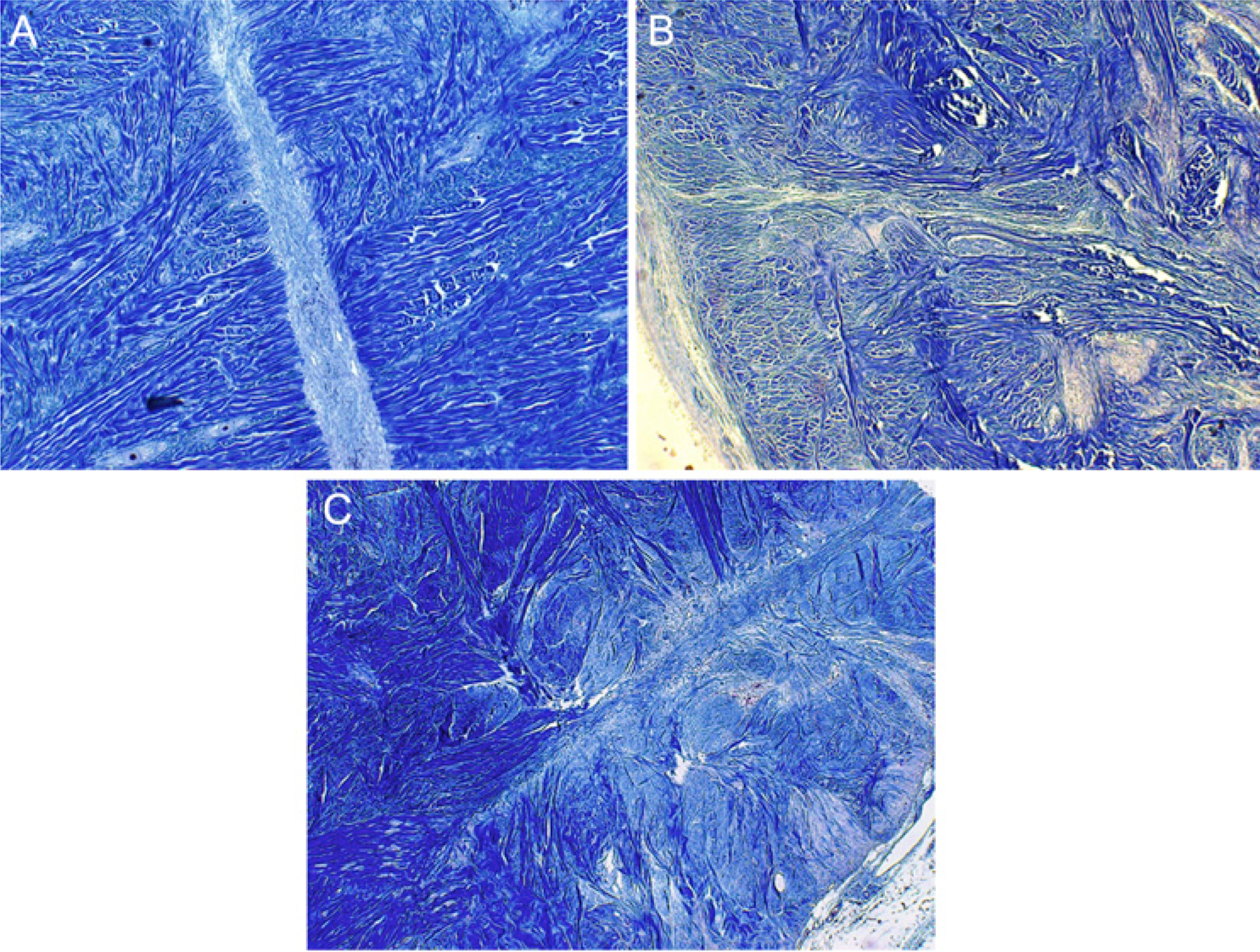
Photomicrograph of experimentally repaired meniscus with meniscal fibrochondrocytes. Note the integrative repair present by 9 weeks (
Cell Labeling
Localization of cells by fluorescence microscopy was observed in all experimental groups that received cell transplants( Fig. 3 ). The number of cells did not decline with time as the 9-week group demonstrated highly positively labeled cells still within the defect site. The cells in all groups remained localized within their respective defect or carrier material and did not migrate into the host meniscus tissue to any large degree.
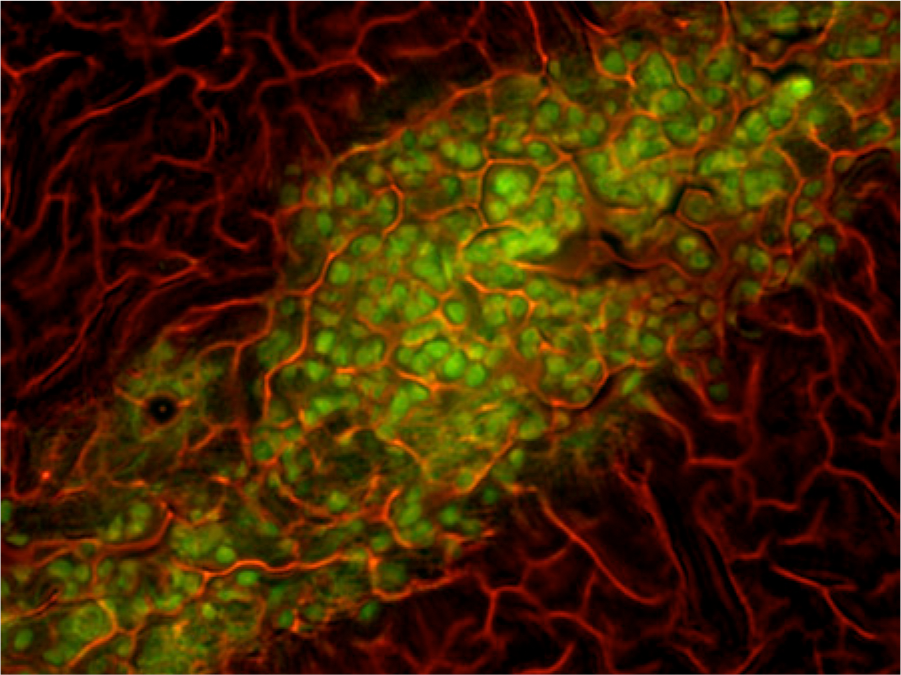
Photomicrograph of implanted labeled synovial cells in defect under fluorescent optics at 200× magnification demonstrating original source of cells are from the transplanted population and their survival in vivo for 9 weeks.
Effect of Scaffold
Meniscal repair in the cells alone group resulted in superior repair independent of tissue of origin when compared with the addition of scaffolds. The group with the next highest rate of repair was collagen gel, followed by the use of collagen scaffold. Hyaluronic acid was the least effective of the scaffolds tested.
Effect of Cell Passage Number
There was no significant trend observed with respect to passage number regardless of cell type tested in their ability to bridge the experimental gap defect created. However, there was a subjective improvement in repair observed with cells that were in the early passage (p2 and p4) compared with later passage cells (p8). These observations were performed with the cells only group exclusive of the addition of a scaffold.
Effect of Cell Type
In comparing the cells with respect to tissue of origin, cells derived from menisci were able to repair defects faster and with more collagen than adipose or synovium derived cells. Adipose cells were the least effective in comparison. Synovial derived cells demonstrated a mixed capacity for cell-based repair.
Histological Grading
For cells alone, the mean histological scores for adipose, synovial, and meniscal groups were 1.55, 1.64, and 1.94, respectively ( Fig. 4 ). A significant difference was found between the group means as determined by one-way ANOVA (P = 0.003). A post hoc Tukey HSD test showed that there was a significant difference between the meniscus and adipose derived cell groups (P = 0.016) and the meniscus and synovium derived cell groups (P = 0.017). There was no significant difference between the adipose and synovium derived cell groups (P = 0.817). For the different time points, the mean histological scores for the 3-week, 6-week, and 9-week groups were 1.33, 1.27, and 2.82, respectively ( Fig. 5 ). A significant difference was found between the group means as determined by one-way ANOVA (P < 0.001). A post hoc Tukey HSD test showed that there was a significant difference between the 9-week and 3-week groups (P < 0.001) and the 9-week and 6-week groups (P < 0.001). There was no significant difference between the 6-week and 3-week groups (P = 0.871).
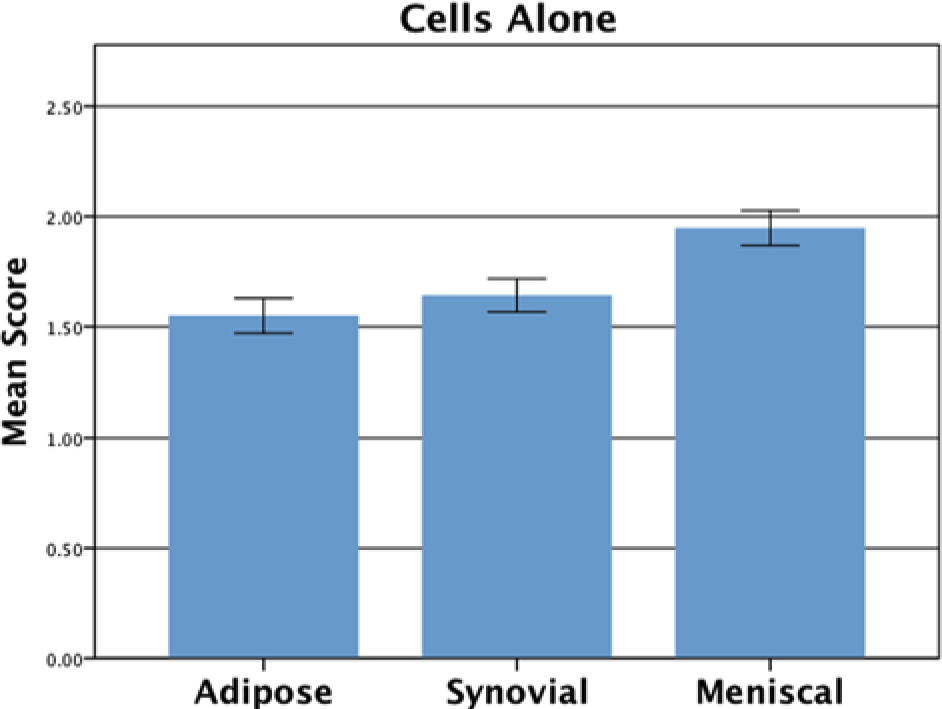
Histological scoring comparing the different cell types: adipose = 1.55, synovial = 1.64, and meniscal = 1.94.
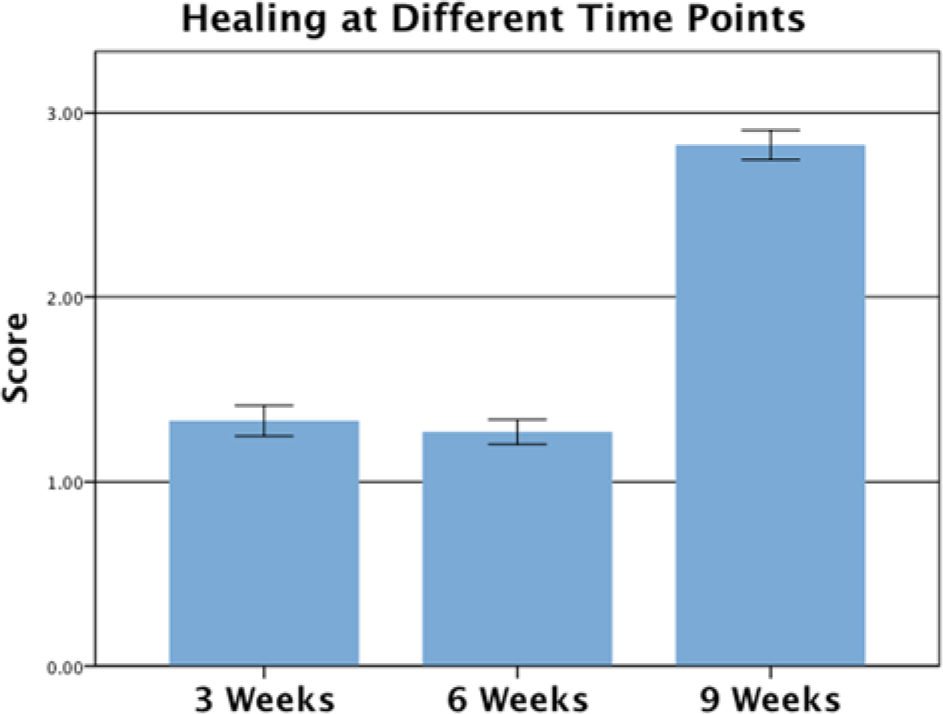
Histological scoring of meniscal cells with respect to time in vivo postimplantation: 3 weeks = 1.33, 6 weeks = 1.27, and 9 weeks = 2.82.
Discussion
King provided evidence that menisci will have a varied response to injury. 2 From this early knowledge, intense debate and research have advanced efforts to repair and regenerate the meniscus. The meniscus is considered a vital tissue that imparts load-bearing properties, supplies nutrients, and provides crucial joint stability to preserve joint biomechanics.1,2,11 Any loss or disruption of the meniscus may lead to irreversible degeneration of the articular cartilage. Injuries to the meniscus often do not heal well and currently available treatments are less than ideal. There is therefore a need for novel methods to repair the meniscus and prevent the onset of degenerative changes.
This study evaluated several cell-based strategies for repairing meniscal lesions. We sought to systematically determine the best cell type to use for clinical application, the effect of passage number on reparative capacity, and various delivery materials to augment meniscus repair. Our results demonstrate that delivery of cells alone outperformed the additional use of biomaterials. This was surprising because we hypothesized that the adjunct use of a scaffold would better retain the transplanted cells within the defect and serve as a network to more quickly immobilize recently synthesized collagen. The opposite finding was observed; scaffold materials impaired, depending on the type of material, the ability to biologically “weld” the defect sides.
The nude rat offers the potential to use xenografts to study integrative repair. This model also allows a large meniscus specimen to be studied and is more cost effective than studies with large animal models. However, the lack of mechanical load normally associated with weightbearing knee motion is a significant limitation of the nude rat model. 20 Thus, the athymic rat model is useful as an initial screening system, but studies of new interventions eventually need to be conducted in a large animal model so that effects of weightbearing can be fully evaluated.
Our results are consistent with other similar studies by Perretti et al. and collaborators,21,22 who also studied cell-based repair of meniscus using various approaches. Based on their successful findings with both autologous as well as allogeneic sources of cells, it is possible to envision a strategy that would be able to bank both meniscus and synovial cells for arthroscopic meniscal repair.
Although the biomechanics of repaired menisci were not evaluated in this study, our microscopic results suggest that a similar level of material properties obtained in earlier studies by our group was achieved. 23 To our knowledge, this is the first study to evaluate and compare different combinations of cell types, tissue culture passage number, and biomaterial carriers for their effect on meniscus repair.
Footnotes
Ethical Approval
All animal work was approved by the Feinstein inst’s IACUC before commencing any animal experimentation. All PHS guidelines for the ethical care and treatment of animals were strictly adhered to.
Acknowledgments and Funding
Hyaluronic acid was kindly provided by Dr. Phillip Band, New York University, New York. The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.